
Abstract
A central goal of the Academy of Breastfeeding Medicine is the development of clinical protocols for managing common medical problems that may impact breastfeeding success. These protocols serve only as guidelines for the care of breastfeeding mothers and infants and do not delineate an exclusive course of treatment or serve as standards of medical care. Variations in treatment may be appropriate according to the needs of an individual patient. The Academy of Breastfeeding Medicine recognizes that not all lactating individuals identify as women. Using gender-inclusive language, however, is not possible in all languages and all countries and for all readers. The position of the Academy of Breastfeeding Medicine (https://doi.org/10.1089/bfm.2021.29188.abm) is to interpret clinical protocols within the framework of inclusivity of all breastfeeding, chestfeeding, and human milk-feeding individuals.
Introduction
Mastitis is a common maternal complication of lactation and contributes to early cessation of breastfeeding. 1 In the past, mastitis has been regarded as a single pathological entity in the lactating breast. 2 However, scientific evidence now demonstrates that mastitis encompasses a spectrum of conditions resulting from ductal inflammation and stromal edema (Fig. 1). If ductal narrowing and alveolar congestion are worsened by overstimulation of milk production, then inflammatory mastitis can develop, and acute bacterial mastitis may follow (Fig. 2). This can progress to phlegmon or abscess, particularly in the setting of tissue trauma from aggressive breast massage. Galactoceles, which can result from unresolved hyperlactation, can become infected. Subacute mastitis occurs in the setting of chronic mammary dysbiosis, with bacterial biofilms narrowing ductal lumens.
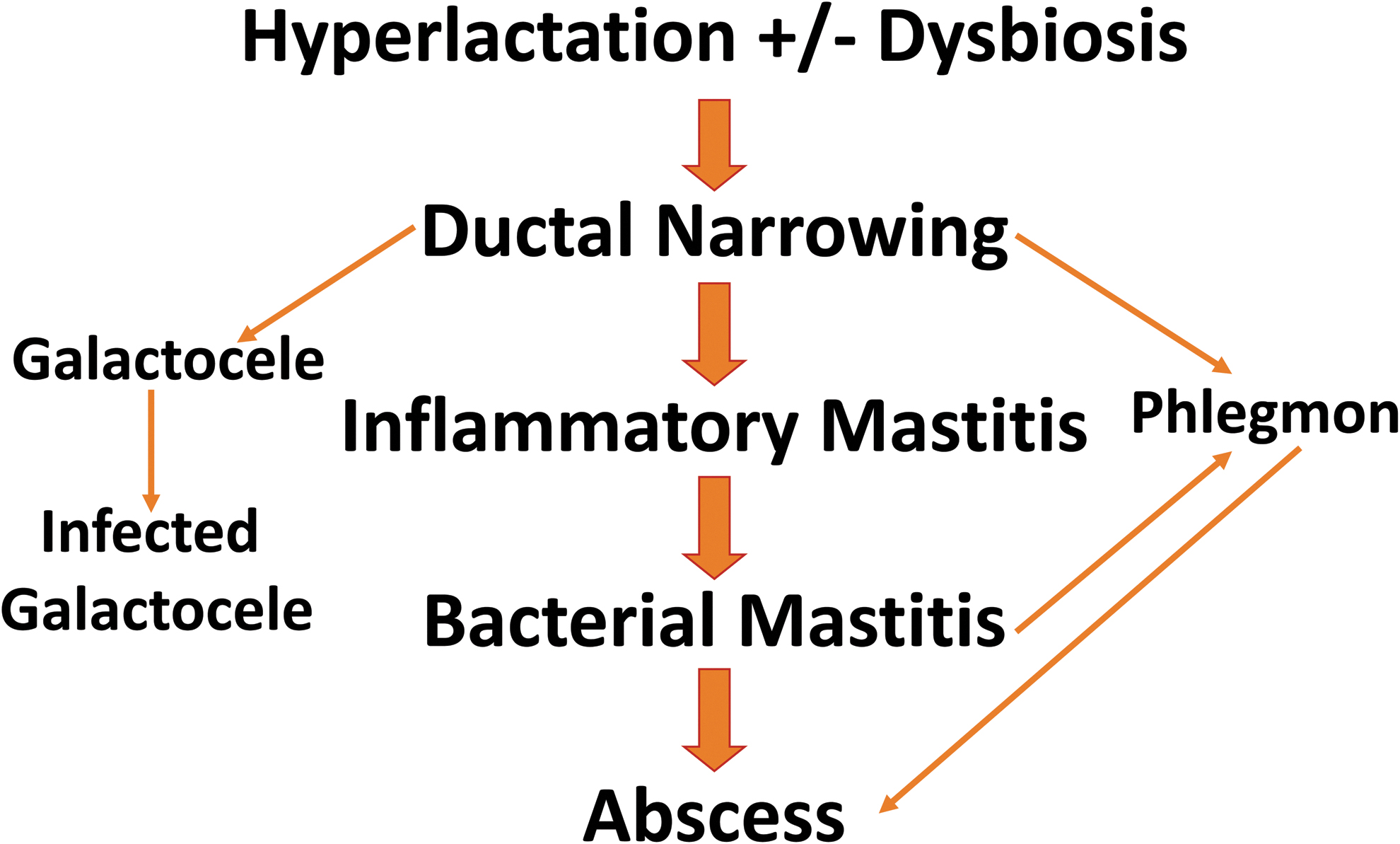
Spectrum of inflammatory conditions in the lactating breast.
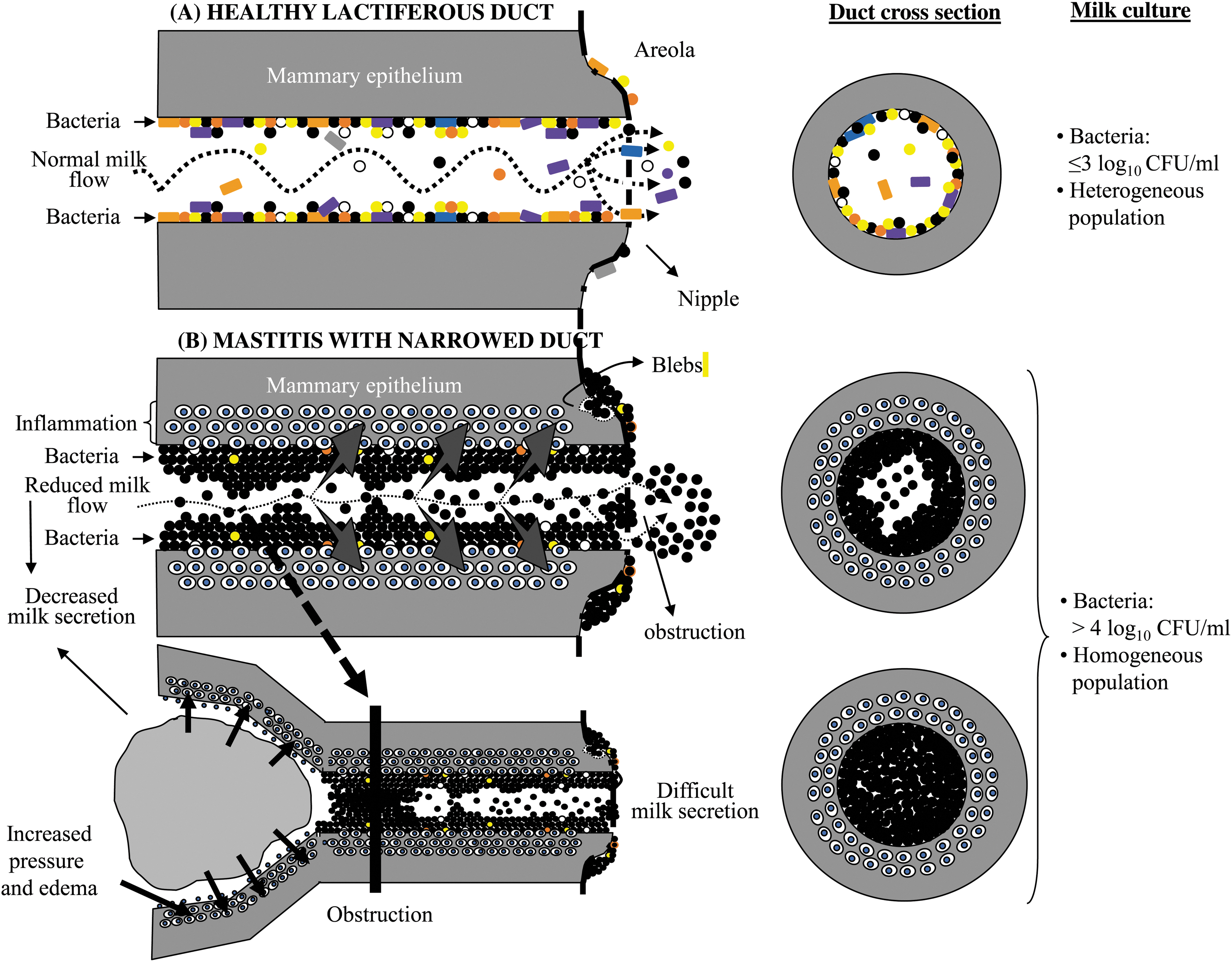
Compared with a healthy lactiferous duct
The pathophysiology, diagnosis, and management of each condition in the mastitis spectrum (ductal narrowing, inflammatory mastitis, bacterial mastitis, phlegmon, abscess, galactocele, and subacute mastitis) will be discussed hereunder. Early postpartum engorgement, a distinct condition that can share some clinical features with mastitis spectrum disorders, will also be reviewed.
Note that this protocol now replaces ABM Protocols #4, Mastitis, and #20, Engorgement, which will both be retired. ABM Protocols #32 (Management of Hyperlactation) 3 and #35 (Supporting Breastfeeding During Maternal or Child Hospitalization) 4 may serve as useful adjuncts to this protocol.
Key Information: Pathophysiology of Mastitis Spectrum Conditions
General principles
Mastitis is inflammation of the mammary gland that most often presents in a segmental distribution of ducts, alveoli, and surrounding connective tissue (Fig. 3). Ductal lumens can be narrowed by edema and hyperemia associated with hyperlactation as well as mammary dysbiosis 5 (Fig. 2). Mammary dysbiosis, or disruption of the milk microbiome, results from a complex interplay of factors, including maternal genetics and medical conditions, exposure to antibiotics, use of probiotics, regular use of breast pumps, and Cesarean births. 6
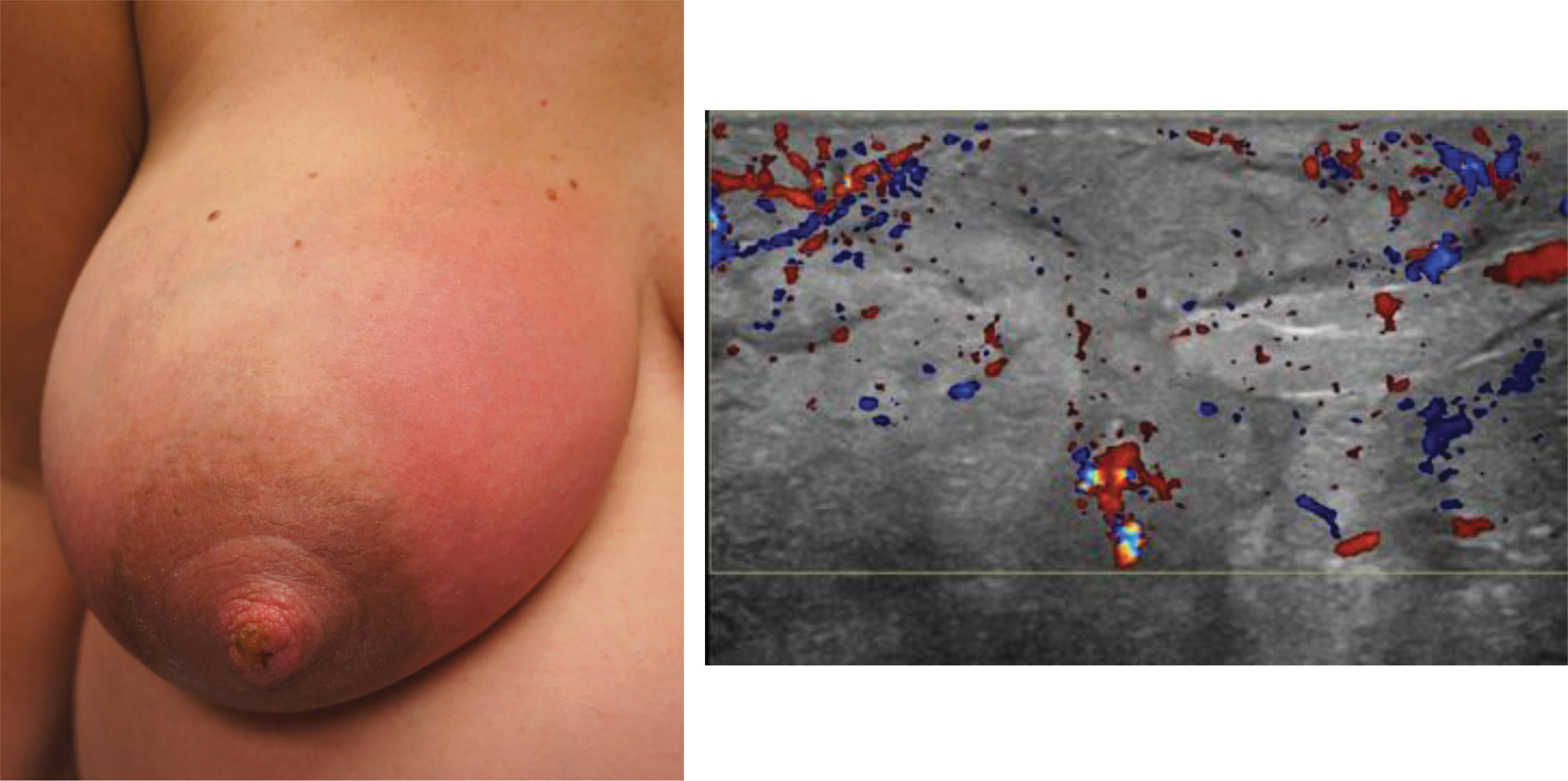
Right breast upper inner quadrant mastitis with ultrasound showing hyperemia and edema without fluid collection.
Basic science research has demonstrated that multiple factors contribute to the development of mastitis (Fig. 4). 6 These include host factors such as hyperlactation, microbial factors such as diversity of the milk microbiome, and medical factors such as antibiotic and probiotic use. Milk stasis has been postulated to be a potential instigating factor for mastitis, although scientific evidence has not proven a causation. No evidence exists that specific foods cause mastitis, although dietary choices may reflect the underlying health and microbiome of an individual. The lactating breast is a dynamic gland that responds to internal and external hormonal stimulation.
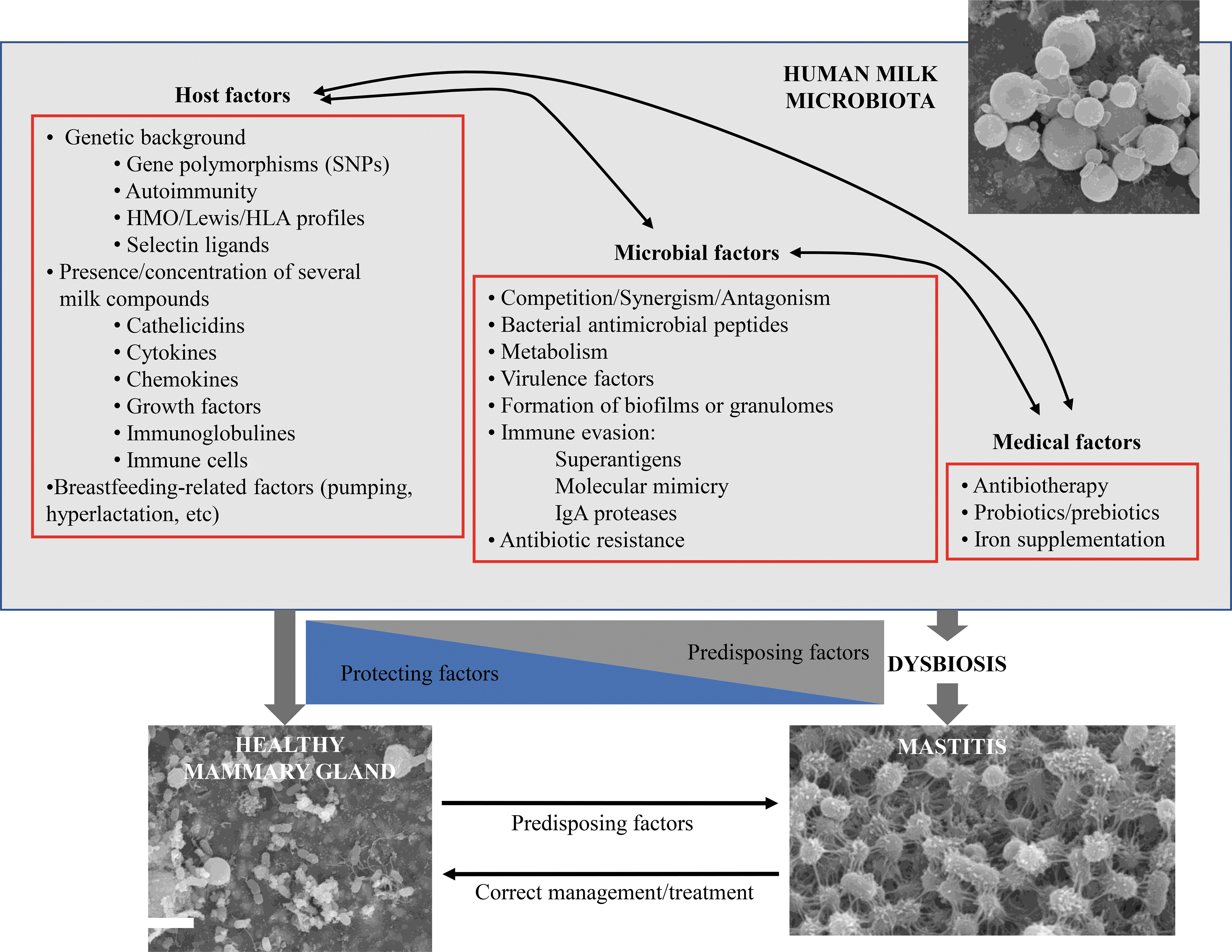
Factors that may play a role in the composition of the human milk microbiota and in protecting or predisposing to mastitis.
Compared with a static repository such as the urinary bladder, the breast requires feedback inhibition to regulate milk production. Reducing milk removal may transiently increase pain and erythema from alveolar distention and vascular congestion; however, it ultimately prevents future episodes as feedback inhibitor of lactation (FIL) and other regulatory hormones activate and decrease milk production. 7 Mothers who experience persistent high milk production despite eliminating iatrogenic causes of excessive milk removal may require additional pharmacological treatment of hyperlactation. 3 These concepts will be expanded upon throughout this protocol.
Engorgement
Some symptoms of early postpartum engorgement may be similar to those of ductal narrowing and early inflammatory mastitis. However, postpartum engorgement that results from secretory activation (lactogenesis II) is a distinct clinical entity related to interstitial edema and hyperemia (Fig. 5). It presents as bilateral breast pain, firmness, and swelling that usually occurs between days 3 and 5 postpartum. 8 Onset may be as late as 9–10 days, although this is less common in multiparous mothers. 8 Cesarean birth is associated with delayed lactogenesis II and, therefore, delayed presentation of engorgement. 9 If engorgement is managed appropriately, it should not progress to other conditions on the mastitis spectrum such as bacterial mastitis, phlegmon, or galactocele.

Day 5 postpartum breast engorgement showing edematous nipple areolar complex and dependent lymphedema with overlying erythema.
Ductal narrowing (e.g., “plugging”)
“Plugging” is a colloquial term for microscopic ductal inflammation and narrowing (Fig. 2) that is related to alveolar distension and/or mammary dysbiosis.
Ducts in the breast are innumerable and interlacing (Figs. 6–8) and it is not physiologically or anatomically possible for a single duct to become obstructed with a macroscopic milk “plug.” It should be noted that ultrasound studies documenting a small number of orifices approaching the nipple 10 reflect limitations of radiographic images as compared with histological anatomy.

Cross section of nipple areolar complex with

Histology image demonstrating functional lobular units with small central duct, surrounding fat, and fibrous stroma (connective tissue).
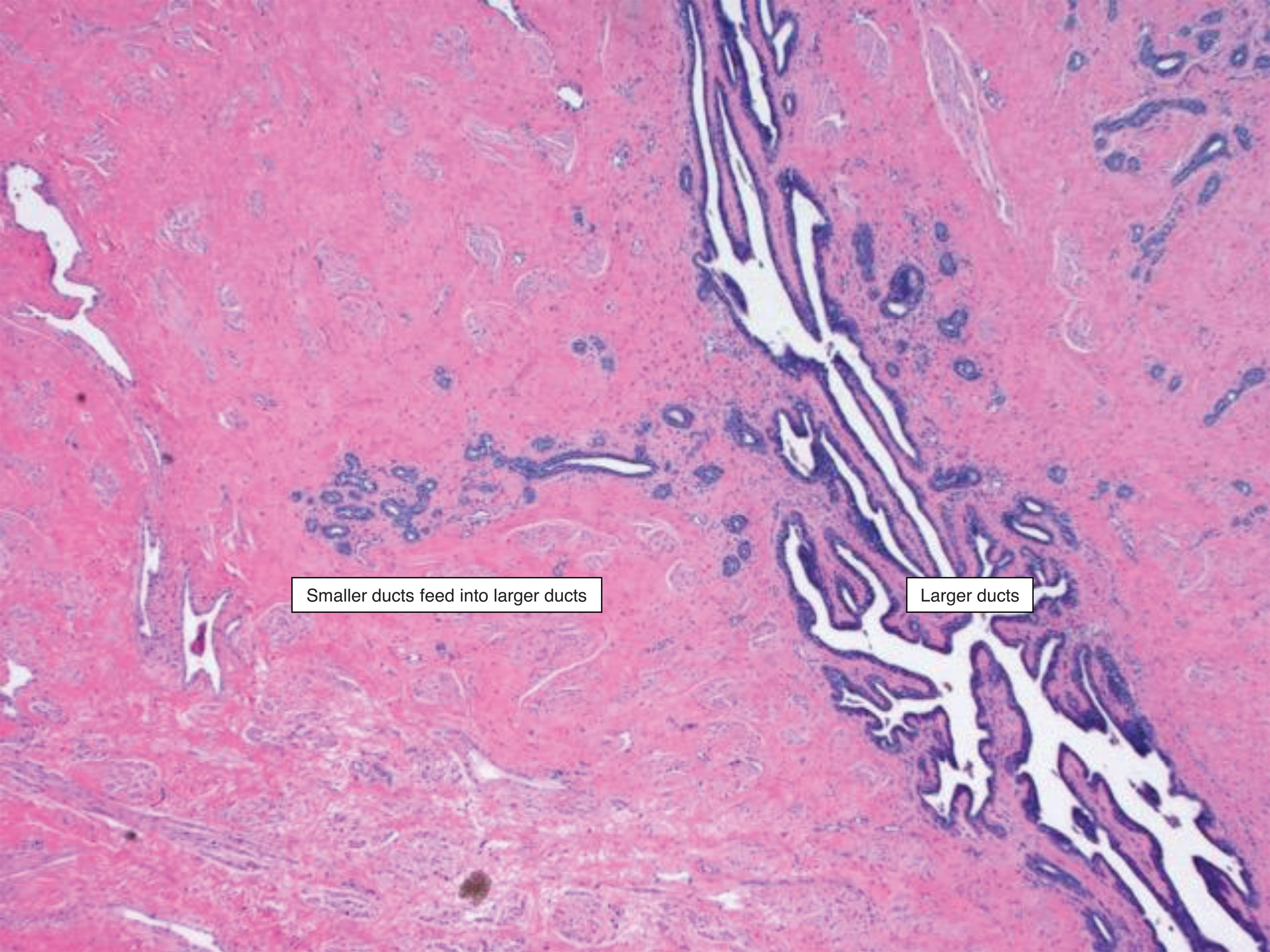
Histology image demonstrating innumerable small ducts draining into larger ductal systems that have complex architecture.
Ductal narrowing presents as a focal area of induration or more globally congested breast tissue that is tender. It may be mildly erythematous from lymphatic congestion and alveolar edema, and does not have associated systemic symptoms (Fig. 9). This may resolve spontaneously, but patients can experience transient residual pain. Patients may feel relief of a “plug” with breastfeeding because this decreases alveolar distension. However, repeated feeding in an attempt to relieve the “plug” will suppress FIL, increase milk production, and ultimately exacerbate inflammation and ductal narrowing. Therefore, physiological breastfeeding and anti-inflammatory measures as described hereunder are most efficacious. Attempts to extrude a “plug” or milk precipitate by squeezing or aggressively massaging the breast are ineffective and result in tissue trauma.

Patient with unilateral left breast “plug” in upper outer quadrant who worsened milk obstruction by repeatedly pumping.
Inflammatory mastitis
When ductal narrowing persists or worsens and surrounding inflammation progresses, inflammatory mastitis develops. Inflammatory mastitis presents as an increasingly erythematous, edematous, and painful region of the breast (Fig. 10) with systemic signs and symptoms such as fever, chills, and tachycardia. It should be emphasized that systemic inflammatory response syndrome may occur in the absence of infection.

Patient with early inflammatory mastitis. Lymphatic congestion is noted by
Bacterial mastitis
Bacterial mastitis represents a progression from ductal narrowing and inflammatory mastitis to an entity necessitating antibiotics or probiotics to resolve. Common organisms in lactational mastitis include Staphylococcus (e.g., S. aureus, S. epidermidis, S. lugdunensis, and S. hominis) and Streptococcus (e.g., S. mitis, S. salivarius, S. pyogenes, and S. agalactiae). Despite the common perception that yeasts cause “candida mastitis,” no scientific evidence exists to support this diagnosis and sterilization of pump parts or infant toys is not recommended to “eradicate” yeast.5,11
Bacterial mastitis is not a contagious entity and does not pose a risk to the infant nor require an interruption in breastfeeding. There is no evidence to support poor hygiene as a cause of bacterial mastitis or the need for routine sterilization of pumps. Handwashing before milk expression and basic pump cleaning practices should be followed.
Although nipple trauma is associated with mastitis, the data are limited by confounding and bias. 1 New evidence about the composition of the human milk microbiome demonstrates that mastitis is not caused by retrograde spread of pathogenic bacteria from visible nipple trauma, as bacteria and fungi identified on the nipple-areolar-complex in the presence of nipple pain and damage are regularly identified in healthy human milk microbiomes. 12 Infection may not occur in the event of a low concentration of the pathogen, presence of nonvirulent or weakly virulent strains, presence of a competitive microbiota, or adequate immunological and nutritional status of the host. 13 Therefore, two patients who host the same pathogen may express different levels of symptomatology.
Bacterial mastitis presents as cellulitis (worsening erythema and induration) in a specific region of the breast that may spread to different quadrants (Fig. 11). An evaluation by a medical professional should be performed if there are persistent systemic symptoms (>24 hours) such as fever and tachycardia. In the absence of systemic signs and symptoms, diagnosis should be considered if the breast is not responding to conservative measures described hereunder. Laboratory testing such as C-reactive protein or a white blood cell count are of limited utility in diagnosing bacterial mastitis as these are markers of inflammation and not specific for infection.

Bacterial mastitis that progressed from early inflammation in the inner quadrant to all quadrants being affected. This patient also pumped and continually fed the infant on the right breast in an attempt to prevent “milk stasis.” This approach resulted in worsened ductal inflammation and bacterial overgrowth as well as milk obstruction.
Phlegmon
Phlegmons are heterogeneous, complex, and ill-defined fluid collections that can occur throughout the body in the setting of inflammation. Excessive deep tissue massage in the setting of ductal narrowing and inflammatory mastitis may propagate phlegmon formation because deep massage potentiates worsened edema and microvascular injury. 14
Phlegmon should be suspected with a history of mastitis that worsens into a firm, mass-like area without fluctuance (Fig. 12). It can be confirmed on ultrasound (Fig. 12).

Clinical appearance of left breast upper inner quadrant phlegmon. Ultrasound showing indistinct fluid collection with surrounding hyperemia and edema.
Abscess
Lactational abscesses represent a progression from bacterial mastitis or phlegmon to an infected fluid collection that necessitates drainage. Approximately 3–11% of women with acute mastitis will develop an abscess. 15
Abscess presents as a progressive induration and erythema, and often a palpable fluid collection in a well-defined area of the breast (Fig. 13). 16 The initial systemic symptoms and fever may resolve as the body walls off the infectious process, or may resolve and then recur. Alternatively, symptoms may continue to worsen until the infected fluid collection is drained. Although the diagnosis of abscess is often made by history and clinical examination, ultrasound also may be utilized (Fig. 14). 17

Patient with right breast upper outer quadrant abscess who underwent office drainage with Penrose drain stent that was removed after 3 days. At 1 week follow-up, the right breast was resolved and the 1 mm stab incision site closed.
Ultrasound image showing fluid collection (
Galactocele and infected galactocele
A galactocele develops when ductal narrowing obstructs the flow of milk to the extent that a significant volume of obstructed milk collects in a cyst-like cavity. 18 Galactoceles can range in size from small (1–2 cm) to very large (>10 cm).
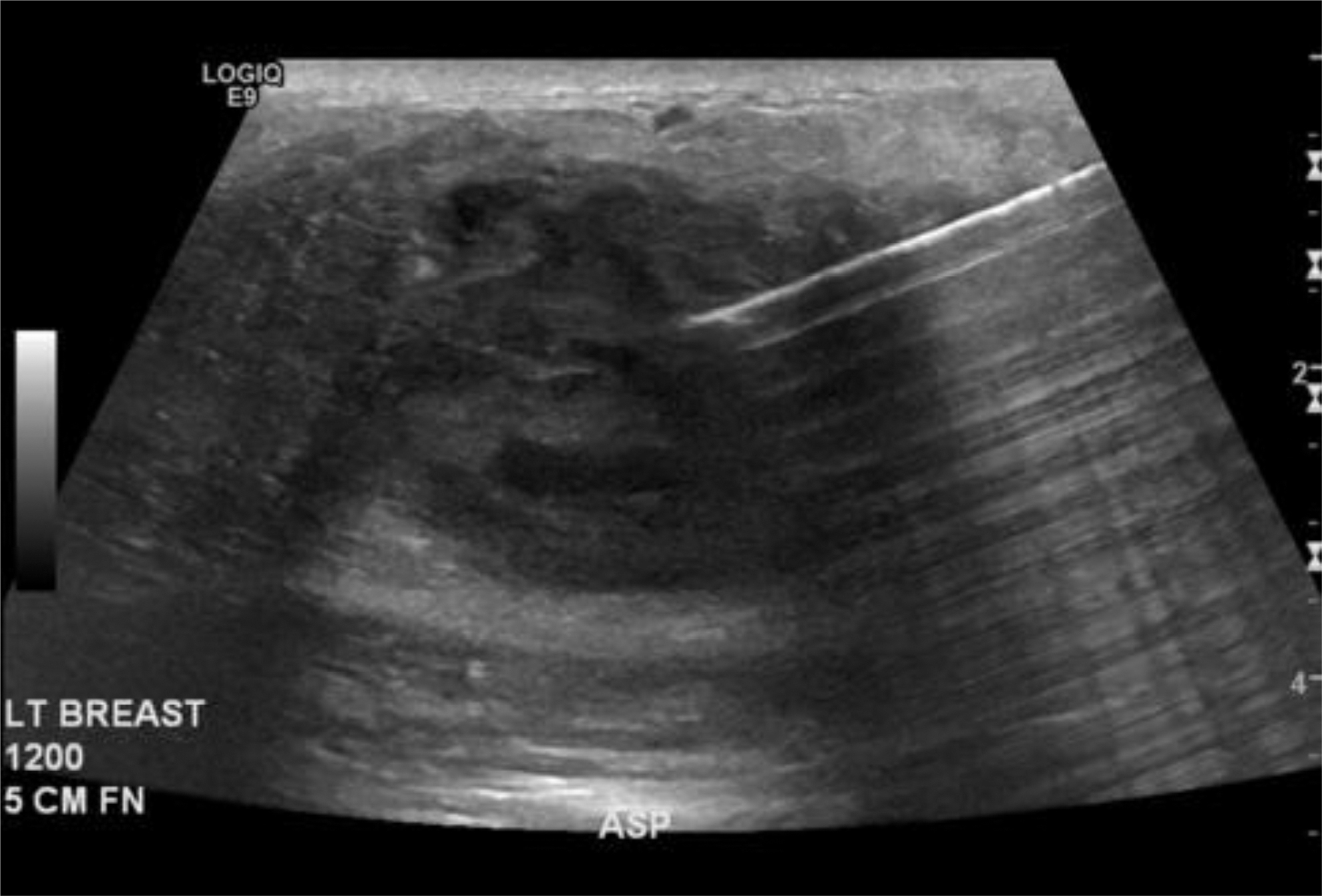
Galactoceles present as a moderately firm mass that gradually or rapidly increases in size over time. The size may fluctuate throughout the day, with a temporary decrease after breastfeeding. It may be uncomfortable, but is generally not as overtly painful as an abscess and does not have associated erythema or systemic symptoms unless it becomes infected (Fig. 15). Ultrasound will show a simple or loculated cystic fluid collection (Fig. 16). On occasion, image-guided aspiration may be utilized to confirm the diagnosis.

Galactocele that was repeatedly drained with a needle and subsequently became infected.

Mammogram showing galactocele adjacent to nipple areolar complex and ultrasound showing septation within galactocele.
Recurrent mastitis
There is no consensus on the definition of recurrent mastitis. Patients may describe having mastitis symptoms such as fever, breast redness, breast swelling, and/or breast pain that occur every 2–4 weeks, or less often. Risk factors include waxing and waning episodes of hyperlactation, dysbiosis, inadequate treatment of prior mastitis, and failure to address the underlying etiology of prior episodes.
Subacute mastitis
Subacute mastitis occurs when ductal lumens become narrowed by bacterial biofilms in the setting of chronic mammary dysbiosis. 5 Dysbiosis is defined as changes in the quantitative and qualitative composition of a host microbiome that contribute to inflammatory disease both acutely and chronically. As in other organs, when the mammary microbiome loses bacterial diversity and the number of anti-inflammatory organisms declines, an increase in pathogenic bacteria occurs.19,20
Under physiological conditions, coagulase-negative Staphylococci (CoNS) and viridans Streptococci (i.e., S. mitis and S. salivarius) form thin biofilms that line the epithelium of the mammary ducts, allowing a normal milk flow. 21 In the setting of dysbiosis, these species proliferate and function under opportunistic circumstances whereby they are able to form thick biofilms inside the ducts, inflaming the mammary epithelium and forcing milk to pass through an increasingly narrower lumen (Fig. 17). CoNS and viridans Streptococci do not produce toxins responsible for acute bacterial mastitis; therefore, systemic symptoms are uncommon and local breast symptoms are milder than in acute mastitis.

Electron microscopy showing normal mammary ducts compared with mammary ducts with biofilm formation.
With subacute mastitis, patients may report a history of previously treated acute bacterial mastitis. Other pertinent history includes Cesarean birth, exclusive pumping, nipple shield use, and other circumstances that alter the milk microbiome. 6 Patients may have needle-like, burning breast pain, nipple blebs, recurrent areas of induration or congestion, and may have unresolved hyperlactation. 22 Sterile milk culture and sensitivities can be performed 23 as noted hereunder.
Recommendations
For each recommendation, the quality of evidence (levels of evidence 1, 2, and 3) and the strength of recommendation (A, B, and C) are noted as defined by the strength of recommendation taxonomy criteria. 24
Management of mastitis spectrum disorders includes general strategies that apply to the entire spectrum, as well as condition-specific interventions. Prompt and effective treatment will halt progression in the spectrum. Many of these measures provide not only treatment, but prevention as well.
Spectrum-wide management strategies will be delineated first, followed by specific recommendations for particular conditions (ductal narrowing, inflammatory mastitis, bacterial mastitis, phlegmon, abscess, galactocele, subacute mastitis, and recurrent mastitis). Recommendations for management of early postpartum engorgement are also included hereunder.
Spectrum-wide recommendations
1. Anticipatory guidance and behavioral interventions
a. Reassure mothers that many mastitis symptoms will resolve with conservative care and psychosocial support.
A Swedish study noted that most women with inflammatory mastitis had complete resolution of symptoms without need for antibiotics or other interventions. The authors attributed this finding to a focus on symptomatic control, appreciation of the physiological anti-inflammatory response, and regular communication between patient and clinician
25
(Fig. 10). Support patients in continuation of breastfeeding and ascertain what resources they may need to prevent early weaning. Assist mothers in identifying ways to decrease stress, increase opportunities to rest, and help resolve early signs of inflammatory mastitis. Fourth-trimester care programs represent a holistic approach to postpartum care, including mental health, psychosocial needs, and breastfeeding counseling.
26
Level of evidence: 3. Strength of recommendation: C.
b. Educate patients on normal breast anatomy and postpartum physiology in lactation.
Many patients experience breast fullness or palpate normal lactational glandular tissue and misinterpret this as “plugging.” They should be reassured that lactating breasts can feel “lumpy” and even painful at times. Although this is uncomfortable, it is not abnormal. Patients should be educated about early postpartum hormonal shifts and a low estrogen state that predisposes patients to sweating and hot flashes that may mimic fevers. In addition, patients should be reassured that infection does not develop in the period of several hours. The pain and redness they may experience in mornings after a long stretch of sleep represents alveolar distention, edema, and inflammation rather than infection. Level of evidence: 3. Strength of recommendation: C.
c. Feed the infant on demand, and do not aim to “empty” breasts.
Milk volume depends on a feedback mechanism whereby increased milk removal increases production.
7
Overfeeding from the affected breast or “pumping to empty” perpetuates a cycle of hyperlactation and is a major risk factor for worsening tissue edema and inflammation (Fig. 18). Mothers can hand express small volumes of milk for comfort until their milk production downregulates to match the infant's needs.
27
Mothers using breast pumps should express only the volume their infant consumes. In some instances, in which the retroareolar region is so edematous and inflamed that no milk is expressible by infant breastfeeding or hand expression, the mother should not continue to attempt feeding from the affected breast during the acute phase (Fig. 19). She can feed from the contralateral breast and return to feeding from the affected breast when edema and inflammation subsides. Edema may resolve more quickly with ice and lymphatic drainage. She should be counseled that a decrease in milk production is expected, but can later be augmented. No evidence exists to support “dangle feeding” (i.e., feeding an infant on the floor with the mother hovering above) or other unsafe infant positions. Patients may consider safe variations on standard feeding positions, with the understanding that this may improve comfort. However, this does not address underlying inflammation. Levels of evidence: 2–3. Strength of recommendation: C. d. Minimize breast pump usage. Mechanical breast pumps stimulate breast milk production without physiologically extracting milk as an infant will. Pumping does not provide the opportunity for bacterial exchange between the infant's mouth and mother's breast, and may, therefore, predispose to dysbiosis.
6
Breast pumps also can cause trauma to breast parenchyma and the nipple areolar complex if improper flange sizes are used, suction is too high, or the mother is pumping for an excessive duration of time. Milk expression should be limited to when mother is separated from her infant or requires pumping for other medically indicated reasons for herself or her infant. Women should not be instructed to express and discard their milk, as bacterial mastitis is not a contraindication to breastfeeding. Women using a breast pump should express milk at a frequency and volume that mimics physiological breastfeeding. Levels of evidence: 2–3. Strength of recommendation: C.
e. Avoid the use of nipple shields.
Available evidence does not support the use of nipple shields. Neither safety nor effectiveness has been demonstrated. Similar to pumping, nipple shields represent nonphysiological breastfeeding and result in inadequate breast milk extraction.
28
Infants often passively drink milk from the shield repository without latching to the parenchyma of the breast. Level of evidence: 3. Strength of recommendation: C.
f. Wear an appropriately fitting supportive bra.
Lactating breasts are highly vascular and require support to avoid dependent lymphedema as well as progressive back and neck pain. Level of evidence: 3. Strength of recommendation: C.
g. Avoid deep massage of the lactating breast.
Deep massage causes increased inflammation, tissue edema, and microvascular injury. Avoid electric toothbrushes and other commercial vibrating or massaging devices. A systematic review concluded that although breast massage may reduce pain, it should not be recommended as standard of care because it requires extensive training to master atraumatic approach.
29
The most successful technique approximates manual lymphatic drainage with light sweeping of the skin rather than deep tissue massage.30,31 It should be noted that gentle compressions during breast pump usage, often termed “hands on pumping,” provide an effect similar to hand expression and is safe if excessive manual force is avoided. Levels of evidence: 1–2. Strength of recommendation: B.
h. Avoid saline soaks, castor oil, and other topical products.
Mastitis is inflammation and/or infection in a deep organ space, and should be managed as such. Topical products such as castor oil will not treat this condition and may in fact cause tissue damage
32
particularly if they are combined with massage.
14
Silicone breast pumps filled with Epsom salt can macerate skin
33
and further contribute to localized hyperemia and edema, and should be avoided. Published evidence and best practice for general wound care do not support the use of saline soaking for pain or nipple trauma. Principles of wound management include handling tissue delicately to minimize further trauma and consideration of ointments and dermal matrices to enhance wound closure.
33
Level of evidence: 3. Strength of recommendation: C.
i. Avoid routine sterilization of pumps and household items.
Mastitis is not contagious and does not result from unhygienic practices. Pump parts should be cleaned appropriately after each use, but routine sterilization of pumps and other household items is not necessary to prevent mastitis.
34
Avoid cleaning of nipple as this may cause skin maceration and pain. Ascending infection is not supported by the highly vascular nature of nipple physiology and anatomy.
35
Similar to other open sites of trauma in the body (e.g., tracheostomies and gastric tube entrance sites), external communication prevents deep tissue infection rather than promotes it. Level of evidence: 3. Strength of recommendation: C.
2. Medical interventions
a. Decrease inflammation and pain.
Ice and nonsteroidal anti-inflammatory drugs (NSAIDs) can reduce edema and inflammation and provide symptomatic relief (Figs. 10 and 19), and acetaminophen/paracetamol can provide analgesia.
36
For example, ice can be applied every hour or more frequently if desired. Ibuprofen can be dosed 800 mg every 8 hours
37
and acetaminophen/paracetamol 1,000 mg every 8 hours
38
in the acute setting. Although heat will vasodilate and may worsen symptoms, it also may provide comfort for some patients.
39
The use of warm showers and antipyretics did not improve mastitis outcomes in a randomized controlled trial.
25
Sunflower or soy lecithin 5–10 g daily by mouth may be taken to reduce inflammation in ducts and emulsify milk.22,40 Levels of evidence: 1–3. Strength of recommendation: C.
b. Treat associated nipple blebs and avoid unroofing.
If a nipple bleb, which represents ductal inflammatory cells propagating to the surface and lodging (Figs. 2 and 20), is present, do not unroof the bleb as this will cause trauma and further luminal narrowing. Oral lecithin and application of a topical moderate potency steroid cream such as 0.1% triamcinolone may be used to reduce inflammation on the surface of the nipple.
22
This is safe with breastfeeding and can be wiped off with a tissue or towel before feeding the infant.
41
Levels of evidence: 2–3. Strength of recommendations: C.
c. Treat hyperlactation, or breast milk “oversupply.”
Hyperlactation predisposes patients to luminal congestion and inflammation, which in turn facilitates mammary dysbiosis. This may potentiate a vicious cycle, as dysbiosis is a cause of ductal narrowing and inflammation. See ABM Protocol 32, Management of Hyperlactation.
3
Level of evidence: 2. Strength of recommendation: C. d. Utilize therapeutic ultrasound. Therapeutic ultrasound, or TUS, uses thermal energy to reduce inflammation and relieve edema. TUS may be an effective treatment for conditions arising in the mastitis spectrum.
42
TUS can be performed under the supervision of a trained physician or physiotherapist on a daily basis until relief is achieved. The breast treatment setting is 1 MHz, intensity 2.0 W/cm2 for 5 minutes.
43
If a patient has persistent symptoms despite several days of treatment, health care providers should consider additional investigations. Levels of evidence: 2–3. Strength of recommendation: C.
e. Reserve antibiotics for bacterial mastitis.
Use of antibiotics for inflammatory mastitis disrupts the breast microbiome and increases the risk of progression to bacterial mastitis. Furthermore, nonselective use of antibiotics promotes development of resistant pathogens. Prophylactic antibiotics have not been shown to be effective in the prevention of mastitis.
44
It should be noted that many antibiotics and antifungal medications have anti-inflammatory properties, and this may explain why women experience relief when taking these. Level of evidence: 2. Strength of recommendation: B.
f. Consider probiotics.
Data regarding probiotics are mixed.44–47
A systematic review suggested that probiotics may be effective for both treatment and prevention of mastitis, but a strong recommendation could not be made due to limitations of the studied trials.
47
If utilized, the probiotic should contain Limosilactobacillus fermentum (formerly classified as Lactobacillus fermentum) or, preferably, Ligilactobacillus salivarius (formerly classified as Lactobacillus salivarius) strains.48,49 Note that only selected strains of these bacterial species may be effective against mastitis pathogens. Therefore, clinical trial outcomes cannot be generalized to an entire species in the same way that antibiotics may be efficacious against one strain of a pathological bacteria but not another. Levels of evidence: 1–2. Strength of recommendation: B.
g. Evaluate for perinatal mood and anxiety disorders (PMADs).
Women with a history of anxiety and depression experience higher rates of mastitis symptoms,
50
and PMADs are increased in any patient experiencing breastfeeding complications. Although any clinicians contacting postpartum patients should screen for PMADs,
26
particular attention should be paid to patients feeling defeated and/or withdrawn as a result of challenges with breastfeeding. Furthermore, patients who express significant worry about potential recurrence and are unable to stop pumping despite recommendations may be suffering from anxiety. Extreme pain out of proportion to exam may also point to alterations in sensitivity to stimulation as a result of PMADs and, therefore, should be considered in the differential diagnosis.
51
Careful exploration of Dysphoric Milk Ejection Reflex and/or nursing aversion may also be warranted if the patient does not report traditional symptoms of PMADs.
52
Level of evidence: 3. Strength of recommendation: C.

Patient with history of right breast mastitis who was instructed to pump every 2 hours to “keep the breast empty.” This resulted in severe upregulation of milk production in her right breast and a continued cycle of mastitis. After being instructed to feed from the less full (left) breast first, she downregulated the right breast and experienced no recurrent episodes of mastitis.
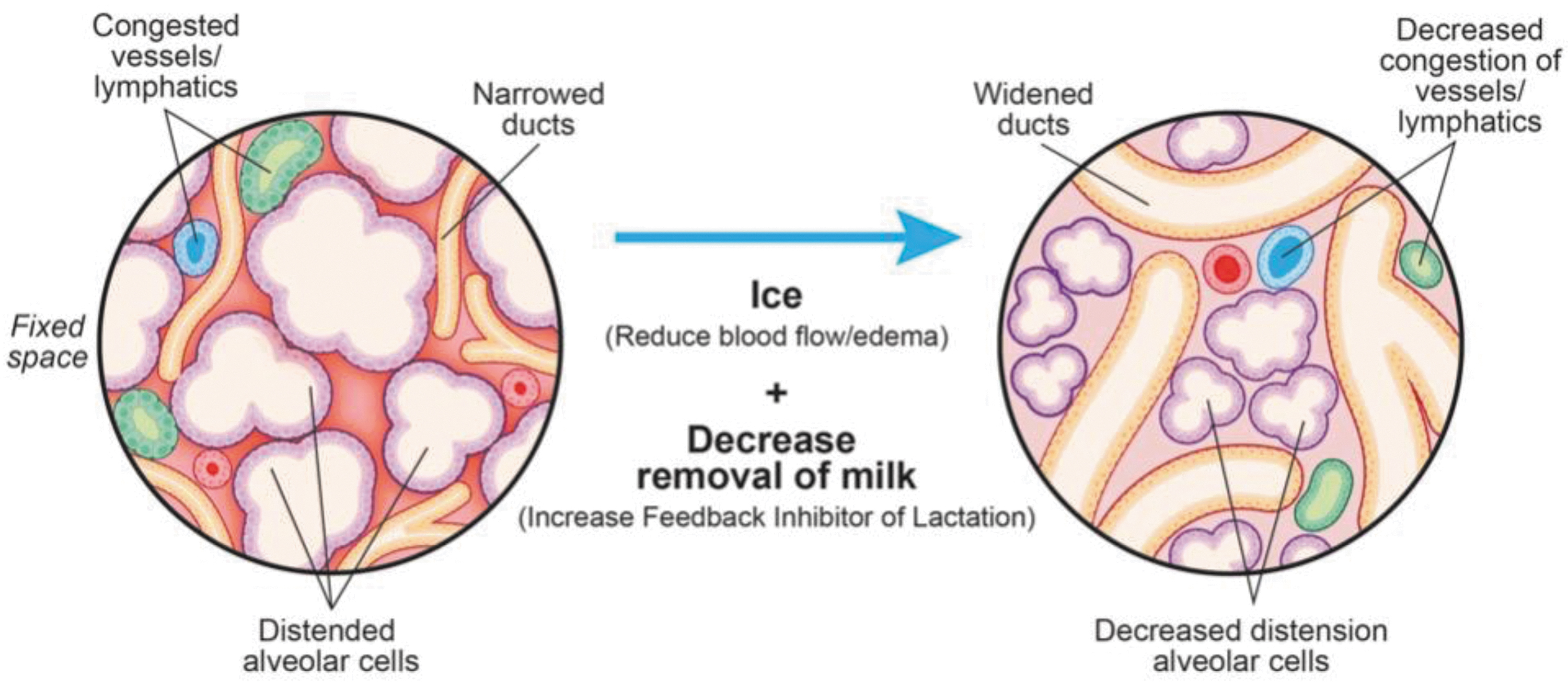
Ducts can become narrowed secondary to alveolar distention and congested vessels and lymphatics. Ice and decreased removal of breast milk reduce ductal narrowing and breast swelling.

Examples of different presentations of nipple blebs.
Condition-specific recommendations
a. Recommendations for postpartum engorgement in lactogenesis II
Minimize intravenous fluids during labor, as interstitial fluid accumulation exacerbates edema and engorgement.
53
Promote “rooming in” to allow physiological breastfeeding and avoidance of pumping.
54
Instruct mothers on hand expression to relieve symptoms and provide breast milk for infants who may not transfer milk effectively or are separated from their mothers.
55
Perform reverse pressure softening of the areola,
56
and manual pump or hand expression to remove small volumes of milk before infant latch and facilitate physiological milk transfer. Consider lymphatic drainage to alleviate interstitial edema
31
(Fig. 21). Consider ice for symptomatic relief. Studies have not demonstrated cabbage leaves to be more effective than ice,
57
suggesting that the therapeutic benefit is related to vasoconstriction from cold rather than a property of cabbage itself. Importantly, cabbage may carry Listeria bacteria.
Levels of evidence: 2–3. Strength of recommendations: B–C.
b. Recommendations for ductal narrowing and inflammatory mastitis
• Follow spectrum-wide recommendations mentioned earlier.
c. Recommendations for bacterial mastitis
Antibiotic selection, dosage, and duration for bacterial mastitis are outlined in Box 1. It is safe for children to consume milk from a breast with bacterial mastitis.
58
Routine hospital admission and IV antibiotics are not necessary unless known multidrug-resistant organism (MDRO) or clinical presentation mandates (e.g., evidence of severe sepsis and inability to tolerate oral medication or fluid). Of note, some MDRO may be treatable using oral antibiotics. Antibiotic choice should be driven by culture data or local antibiogram. If hospital admission is necessary, mother and infant should be kept rooming in together and allowed to continue to breastfeed on demand. ABM Protocol #35, Supporting Breastfeeding During Maternal or Child Hospitalization, refers to other recommendations in detail.
4
Consider intravenous fluid administration if patient's oral intake of fluids is suboptimal as this may alleviate tachycardia and improve symptomatology. If there is no symptomatic improvement after 48 hours of first-line therapy, consider a milk culture to evaluate for resistant and/or less common pathogens such as methicillin-resistant Staphylococcus aureus (MRSA).
58
Consider local susceptibility and resistance patterns and proceed to empiric therapy. Other situations in which to consider early milk culture include mothers expressing breast milk for an immunocompromised infant in the neonatal intensive care unit, health care workers in areas with a high prevalence of MRSA, and patients with recurrent infections. Data regarding the role of probiotics in bacterial mastitis continue to emerge. Probiotics have been shown not to alter composition of human milk microbiome.44–47
Levels of evidence: 2–3. Strength of recommendations: C.
d. Recommendations for phlegmon
Lactational phlegmon may require extended antibiotics for complete resolution, but cases should be considered individually.
14
A phlegmon may coalesce into a drainable abscess and, therefore, patients should be followed carefully for this development. Interval examination and imaging is warranted until complete resolution.
14
Level of evidence: 2. Strength of recommendations: C.
e. Recommendations for abscess
Drain the abscess to achieve source control. Needle aspiration with fluid culture and sensitivity is often recommended as the first-line intervention for lactational abscess.
59
However, patients most often require recurrent aspirations for definitive resolution. Repeated aspirations may be stressful and discouraging for the patient, and risk breastfeeding discontinuation.60–62
Drain placement as the initial intervention should be considered for definitive management at the time of the index procedure. Office drainage is demonstrated in published videos63,64 and illustrated in Figure 13. Patients also can be referred to interventional radiology for drain placement. Drains or skin stents should be placed to gravity rather than suction (Fig. 22). If formal drain is not available, adaptations using supplies such as Foley catheters or glove fingers can be used based on local resources. Strictly avoid vacuum-assisted wound devices on a lactating breast. After aspiration or drain placement, mothers should continue breastfeeding from the affected breast. Milk fistula rate is <2%, but lactation must be managed appropriately and hyperlactation treated if present.
65
Antibiotic duration is commonly 10–14 days
58
; however, a shorter course may be appropriate if there is rapid resolution of surrounding cellulitis. Tissue inflammation and phlegmonous changes may take several weeks to resolve and patients may feel the presence of a small mass-like area. They should undergo interval examination and imaging to ensure resolution.
14
Levels of evidence: 2–3. Strength of recommendations: C.
f. Recommendations for galactocele and infected galactocele
For symptomatic galactoceles, drainage is recommended for symptom relief, confirmation of diagnosis, and to decrease mass effect to facilitate latch. Aspiration almost always results in incomplete drainage and/or recurrence, and repeated aspirations risk converting a sterile galactocele into an infected galactocele. Therefore, drain placement as described earlier is recommended. An infected galactocele requires drainage as well as antibiotics (Fig. 15).
66
Level of evidence: 3. Strength of recommendations: C.
g. Recommendations for recurrent mastitis
Examine patients and obtain milk culture to establish a diagnosis of true recurrent mastitis, rather than treating empirically. Breast milk culture
23
(Box 2) can identify and provide sensitivities of uncommon pathogens and resistant bacteria. For example, although CoNS are commonly present in breast milk, they have also been identified as opportunistic pathogens in mastitis.
67
MRSA and resistant CoNS will not respond to typical antibiotics used for acute mastitis such as dicloxacillin or cephalexin. Ensure resolution of bacterial mastitis, as earlier, with follow-up examination of patients. Evaluate breastfeeding and/or pumping for potential risk factors for mastitis (e.g., excessive massage and unnecessary pumping). Consider daily probiotic use with L. fermentum or, preferably, L. salivarius for prevention,48,49 recognizing the limitations of different strains of the same species having different efficacies. Prophylactic antibiotics have not been shown to be effective in the prevention of mastitis and may select antibiotic-resistant strains.
44
Multiple recurrences in the same location warrants radiology evaluation to rule out an underlying mass or other abnormality such as granulomatous mastitis.
68
Inflammatory breast cancer is an aggressive subtype of malignant tumors that presents with progressive erythema, breast retraction, and peau d'orange appearance of the breast. Any concern for inflammatory breast cancer warrants urgent referral to breast surgery and oncology.
69
Levels of evidence: 1–3. Strength of recommendations: B–C.
h. Recommendations for subacute mastitis
Individual mammary microbiomes have different environmental thresholds at which opportunistic bacterial pathogens become symptomatic. Further, milk culture may not grow a dominant organism. Therefore, treatment should be individualized based on clinical history and level of suspicion for subacute mastitis.70,71 Antibiotics in the macrolide class may have the best efficacy in this clinical scenario due to the intracellular mechanism of action, though more studies are needed.
72
Probiotics containing L. salivarius or L. fermentum strains represent a treatment option, although more studies are required.48,49
Levels of evidence: 2–3. Strength of recommendations: B–C.
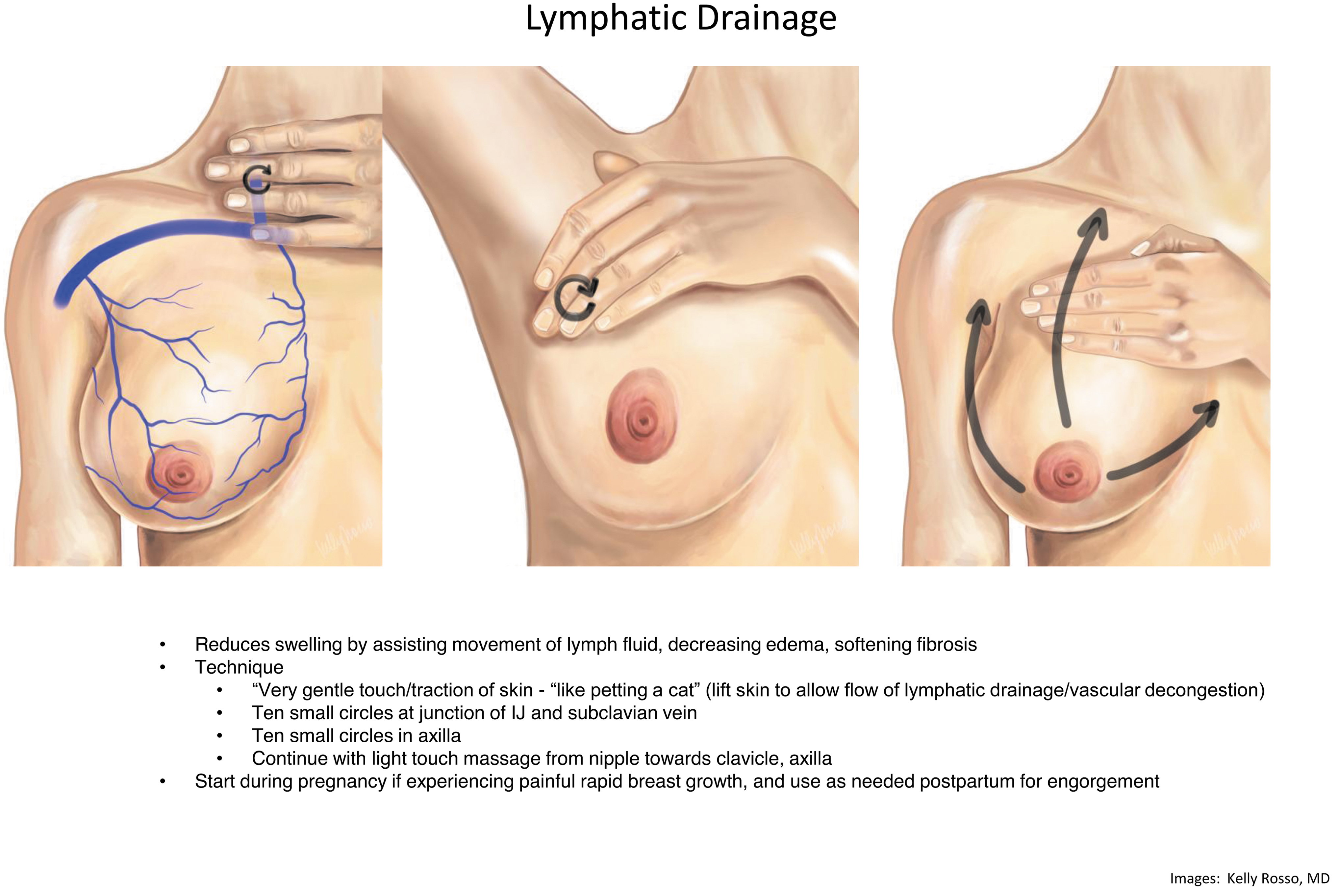
Technique of lymphatic drainage.
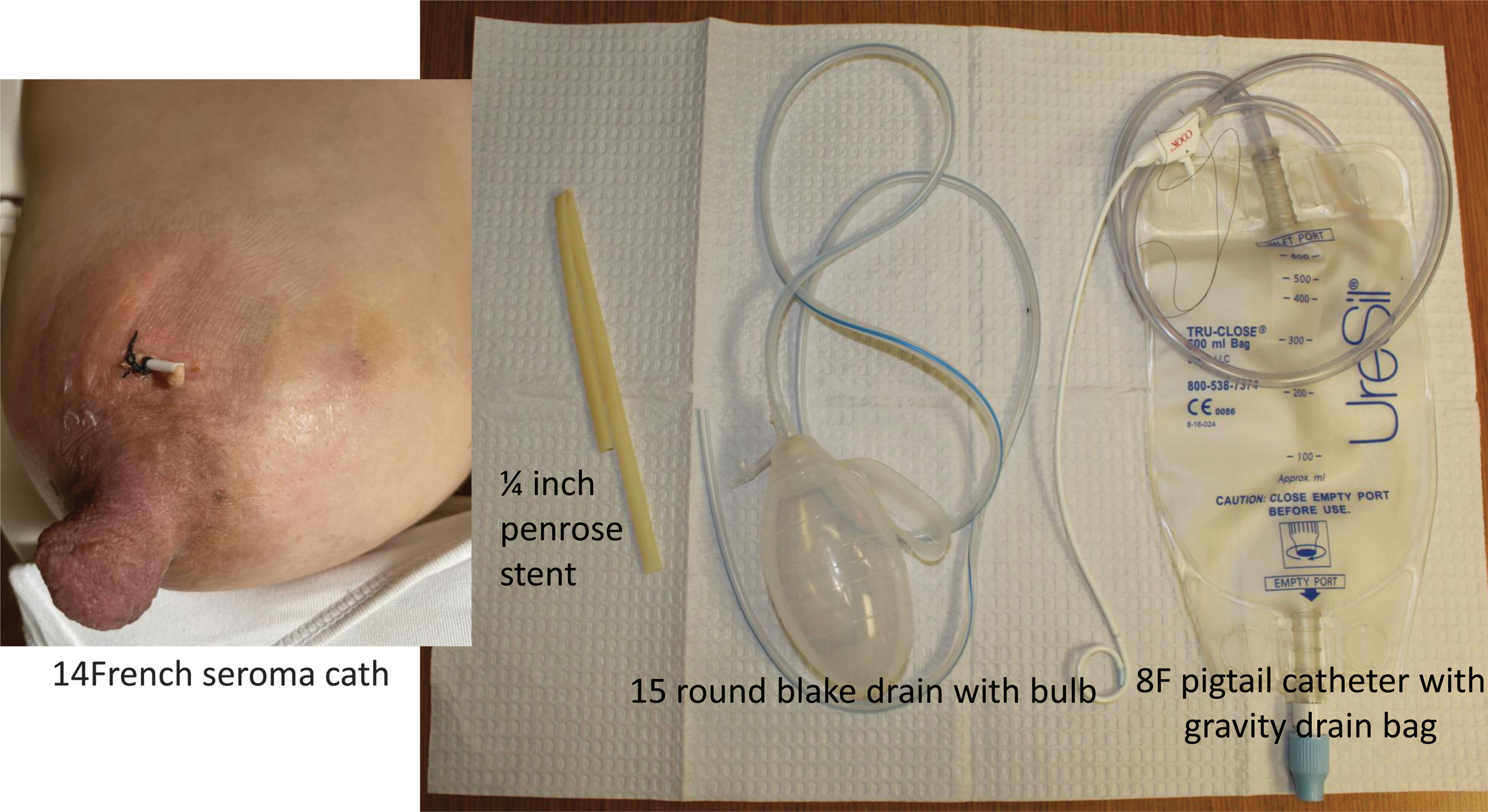
Options for drainage of lactational fluid collections.
How to Perform a Sterile Breast Milk Culture
Summary
Overall, conditions occurring in the mastitis pathophysiological spectrum can be prevented and treated by reducing iatrogenic interventions and utilizing simple management principles such as ice, NSAIDs, and physiological breastfeeding. Attention should be given to appropriate treatment of hyperlactation as an primary underlying risk factor for mastitis. Similarly, given the importance of a healthy breast milk microbiome in preventing mastitis, risk factors for dysbiosis should be addressed. Understanding the pathophysiology of ductal narrowing and inflammation allows clinicians to select targeted effective treatments for mastitis.
Traditional recommendations to augment milk removal to counteract milk stasis and to massage breast tissue to relieve ductal obstruction from milk “plugs” lack physiological validity. Frequent stimulation of breasts with congested alveolar cells worsens hyperemia and edema, causing increased pain, swelling, and redness. This not only worsens pain and edema, but also decreases the ability of an infant to obtain an atraumatic latch and effectively withdraw milk from the breast. Frequent pumping also disrupts the milk microbiome, potentiating the development of mammary dysbiosis and increasing the risk for bacterial mastitis. In addition, massage of the mammary gland causes capillary injury and tissue necrosis, and is a primary risk factor for phlegmon and abscess development.
Areas for Future Research
Clinical studies on mastitis and related disorders are limited by study design and confounding factors. For example, nipple trauma appearing to be a cause of mastitis likely represents an association rather than a causation. Nipple trauma is extremely frequent in hyperlactation, which is a risk factor for mastitis. Future studies should carefully control for potential confounding factors as well as explore diverse cultures and practices throughout the world. In addition, higher quality studies are needed to determine precise recommendations regarding antibiotics as the presence of even small quantities of antibiotics in human milk alters the diversity and resilience of the human milk microbiome. 73
Because antibiotics are often prescribed through telephone triage in many countries, studies to clarify prevalence of bacterial mastitis as opposed to engorgement and/or inflammatory mastitis are necessary. The use of probiotics warrants further research as well. As women in the peripartum period are at their lifetime highest risk for developing an anxiety or mood disorder, the distinction between symptoms of mood and anxiety disorders versus mastitis should also be explored.
Footnotes
Disclosure Statement
J.M.R. has been the PI of research projects and clinical assays funded by Puleva/Biosearch Life (Granada, Spain) or Nutricia (Utrecht, The Netherlands), involving the characterization, safety, and efficacy of probiotic strains for the mastitis target. He and his research group have never received any payment or royalty related to the commercialization of probiotic strains.
Funding Information
No funding was received for this article.
ABM protocols expire in 5 years from the date of publication. Content of this protocol is up to date at the time of publication. Evidence-based revisions are made within 5 years or sooner if there are significant changes in the evidence.
The Academy of Breastfeeding Medicine Protocol Committee Members:
For correspondence:
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.