
Abstract
Introduction:
Maternal stress can lead to changes in the composition of human breast milk. The present study evaluates cortisol levels in the breast milk of mothers after giving birth preterm, term, or post-term, and ascertains whether the levels are associated with maternal stress.
Materials and Methods:
Included in the study were mothers who gave birth vaginally after 32 weeks of gestation between January and April 2022. The breast milk was expressed with an electronic pump under the supervision of a nurse on day 7 following birth, and 2 mL samples of the milk were transferred into microtubes and stored at −80°C. Stress in the mothers was measured using the perceived stress scale developed by Cohen et al. The human breast milk cortisol levels were determined using an enzyme-linked immunoassay in a single session.
Results:
A total of 90 mothers, including 30 with preterm births, 38 with term births, and 22 with post-term births, were included in the study. The median stress scale score was 28 (17–50) and the median breast milk cortisol level was 0.49 ng/mL (0.1–1.96 ng/mL). A significant positive correlation was noted between the stress scale scores and breast milk cortisol levels (r = 0.56, p < 0.01). The breast milk cortisol levels and maternal stress scale scores were significantly higher in the preterm birth group than in the term birth group (p = 0.011 and p = 0.013, respectively).
Conclusion:
Although there is an association between maternal stress and preterm labor and milk cortisol levels, we believe that more studies are needed to establish a causal link.
Introduction
Human breast milk contains many of the nutrients and bioactive substances that infants need. 1 Breastfeeding in the first months of life starting after birth supports healthy development in infants and decreases the risk of respiratory tract infections, diarrhea, and sudden infant death syndrome in infancy, and the risk of hypertension, diabetes, and obesity in adolescence.2–4 The levels of bioactive substances in human breast milk may vary between mothers, with maternal psychosocial stress being one of the factors behind such variations. 5 Maternal psychopathology was reported to affect the levels of lipids, hormones, and immune components in breast milk. 6 It has been demonstrated that human cortisol levels in breast milk and their immunological properties can be affected by psychosocial stress in the mother.6,7
Physiological and/or psychological stress before or during pregnancy (due to the timing of the pregnancy, socioeconomic status, family structure, maternal nutrition, maternal disease, etc.) can affect maternal stress levels. 8 Postpartum stress increases maternal serum cortisol levels and affects breast milk production. Maternal serum cortisol level has been reported to be a good indicator for postpartum stress. 9 In addition, a negative correlation between breastfeeding rate and perceived stress score (PSS) has been reported. 10 The STEPS (Steps to Healthy Development of Children) study investigated the maternal factors that affect breast milk cortisol levels. It was reported that the cortisol levels of breast milk are high in preterm births. 8 Nevertheless, the evaluation of PSS and post-term birth was not assessed in the STEPS study. In addition, it has been reported in the literature that cultural differences also affect the level of maternal stress.
It has also been reported that variables such as socioeconomic status and whether it is a desired pregnancy or not may be perceived differently. 11 In our study, we think that investigating the factors affecting maternal stress and milk cortisol level in a different culture with dense rural settlement might be a guide in planning social support programs.
To our knowledge, there are no studies investigating the relationship between post-term birth and breast milk. In a study conducted by McCool et al. in 1994 involving 38 primiparous adolescent pregnant women, anxiety scores were higher in the mothers of post-term infants than in those who delivered at-term infants, although a regression analysis revealed no significant difference between the gestational-age groups in terms of anxiety levels and salivary cortisol levels. 12 Post-term deliveries are relatively high in our region due to unattended pregnancies and the sociocultural structure. Considering the limited data on post-term pregnancies in the literature, we believe that studies on this subject may provide guidance on pregnancy and postpartum follow-up, especially for the developing and underdeveloped countries.
In similar studies in the literature, PSS has been used to measure maternal stress.13,14 In this type of scale, a separate validity study should be conducted for each different language. We preferred to use the PSS because it is a questionnaire that has been validated for our country, is suitable for the region we live in, and is easy to understand. However, since the PSS scale examines data from the last month, we aimed to conduct a study covering the last 3 weeks of pregnancy and the first week postpartum in the measurement of maternal stress in our study. Since our aim was not to investigate the causal relationship between gestational age and maternal stress, but only to investigate whether there was a relationship and to examine the effect of stress on milk cortisol levels, we therefore thought that the PSS was a suitable scale for our study.
We hypothesized that maternal stress and milk cortisol levels may be different in nonterm deliveries compared with term deliveries. There is no study in the literature comparing maternal stress and breast milk cortisol levels in preterm, term, and post-term infants. Therefore, in our study, in light of the hypothesis that there may be a relationship between gestational age, milk cortisol, and maternal stress, we aimed to examine the relationship between maternal stress score and breast milk cortisol level with preterm, term, and post-term infants in a rural region of our country with a high birth rate.
Materials and Methods
The study was conducted prospectively on a cohort of patients who presented to the Obstetrics and Gynecology Clinic of Erzurum City Hospital between January and April 2022. Approval for the study was granted by the Ethics Committee of the Atatürk University Faculty of Medicine (approval No.: B.30.2.ATA.0.01.00/07.05.2020). Informed consent was obtained from all participating mothers.
Study inclusion criteria
Included in the study were mothers who delivered their babies after 32 weeks of gestation. Mothers of infants with a gestational age of 32–366 weeks at birth were included in the preterm group, those with a gestational age of 37–42 weeks at birth were included in the term group, and those with a gestational age above 42 weeks at birth were included in the post-term group. Only mothers who underwent spontaneous vaginal delivery were included in the study to rule out any stress factors associated with cesarean section.
Exclusion criteria
The exclusion criteria were cesarean section, preeclampsia, eclampsia, diabetes mellitus, fetomaternal hemorrhage, multiple pregnancy, erythroblastosis fetalis, intrauterine growth restriction in the fetus, presence of a congenital anomaly in the fetus, previous maternal diagnosis of depression, and maternal need for intensive care unit admission after birth.
The women were recruited at their first postnatal midwife visit. All women who met the inclusion and exclusion criteria were interviewed face to face. The study protocol and purpose were explained, and an informed consent form was given. The mothers who read and accepted this consent form were told that some milk would be taken for the study while breastfeeding education was given when they came to the postnatal 7th day follow-up visit. They were also told that they would be given a PSS form to complete. PSS forms were completed by the mothers themselves on the 7th postnatal day at the hospital. A total of 142 mothers agreed to participate in the study. However, only 90 of them came for postnatal follow-up (Fig. 1).
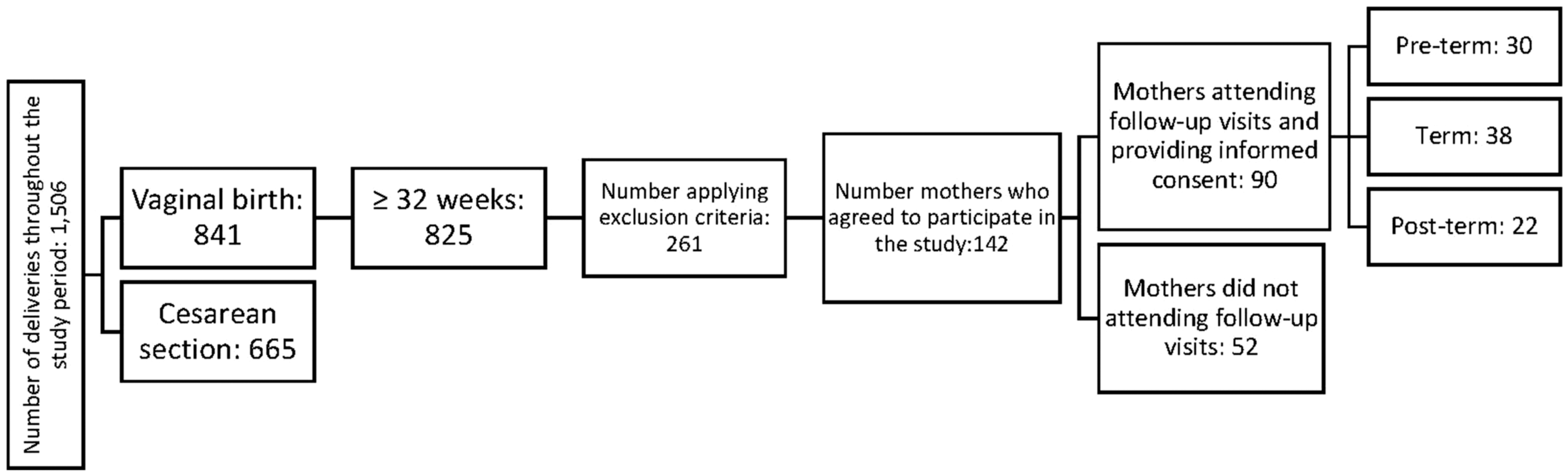
Flow diagram showing the number of participants.
Collection of breast milk samples
Milk collection was planned in the routine follow-up of the babies. Babies who are discharged from our hospital after birth are called to the hospital for routine follow-up (for bilirubin measurement, screening test) on the 2nd, 4th, and 7th days after birth. For babies who were already in the hospital, the mothers remained with them and the milk samples were collected on the 7th day.
Breast milk samples were collected over 3 months (January, February, and March) to minimize the effect of seasonal variations. A health care professional responsible for providing breastfeeding counseling to the mothers collected fresh breast milk samples between 12:00 and 14:00 hours on day 7 after birth. The breast milk samples were collected into sterile bottles (Medela Symphony) from the right breast using an electronic breast pump (Medela Symphony). After emptying the breast completely, a 2-mL breast milk sample was withdrawn into a sterile syringe and transferred into a low-protein binding microtube (Eppendorf). The samples were stored at −80°C until analysis.
Measurement of human breast milk cortisol levels
After thawing the milk samples under appropriate conditions, all analyses were performed in a single session in the Atatürk University Laboratory.
The cortisol levels in the human breast milk samples were measured using enzyme-linked immunosorbent assay (ELISA) kits sourced from Enzo Life Sciences, Inc. (Farmingdale, NY), in accordance with the manufacturer's instructions, and using a Dynex automated ELISA reader (Dynex Technologies Headquarters, Chantilly, VA).
Social data of the mothers and maternal stress assessment
All forms were given to the mothers when they came to the 7th day follow-up in the breastfeeding room. For the completion of forms, the time period when the babies were asleep was preferred. The forms were filled in by mothers.
The demographic form included maternal age, duration of marriage, number of pregnancies (primiparous, multiparous), pregnancy desire (wanted, unwanted), educational status (primary school, secondary school, high school, university), income status (low, middle, high according to the national poverty threshold), employment status (housewife, employed), family type (nuclear family if consists of parents and children, extended family if the house is shared with other relatives), and infant's gender being recorded.
Perceived stress scale
The scale was developed by Cohen et al. in 1983. 15 The Turkish validity and reliability study of the scale was conducted by Eskin et al. 16 The 14-item PSS was designed to assess to what degree the respondent perceives certain life situations as stressful. The participants rate items on a 5-point Likert scale, ranging from “Never” (0) to “Quite Often” (4), and seven positive items (items 4, 5, 6, 7, 9, 10, 13) are inversely rated. The total possible PSSs are in the 0–56-point range, and higher scores indicate greater perceived stress.
Since the PSS was used to assess perceived stress in similar studies in the literature, this scale was preferred in our study.13,14
Statistical analysis
The statistical analysis was performed using IBM SPSS Statistics (Version 23.0; IBM Corp., Armonk, NY). Descriptive statistics included numbers and percentages for categorical variables and median, minimum, and maximum values for numerical variables. A Shapiro–Wilk test and a Kolmogorov–Smirnov test were used to assess fitness to the normal distribution, and all data in the study group were found to have a nonparametric distribution. Nonparametric techniques are based on ranks or medians. Ranks represent the relative position of an individual in comparison with others, but are not affected by extreme values (whereas a mean is sensitive to outlier values). Ranks and medians are more robust to outliers. Therefore, outlier extraction was not considered necessary in our study.
Mann–Whitney U test and Wilcoxon test were used for the comparison of nonparametric variables. Pairwise comparisons were made using Dunn's post hoc test for parameters that showed significant differences in a Kruskal–Wallis test. The correlation of continuous variables was tested using Spearman's rank correlation coefficient. A two-tailed p-value of <0.05 was considered statistically significant.
Results
Erzurum City Hospital is located in eastern Turkey and has the highest birth rate in the country, with 6,000–7,000 deliveries annually. A total of 1,506 deliveries were performed during the defined 3-month study period, of which 841 were spontaneous vaginal deliveries. The purpose and method of the study were explained to the mothers who met the inclusion criteria. After the exclusion criteria, the study was explained to a total of 261 mothers. There were 142 mothers who agreed to participate in the study. However, 52 mothers did not come to the follow-up.
A total of 90 mothers were included in the study based on the inclusion and exclusion criteria (Fig. 1), of which 30 (33.3%) delivered preterm, 38 (42.4%) delivered at term, and 22 (24.5%) delivered post-term. Of the infants, 42 (46.7%) were female and 48 (53.3%) were male. The median age of the mothers was 25 years (16–42 years), and the median duration of marriage was 2 years (1–23 years).
Of the mothers, 48 (53.4%) were primiparous and 42 (46.6%) were multiparous; 9 (10%) were employed and 81 (90%) were housewives; 16 (17.7%) were low income and 74 (82.3%) were middle–high income; and 17 (18.9%) were primary school graduates, 32 (35.6%) were secondary school graduates, 27 (30%) were high school graduates, and 14 (15.5%) were university graduates. The family type was nuclear family for 46 (51.1%) mothers and extended family for 44 (48.9%) mothers. Of the pregnancies, 82 (91.1%) were wanted and 8 (8.9%) were unwanted.
The median stress scale score of the mothers was 28 (17–50), and the median breast milk cortisol level was 0.49 ng/mL (0.1–1.96 ng/mL). There was a significant positive correlation between the stress scale score and the breast milk cortisol level (r = 0.56, p < 0.01) (Fig. 2).
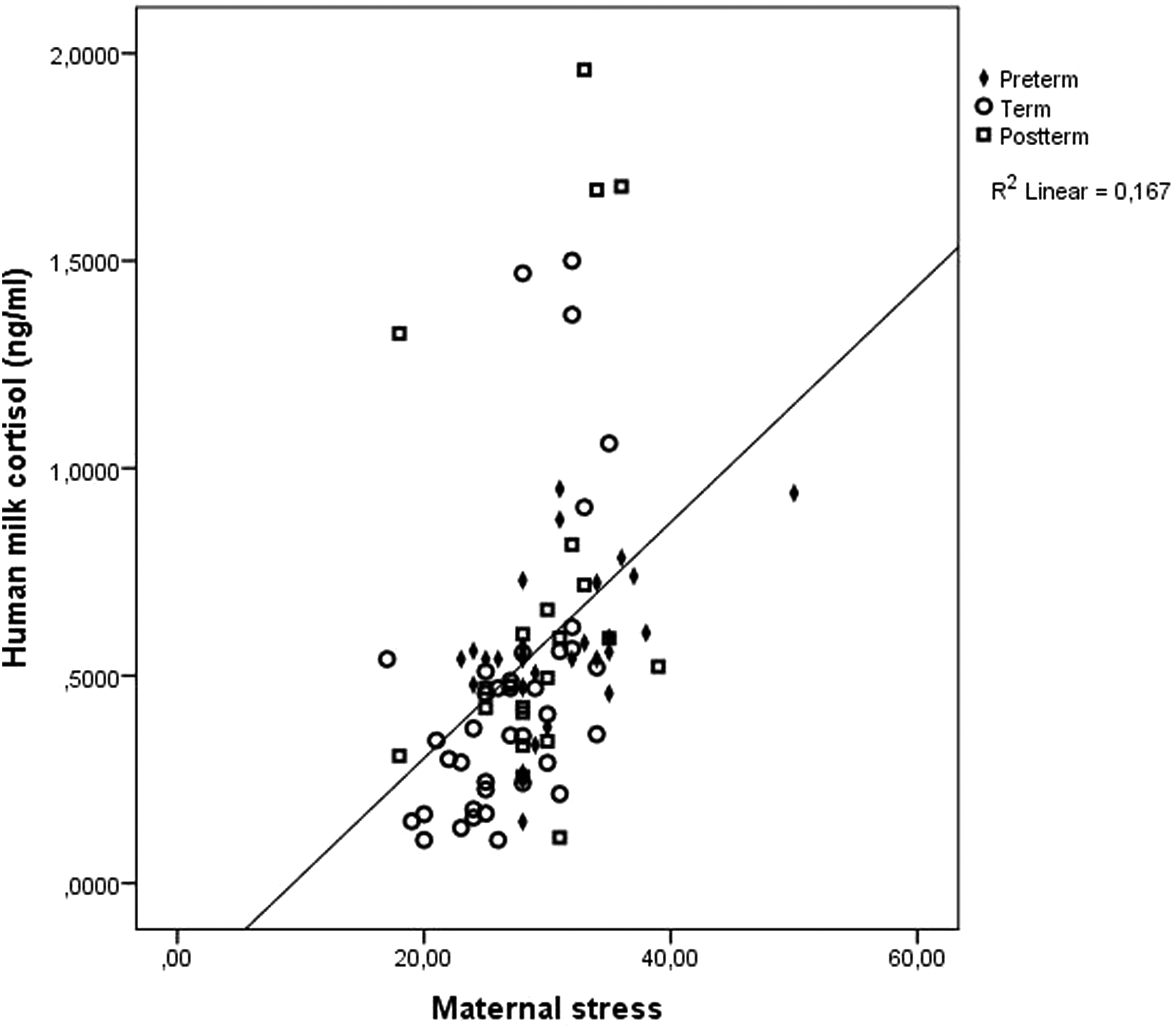
A graph showing the correlation between human breast milk cortisol level and maternal stress score.
Among the continuous variables, age and duration of marriage were uncorrelated with maternal stress score (p = 0.1, p = 0.9, respectively) or human breast milk cortisol level (p = 0.8, p = 0.93, respectively). An analysis of categorical factors revealed no significant correlation with maternal stress score or human breast milk cortisol levels (Table 1).
Maternal Categorical Factors and Their Relationship with Human Breast Milk Cortisol Levels and Maternal Stress Scores
Median (minimum to maximum).
Mann–Whitney U test and Kruskall–Wallis test were used. A p-value of <0.05 was considered statistically significant.
The gestational age of the infants at birth was evaluated for its relationship with human breast milk cortisol level and maternal stress score, revealing significant differences in the human breast milk cortisol levels and maternal stress scores of the preterm birth, term birth, and post-term birth groups (p = 0.006, p = 0.009, respectively). A post hoc analysis revealed breast milk cortisol levels and maternal stress scale scores to be significantly higher in the preterm birth group than in the term birth group (p = 0.011 and p = 0.013, respectively).
The median breast milk cortisol level was 0.54 ng/mL (0.148–0.95 ng/mL) and the median maternal stress score was 29 (23–50) in the preterm birth group; the median breast milk cortisol level was 0.36 ng/mL (0.1–1.5 ng/mL) and the median maternal stress score was 27 (17–35) in the term birth group; and the median breast milk cortisol level was 0.50 ng/mL (0.11–1.96 ng/mL) and the median maternal stress score was 30 (18–39) in the post-term birth group. Although the human breast milk cortisol levels and maternal stress scores were numerically higher in the post-term birth group than in the term birth group, the difference was not statistically significant (p = 0.57 and p = 0.101, respectively) (Table 2 and Fig. 3).
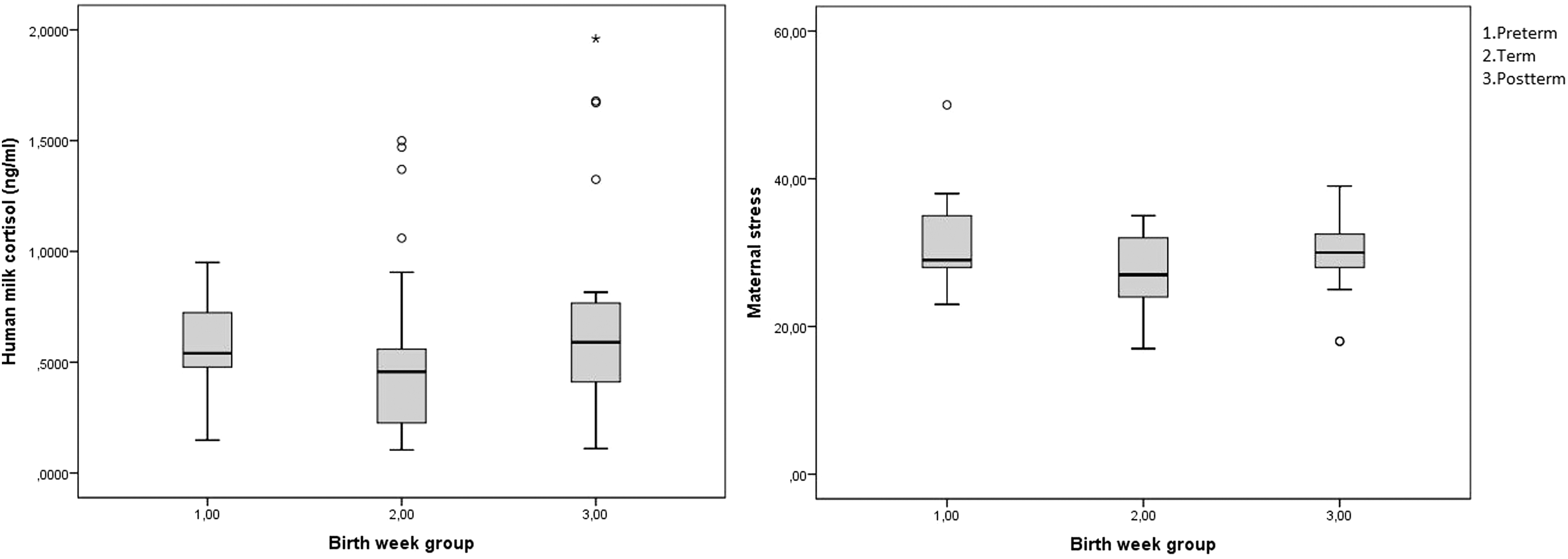
A graph showing human breast milk cortisol level and maternal stress score according to gestational age at birth. (The error bars show standard errors of the mean.)
Comparison of Human Breast Milk Cortisol Levels and Maternal Stress Scores of Gestational-Age Groups
Bold values means the significance.
Median (minimum to maximum).
Kruskall–Wallis test was used. A p-value of <0.05 was considered statistically significant.
Pairwise comparisons were performed using Dunn's post hoc test.
Discussion
In our study, we found that maternal stress and milk cortisol levels were higher in the groups with nonterm deliveries. However, there was a statistically significant difference only in the group with preterm deliveries compared with those with term deliveries. Although it is not possible to establish a cause and effect relationship between birth week and maternal stress, our results show that PSS is increased in mothers who did not give birth at term, and this may affect milk cortisol level because there was a strong correlation between maternal stress level and milk cortisol level.
There have been studies reporting a relationship between maternal prenatal stress and cortisol levels and preterm birth, 17 while there is only limited information on the relationship between postnatal maternal stress and cortisol levels in breast milk. The components in the breast milk of mothers of preterm infants are known to differ from those of the mothers of term infants. 18 In the STEPS study, the cortisol levels were found to be higher in mothers who underwent preterm labor, independent of the presence of gestational diabetes mellitus. 8 Breast milk cortisol levels in the present study were similarly higher in the preterm birth group than in the term birth group, which raises the question of the cause of the elevated cortisol levels.
In a study by Pundir et al., social and environmental factors such as educational status, employment status, income level, family type, and rural or urban residence were reported to have no effect on the cortisol levels in breast milk. 8 In a study comparing 195 mothers diagnosed with postpartum depression and 1,167 mothers without depression, Mohamad et al. reported no significant difference between the groups in terms of maternal age, educational status, infant's gender, pregnancy desire, income level, or employment status of the mother. 19 On the contrary, Clout and Brown reported that increased maternal stress was associated with cesarean delivery, maternal sleep disturbance, child health problems, and stressful life events. 20 The present study identified no relationship between the sociodemographic characteristics of the mother, stress, and breast milk cortisol levels.
In our study, preterm birth was associated with increased maternal stress and elevated milk cortisol levels. Therefore, increased stress due to preterm birth may be thought to be the cause of the increase in the cortisol levels in milk. However, in our study, it is not possible to determine whether the higher stress score in preterm birth was due to preexisting maternal stress or stress caused by preterm birth. This still does not eliminate the negative effects of stress. It has been reported that prenatal psychosocial maternal stress increases the risk of preterm birth and is associated with neonatal mobility problems.21,22 Maternal stress during pregnancy leads to increased obstetric and psychological complications.
The American College of Obstetricians and Gynecologists (ACOG) has recognized maternal stress as an independent risk factor for preterm birth and recommends that all pregnant women be monitored for psychosocial stress factors. 23 Stress occurring during pregnancy causes an increase in oxytocin, inflammatory mediators, and cytokines. Increased cortisol and catecholamines, in particular, have been associated with increased maternal and neonatal morbidities and adverse long-term effects on infant neurodevelopment.22,24 Approaches to reduce maternal stress have positive long-term effects. Mclean et al. examined 126 mothers who gave birth at <33 weeks of gestation and reported that maternal psychological stress was less in those who received family integrated care and behavior in infants improved at postnatal 18 months. 25 Although long-term effects were not the subject of our study, early detection of high maternal stress and its causes, as we found, may be instructive in terms of stress-reducing practices and treatments to be developed.
Cortisol levels in human breast milk are known to exhibit diurnal and seasonal variations.26–28 To avoid bias, breast milk samples were collected during the winter months and at the same time of day. In a study of 89 mothers of infants with a gestational age >36 weeks, Moirasgenti et al. identified a positive correlation between the cortisol levels in human breast milk and maternal stress scores (r = 0.321, p = 0.002) using the perceived stress scale introduced by Cohen et al., adopted also for the present study, but provided no data regarding seasonal variations and diurnal rhythms.13,15 In our study, the finding of a strong positive correlation between maternal stress and cortisol levels in breast milk independent of seasonal variations and diurnal rhythm further supports the body of literature suggesting that the cortisol levels in breast milk are affected by stress.
To the best of our knowledge, there have been few studies to date evaluating stress levels in mothers undergoing post-term delivery in the English language literature, and no data on the cortisol levels in breast milk in the mothers. The present study is the first in the literature to report on the stress scores and breast milk cortisol levels in mothers undergoing post-term delivery. Although both maternal stress and breast milk cortisol levels were higher in the post-term birth group than in the term birth group, the differences were not statistically significant. Post-term births are less common in pregnancies that are followed closely. The authors believe that there is a need for large-scale studies of post-term infants in centers with a high rate of unfollowed pregnancies.
The present study has certain limitations. A limited study period was applied to rule out seasonal variations with the potential to affect cortisol levels. Aside from this, certain criteria were defined to exclude endogenous stress factors. Since the PSS, which we used to measure maternal stress, evaluated the past 1 month, we could not evaluate pure postnatal stress. Only one sample could be collected on day 7 due to noncompliance of families with postnatal follow-up in our region. Since some of the preterm babies were hospitalized in the neonatal intensive care unit, the effects on stress could not be evaluated. Large-scale multicenter studies may be designed to achieve more robust data.
In conclusion, human breast milk is a bioactive compound, the composition of which changes according to the conditions. In our study, we found an association between preterm birth and maternal stress and milk cortisol levels. However, since we did not assess stress prenatally and throughout pregnancy, it is not possible to suggest whether stress causes preterm birth or preterm birth causes stress. Nevertheless, it is known that maternal stress has long-term adverse effects on the infant, and better infant development is achieved with maternal stress-reducing treatments. 25 The findings of the present study indicate the importance of providing psychological support to the mothers of preterm infants for stress control, particularly in predominantly rural regions. The authors believe there is a need for large-scale studies involving the long-term follow-up of infants and investigations of geographical variations in cortisol levels in human breast milk.
Footnotes
Authors' Contributions
S.E.T. conceptualized the study design, formal analysis, methodology, and writing. M.L. was involved in formal analysis, methodology, and editing. M.N. carried out software, formal analysis, and writing—review and editing. S.E.A. was in charge of conceptualization and writing—review and editing. K.Ş.T. contributed to study design—review and editing.
Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This study has not benefited from any financial support.