
Abstract
Background:
Nipple vasospasm is a painful cutaneous vasoconstriction that nursing mothers experience after breastfeeding.
Case presentations:
In this case series, we present the common features and management of nipple vasospasm in nursing mothers.
Discussion:
The diagnosis of vasospasm relies on the doubt of physician or the breastfeeding consultant and observation of the color change of the nipple. Persistent nipple and breast pain in breastfeeding is often attributed to Candida albicans; thus, many mothers receive antifungal therapy before the diagnosis.
Conclusions:
Timely diagnosis also prevents unnecessary antimicrobial treatments. Precise and rapid diagnosis is crucial, as pain is a risk factor for cessation of breastfeeding and its exclusivity.
Introduction
Nipple pain is a very common complaint of nursing mothers. Potential causes of persistent breast and nipple pain can be numerous; it may occur concurrently or sequentially. Nipple damage/cracks, infection, dermatosis, allodynia, or functional pain can be seen frequently. 1
Vasospasm is a spasmodic contraction of the smooth muscle, which lines the walls of the small arteries and arterioles, limiting blood flow. Vasospastic diseases of the upper extremity are commonly regarded as Raynaud's phenomenon, which was first described by Maurice Raynaud, a French physician, in 1862. The classic presentation of this phenomenon consists of triphasic or biphasic color change. Ischemia is manifested as pallor, followed by deoxygenation in severe episodes that results in cyanosis, followed by reflex vasodilatation and reperfusion manifested as erythema.2,3 The mechanisms of vasospasm remain poorly understood. In general, chronic hyperactivation of the sympathetic nervous system causes unstable vasoconstriction. Inflammatory factors are known to destabilize the homeostasis of smooth muscle contraction and relaxation in arterioles, triggering contraction. 4
Nipple vasospasm is a painful cutaneous vasoconstriction that presents itself with hardening of the nipple and color changes on a spectrum from white to blue to red. Because the innervation of the breast is complex, pain can focus in the nipple or radiate deep into the breast and may last for >30 minutes. The pain often subsides upon return of normal color to the nipple.1,5 Even though Raynaud's phenomenon may occur in approximately one-fifth of reproductive-aged women on their toes and fingers, incidence of nipple vasospasm is currently unknown.6,7
Itching, burning pain of breast, radiating and sharp pain existence between feedings, high level of sensitivity of nipple to light touch without nipple trauma or cracks can be the complaints of nursing mothers with nipple vasospasm.1,4,5 Breast and nipple-areolar complex pain can be misdiagnosed as Candida albicans. Mothers experiencing vasospasm are treated repeatedly for fungal infections.8,9 In a recent review, it was proposed that overtreatment with antifungal medications is one of a number of examples of overmedicalization of nipple pain. 10
Hyperlactation, breastfeeding with inadequate positioning, and environmental temperature changes can trigger vasospasm. 3 Sudden environmental heat change such as moving from a warm environment to a cooler environment can exacerbate pain. In the presence of these conditions, nipple must be observed. Color change in the nipple blanching to deep purple with the existence of nipple pain after breastfeeding is the diagnostic clinical finding. In differential diagnosis of nipple vasospasm, there are some cautionary clues. The color of the nipple may be lighter than normal immediately after breastfeeding as the nipple is pressed between the tongue and palate of the baby. In vasospasm although the shape of the nipple returns to normal after breastfeeding, the color change in the nipple continues.1,4
Treatment of vasospasm involves resolving any underlying persistent trauma, such as improper latch and positioning. Generally dry hot compresses after breastfeeding to breast are recommended. Cold exposure, vasoconstrictive drugs, and nicotine should be avoided. 1 Ibuprofen may help alleviate discomfort. 11 However, if the pain persists, magnesium (up to 600 mg) can be initiated to nursing mothers. Nifedipine, a calcium channel blocker, inhibits the uptake of calcium by vascular smooth muscle cells. In severe cases, nifedipine at a dose of 10–20 mg/day can be used two to three times a day for 2 weeks to relieve the pain. Longer treatment may be necessary for some women.1,5,6
The aim of case series is to present the common features and management of nipple vasospasm cases.
Materials and Methods
This study is a case series which has an observational descriptive prospective research design. It was carried out in Memorial Sisli Hospital, Breastfeeding Counselling Unit of Pediatric Department in Turkey. All children, whose mothers were provided with Breastfeeding Consultancy (BC) between October 2021 and December 2022 were included in the study. Children admitted to the Unit include infants most of which were born at the maternity clinic of the same hospital.
At the Unit, one BC nurse and a pediatrician, who is a specialist in Social Pediatrics, are working. Nursing mothers, who come to Well Child visit regularly or in need of BC can apply to the Unit. History of maternal health and breastfeeding were taken and children were examined carefully. Mother–infant dyads were assessed and BC was provided according to WHO/UNICEF 2012 Breastfeeding counselling: a training course guide. 12 Since Turkey is a country located in the northern hemisphere, we questioned the seasons and months accordingly.
The diagnosis was made by observation of the nipple color changes when mother was feeling pain after breastfeeding (Fig. 1). Dry warm compresses or heat pads were applied to breast after a breastfeed or whenever the mother experienced pain. Cold exposure to the breasts and nipples and sudden environmental changes were advised to be avoided. Smoking and use of vasoconstrictive drugs were questioned. If pain persisted despite preventive measures, nifedipine 20 mg/day for 2 weeks was initiated. 1 Before initiating nifedipine medication, mothers were consulted to cardiology department for any contraindication. Informed consent was obtained from all participants included in the study.
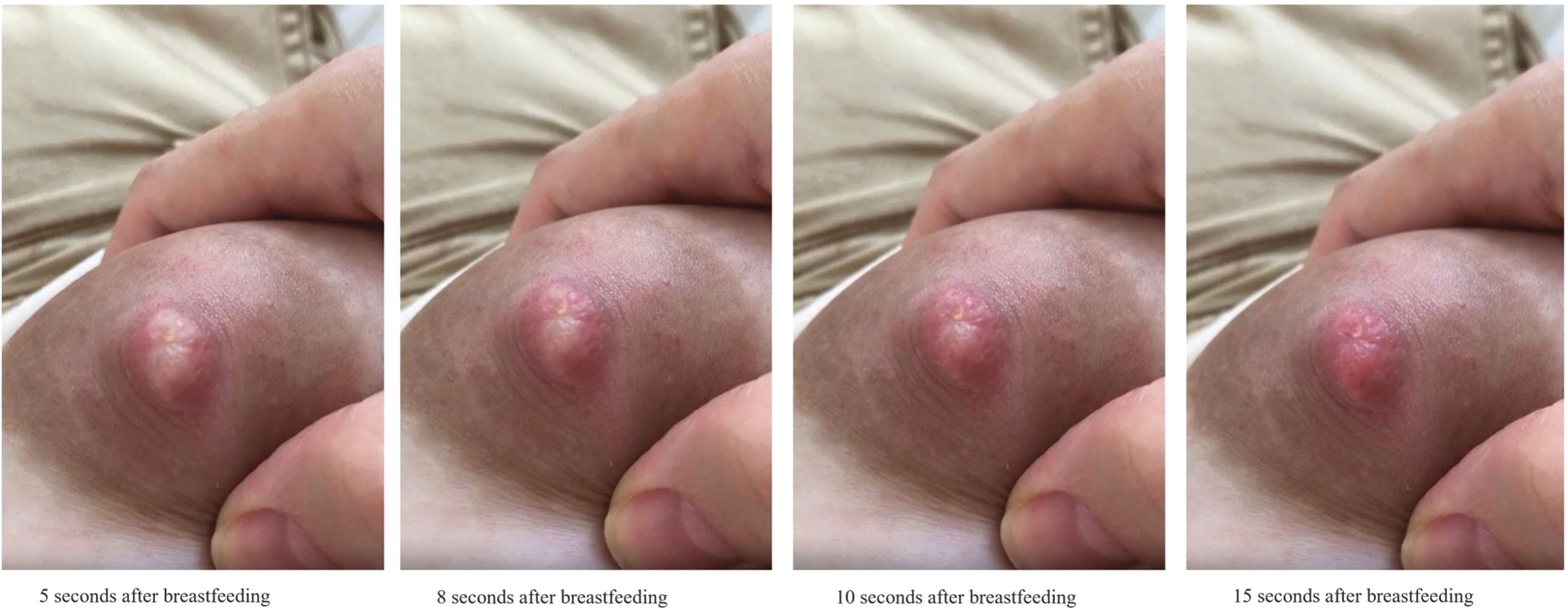
Color change in vasospasm of nipple after breastfeeding. Photos by Dr. Serap Deniz. Color images are available online.
Results
Total of 274 mother–infant dyads were consulted by the Unit during study. Of those 19.7% (n = 54) had persistent nipple pain complaint. Only seven mothers were diagnosed with nipple vasospasm. In the series, the nipple vasospasm rate was 12.9% (7/54) among mothers who had persistent nipple pain, whereas 2.5% (7/274) among breastfeeding mothers.
In all seven cases, breastfeeding was observed, and it was found that the baby was sucking effectively and the mother did not have nipple cracks. Also, no anatomical problem or oral candidiasis was observed in the baby. Detailed breakdown of the cases is given in Table 1. Only Case 2 had previous history of Raynaud's phenomenon. One mother was smoking (Case 7) and smoking cessation was recommended.
Clinical Information of Nursing Dyads
CF, complementary feeding; FF, formula feeding; NA, not applicable.
Two out of seven mothers were given antifungal therapies (Table 1). To relieve pain, two mothers (28.6%) used milk pumps. One mother had breast abscess and one mother had cracks on the nipple. Six out of seven mothers (85.7%) were primiparous. Interestingly, only Case 3 was multiparous and she experienced vasospasm when she was breastfeeding her second child. She did not have vasospasm when she was breastfeeding her first child, thus she visited dermatology and rheumatology departments before lactation consultation. She received antibiotic and antifungal therapies while she was being followed by these departments.
Six mothers benefited from dry hot compress application and avoidance of cold exposure. Only one mother (Case 3) needed nifedipine medication. Babies who were <6 months at the time of diagnosis were exclusively breastfed thereafter the diagnosis. Formula feeding cessation was achieved in all babies who were on formula supplementation. Breastfeeding continued successfully in all cases (Table 1). In cases where hyperlactation was considered block feeding was recommended; those dyads were closely monitored for plugged ducts, mastitis, and for adequate weight gain. 13
Discussion
Suspecting vasospasm in persistent nipple pain is crucial in the diagnosis. Our study emphasizes the importance of detailed breastfeeding history and physical examination of nipple in the diagnosis of nipple vasospasm in nursing mothers.
In the literature, nipple vasospasm has been reported mostly as case studies and the studies that investigated the incidence are limited. Buck et al. followed 360 mothers prospectively for 8 weeks postpartum between 2009 and 2011. They diagnosed 73 mothers with vasospasm out of 323 mothers with the incidence of 23%. 7 Barret et al. diagnosed 22 nursing mothers with vasospasm out of 88 mothers with nipple pain retrospectively for 6 years' time. The incidence was 25%. 2 Our study included 7 mothers with vasospasm out of 54 mothers with persistent nipple pain within 14 months and the incidence was 12.9%. Studies have revealed a range of 12.9–25% depending on the design and duration of the studies, number of participants, ethnicity, and their accompanying diseases.
In the first weeks of postpartum, breast pain is common but only one in five women report persistent pain at 2 months postpartum. 13 Because of the complex innervation of the breast and nipple-areolar complex, deeper breast pain may present as nipple-areolar complex pain. Candida infection has been associated with burning nipple pain or radiating breast pain symptoms. 1 There is no evidence that antifungal treatments are any more effective than the passage of time in women with these symptoms. 10 Topical antifungals and other topical agents can worsen vasospasm. 1 Two out of seven mothers had received antifungal treatments in our study. Diagnosis of vasospasm prevents mothers from taking unnecessary antifungal medications.
Pain and discomfort associated with breastfeeding is a common cause for early breastfeeding cessation. 5 Painful breastfeeding experience may be a barrier for mothers to achieve their breastfeeding duration goal. 14 In our cases, timely diagnosis of vasospasm enabled exclusive breastfeeding of the babies <6 months of age. Breastfeeding continuation was achieved in all cases.
In our case series, six out of seven mothers were primiparous. All primiparous mothers were relieved by positioning, management techniques for hyperlactation, dry hot compress application, and avoidance of cold exposure. Only one mother (Case 3) was multiparous, but she had not experienced vasospasm at her previous breastfeeding period. Hot compress application and avoidance of cold exposure were not effective in pain relief for her and nifedipine medication was initiated. Page and McKenna reported one mother who experienced nipple vasospasm while breastfeeding her second child and she was also treated with nifedipine. 6 We consider the possibility that those mothers, who had painless breastfeeding experience with their previous babies, may be more sensitive to the pain of vasospasm.
Our study was conducted for 1 year covering four seasons. All cases were reported between December and April (Table 1). This period is statistically the coolest time of the year in Istanbul. This may lead to an assumption that lower temperatures can aggregate vasospasm.
Limitations
The distribution of all nipple pain causes were not detected in the study group. Only nipple pain related to vasospasm cases were collected prospectively.
Conclusion
Nipple pain due to breastfeeding can result in early cessation of breastfeeding. Recognition of vasospasm could prevent mothers from receiving unnecessary antibiotic or pain treatments. Mothers who have vasospasm in their second or subsequent breastfeeding experiences may have different reactions compared with first-time mothers.
Footnotes
Authors' Contributions
S.D and B.K. contributed to the conception and design, acquisition, analysis, and interpretation of data, as well as with the drafting and critical revising of this article, and then approving the final version submitted for publication.
Informed Consent
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.