
Abstract
Introduction:
Infants with single-ventricle (SV) congenital heart disease (CHD) undergo staged surgical and/or catheter-based palliation and commonly experience feeding challenges and poor growth. Little is known about human milk (HM) feeding or direct breastfeeding (BF) in this population.
Aim:
To determine (1) HM and BF prevalence for infants with SV CHD, and (2) whether BF at neonatal stage 1 palliation (S1P) discharge is associated with any HM at stage 2 palliation (S2P; ∼4–6 months old).
Materials and Methods:
Analysis of the National Pediatric Cardiology Quality Improvement Collaborative registry (2016–2021) using (1) descriptive statistics for prevalence, and (2) logistic regression adjusted for multiple variables (e.g., prematurity, insurance, length of stay) to examine early BF/later HM feeding.
Results:
Participants included 2,491 infants from 68 sites. HM prevalence ranged from 49.3% any/41.5% exclusive before S1P to 37.1% any/7.0% exclusive at S2P. Direct BF ranged from 16.1% any/7.9% exclusive before S1P to 9.2% any/3.2% exclusive at S2P discharge. Prevalence varied among sites; for example, 0–100% any HM before S1P. Infants BF at S1P discharge had greater odds of any HM (odds ratio = 4.11, 95% confidence interval [CI] = 2.79–6.07, p < 0.001) and exclusive HM (1.85, 95% CI 1.03–3.30, p = 0.039) at S2P.
Conclusions:
The prevalence of HM and BF for infants with SV CHD was low and declined over time. Direct BF at S1P discharge was associated with increased odds of any HM at S2P. Wide variation suggests that site-specific practices impact feeding outcomes. HM and BF prevalence are suboptimal in this population, and identification of supportive institutional practices is needed.
Introduction
As the most common congenital anomaly, congenital heart disease (CHD) affects nearly 1 in 100 infants born in the United States. 1 Single-ventricle (SV) CHD is considered the most critical CHD and requires three-staged surgical and/or catheter-based palliations, with two occurring during infancy (i.e., neonatal stage 1; stage 2 at ∼4–6 months of age). Recent guidelines 2 highlight the importance of human milk (HM) and direct breastfeeding (BF) in protecting against disease (e.g., necrotizing enterocolitis 3 ) and developmental delay 4 in hospitalized infants. For infants with SV CHD, who experience substantial risk for these morbidities, HM and BF may be particularly essential.
However, little is known about HM and BF for infants with SV CHD. Previous studies5–13 have reported generally low prevalence in a broad range of CHD diagnoses5–7,12–14 or congenital anomalies8–11 (e.g., 35% any HM at hospital discharge 8 ), but typically include small samples from single centers. While these reports are informative, infants with SV CHD experience longer hospitalizations and more complications than those with biventricular and noncritical CHD diagnoses. 15 Furthermore, most studies do not distinguish between HM via any route and BF directly at the breast, despite the fact that direct BF improves cardiorespiratory stability during feeding for infants with CHD 16 and offers infant-specific immunological benefits. 17 Direct BF during neonatal hospitalization is associated with longer HM feeding duration for preterm infants, 18 but this association has not been examined in the CHD population.
We identified only two studies describing HM prevalence for infants with SV CHD. A multiyear Irish study 19 reported that, in 2018, 86% (n = 18) of infants with SV CHD received predominant HM at stage 1 palliation (S1P) discharge. In contrast, a 2018 U.S. study 20 found that only 15% (n = 34) of infants with SV CHD received exclusive HM at S1P discharge. Neither of these studies was primarily focused on HM or reported direct BF.
To address the gap in knowledge about HM and BF for infants with SV CHD, we aimed to determine the prevalence of these practices at time points from birth through stage 2 palliation (S2P) discharge and to test the hypothesis that direct BF at neonatal S1P discharge was associated with increased odds of HM feeding by any route at S2P. By analyzing a large, multisite SV CHD registry, this study offers foundational evidence by which to gauge future improvement in HM and BF for these vulnerable infants.
Materials and Methods
We analyzed the National Pediatric Cardiology Quality Improvement Collaborative (NPC-QIC) registry (2016–2021), which includes infants with SV CHD from >60 pediatric cardiology centers across the United States. Parental informed consent or waiver was obtained by each site for enrollment in the registry, and data were entered online by site staff. The University of Minnesota Institutional Review Board approved this study and deemed it exempt from continuing review. Infants with SV CHD who completed S1P were included. Exclusion criteria included fetal/infant demise before S1P and family choice not to pursue postnatal treatment.
Feeding practices were measured: (1) preoperatively at S1P, (2) at S1P discharge, (3) at S2P; and (4) at S2P discharge, with registry measures in Supplementary Table S1. At S2P discharge, only BF prevalence was assessable.
Definitions
We defined HM feeding as milk from a lactating person's breast, delivered via any route. The NPC-QIC registry does not differentiate between mother's own milk and donor HM. There were two HM outcomes: (1) any HM, in which an infant received exclusive HM or a combination of HM and formula; and (2) exclusive HM, in which an infant received only HM. Infant feedings were considered fortified if the recommended calorie density was ≥22 kcal/oz.
Direct BF was defined as HM directly from the breast. We use the term “breastfeeding” as it is the language in the NPC-QIC registry and acknowledge that individuals may prefer another term (e.g., chestfeeding 21 ). The BF outcomes were as follows: (1) any BF, in which an infant received exclusive BF or a combination of BF and another type/route of nutrition; and (2) exclusive BF, in which an infant received only HM from the breast.
Covariates
Covariates for models were selected a priori based on factors associated with HM or BF in the neonatal literature. These included prematurity, infant race, 22 Hispanic/Latino/a ethnicity, socioeconomic indicators 22 including social deprivation index 23 of residential zip code tabulation area (ZCTA) and insurance type, major genetic syndrome, postoperative complications, intubation duration, and S1P hospital length of stay. 8
An infant was preterm if born <37 weeks of gestational age. Response options for infant race included American Indian or Alaska Native, Asian, black-African American, Native Hawaiian, or other Pacific Islander, white, or other. Due to small numbers in some groups, response options were collapsed into black-African American, white, or another race/multirace. Insurance-type response options were collapsed into government or private/self (i.e., commercial, non-U.S., or none/self). Residential zip codes were matched to ZCTAs and used to calculate an infant's social deprivation index, 23 an indicator of potential health inequities created from the American Community Survey (e.g., % in the ZCTA living in poverty; % <12 years education).
Data analysis
Analysis of prevalence
All analyses were conducted in R (versions 4.2.1/4.2.2). We calculated the valid percentage of feeding practices at each time point. Preoperative S1P prevalence was calculated in the entire sample and in the subgroup of infants who were enterally fed preoperatively. Prevalence at S2P was calculated in the full sample, in those who were discharged after S1P, and in those who remained hospitalized until S2P. We visually examined HM/BF patterns among NPC-QIC sites.
Missing data
Across the sample, 2.3% of data were missing. We conducted multiple imputation by chained equations using the mice 24 package including variables in Supplementary Appendix SA1 and inspected imputations for convergence and plausibility. 24
Analysis of direct BF at S1P discharge and HM feeding at S2P
To determine whether direct BF at S1P discharge was associated with any or exclusive HM via any route at S2P, we fitted unadjusted and adjusted logistic regression models for each imputed data set, obtaining pooled estimates and 95% confidence intervals (CIs) using the mice package. For sensitivity analyses, we conducted the same logistic regression analyses for the subset of infants receiving any HM at S1P discharge and in the complete case, unimputed data. We tested complete case models for multicollinearity by calculating the variance inflation factor (VIF) for each included variable. All VIF values were under 1.5, indicating no issues. Statistical significance was set at p < 0.05.
Results
In 68 sites from the NPC-QIC registry, 92.5% (2,491/2,693) of infants met the eligibility criteria. Characteristics of participants at baseline are in Table 1. The median (25th–75th%) infant age was 6 (4–8) days at S1P; 39 (28–59) days at S1P discharge; 144 (123–175) days at S2P; and 162 (139–193) days at S2P discharge.
Baseline Characteristics of the Full Sample (N = 2,491)
SDI, social deprivation index; ZCTA, zip code tabulation area.
Prevalence of HM feeding and direct BF
The prevalence of HM feeding and BF at all time points can be found in Table 2. Of the 57.8% of infants who were fed before S1P, 85.7% (95% CI: 83.9–87.6%) received any HM and 27.8% (95% CI: 25.5–30.1%) were directly BF. The prevalence of HM and BF declined over time, with 37.1% (95% CI: 34.6–39.5%) of infants receiving any HM and 9.4% (95% CI 8.0–10.7%) BF at S2P. Infants who remained hospitalized between S1P and S2P had a slightly higher prevalence of HM at S2P than those discharged (39.5% versus 36.7%), but lower BF prevalence (5.7% versus 10.0%).
Prevalence of Human Milk Feeding and Direct Breastfeeding for Infants with Single-Ventricle Congenital Heart Disease at Time Points from Birth Through Stage 2 Palliation Discharge
Median (25th–75th%) age at S1P = 6 (4–8) days.
A total of 1,063 infants were not enterally fed preoperatively due to institutional policy or clinical reasons.
Median (25th–75th%) age at S1P discharge = 39 (28-59) days (1.3 months).
Median (25th–75th%) age at S2P = 144 (123–175) days (4.7 months).
Median (25th–75th%) age at S2P discharge = 162 (139–193) days (5.3 months).
Infants were considered to receive fortification if they had a recommended calorie goal of ≥22 kcal/oz.
CI, confidence interval; NC, not computable; preop, preoperative; S1P, stage 1 palliation; S2P, stage 2 palliation.
Variation in prevalence across NPC-QIC sites
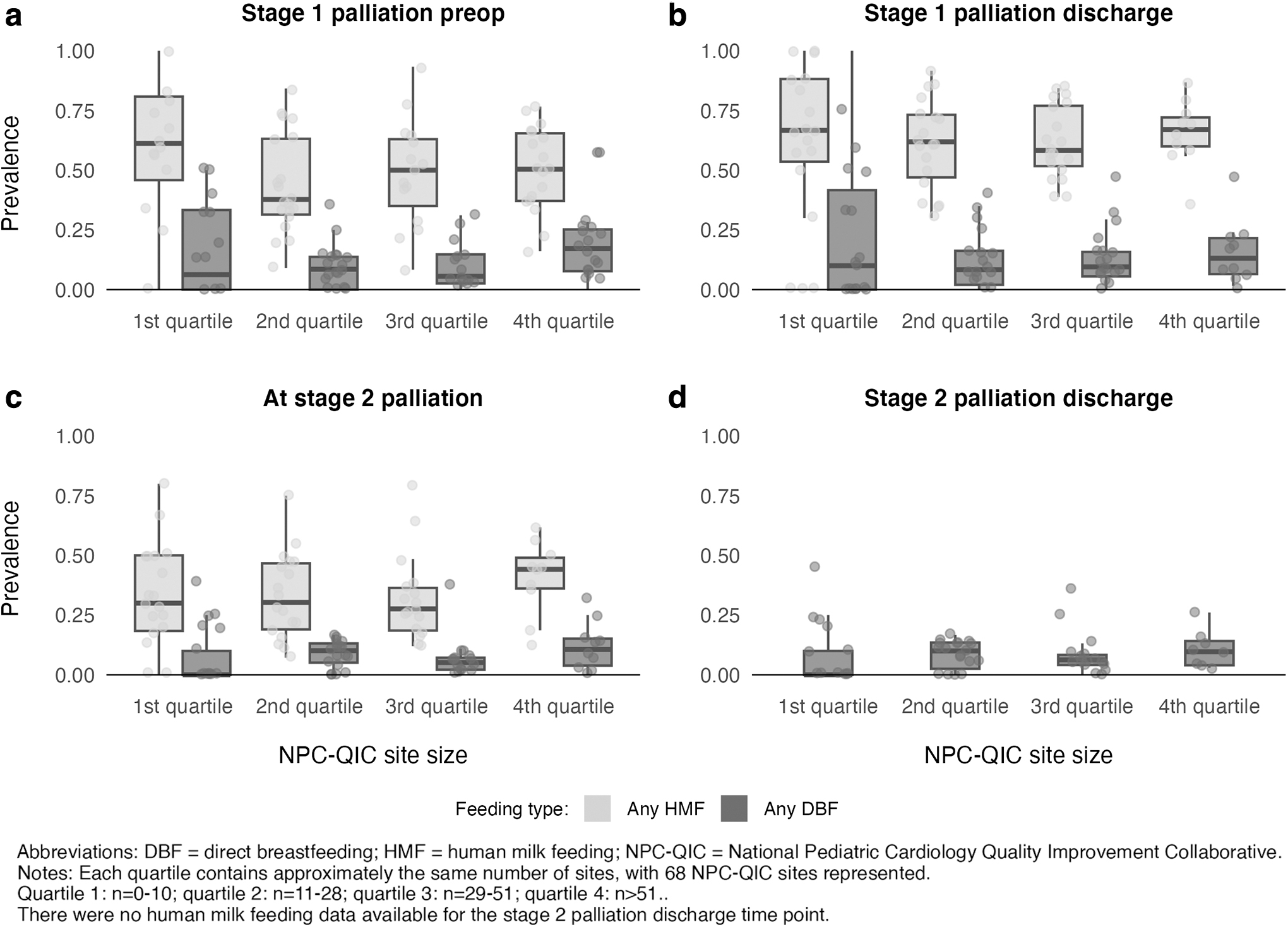
Feeding practices varied widely across NPC-QIC sites (Fig. 1). The prevalence of any HM ranged from 0 to 100.0% at both S1P time points and from 0 to 80.0% at S2P. The prevalence of any BF ranged from 0.0 to 57.8% preoperatively at S1P; 0.0–100.0% at S1P discharge; 0.0–40.0% at S2P; and 0–44.4% at S2P discharge. Figure 2 is a visual representation of this variation stratified by site size (i.e., number of patients enrolled in the registry). While there were no substantial differences based on size, the largest sites (n > 51 infants) appeared somewhat more likely to directly BF infants preoperatively. Figure 3 shows NPC-QIC sites with the top 5 highest prevalence of HM and BF at each time point.
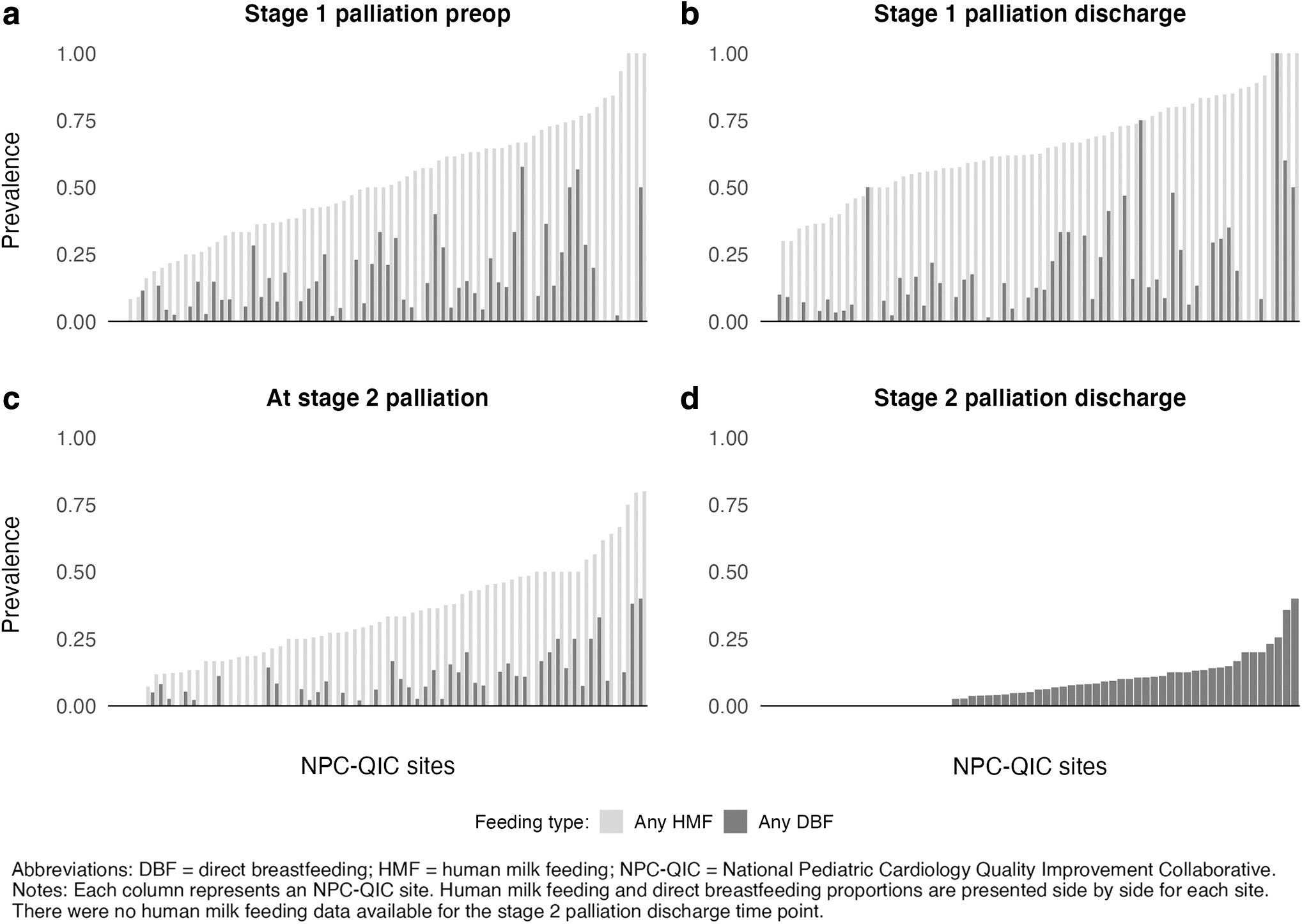
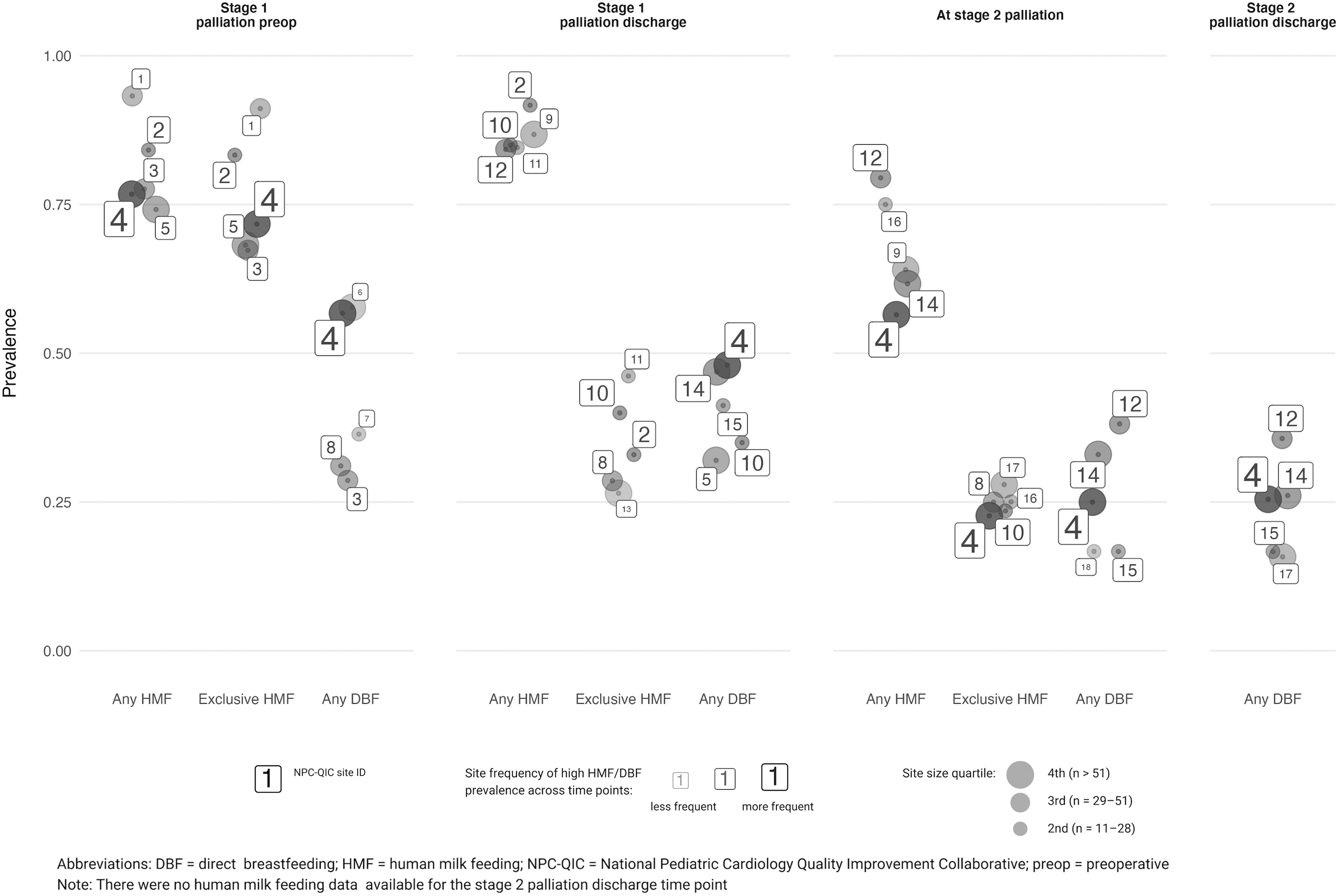
NPC-QIC sites with the top 5 highest prevalence of human milk feeding and direct breastfeeding for infants with single-ventricle congenital heart disease at each time point.
Due to the potential for skewed results in small sites (e.g., a site with n = 1 could have 0% or 100% prevalence), the 53 sites in the second to fourth size quartiles (all n > 10) are presented. Site number 4 appeared most frequently as a top 5 HM/BF site. Other sites (i.e., 2, 10, 12, and 14) also appeared across multiple time points, indicating that certain sites have consistently strong HM/BF outcomes. There were no clear patterns of high prevalence related to site size.
Association between direct BF at S1P discharge and HM feeding at S2P
A total of 1,584 infants were discharged after S1P and underwent S2P. Sample characteristics of infants receiving any versus no HM at S2P are in Supplementary Table S2. Analyses of associations between direct BF at S1P discharge and HM feeding at S2P can be found in Table 3. In both unadjusted and adjusted models, infants with any BF at S1P discharge had greater odds of HM at S2P, including 4.11 times greater adjusted odds of any HM (95% CI = 2.79–6.07 greater, p < 0.001) and 1.85 times greater adjusted odds of exclusive HM (1.03–3.30 greater, p = 0.039).
Associations Between Any Direct Breastfeeding at Stage 1 Palliation Discharge and Any or Exclusive Human Milk Feeding at Stage 2 Palliation for Infants with Single-Ventricle Congenital Heart Disease in the National Pediatric Cardiology Quality Improvement Collaborative Registry (N = 1,584)
Bold values indicate significance of the main effect at p < 0.05.
Reference for race = white; reference for insurance type = private/self. Analysis included pooled unadjusted and adjusted logistic regression using imputed data (m = 10).
SDI score = social deprivation index of the residential zip code tabulation area, an indicator of potential social health inequities (range, 0–100). A higher score indicates greater potential for social health inequities.
S1P postoperative complications included arrhythmia requiring drug therapy or a pacemaker; necrotizing enterocolitis (treated medically or surgically); neurological deficit; paralyzed diaphragm; pleural effusion requiring drainage; pneumonia; pneumothorax requiring drainage or evacuation; respiratory insufficiency requiring reintubation; acute renal failure; seizure; sepsis; stroke; vocal cord dysfunction; or wound infection.
BF, breastfeeding; CI, confidence interval; HM, human milk; OR, odds ratio; S1P, stage 1 palliation; SDI, social deprivation index.
Results of the sensitivity analyses can be found in Supplementary Table S3. For the subset of infants receiving any HM at S1 discharge, direct BF was still associated with greater odds of any HM at S2P (2.86, 1.88–4.33, p < 0.001). The results between models using imputed data and complete case models were similar in direction, with greater magnitude of effect size in complete case models.
Discussion
To our knowledge, this is the first broadscale examination of HM and BF in the SV CHD population, the first to investigate direct BF for these infants, and the largest study of HM/BF for infants with any form of CHD. Of great importance is that BF at neonatal S1P discharge was associated with increased odds of HM by any route at S2P.
Prevalence of HM feeding and direct BF
In our sample, the prevalence of HM and BF for infants with SV CHD was lower than recommended, 25 lower than the U.S. population average (i.e., 55.8% any/24.9% exclusive HM at 6 months old), 26 and declined over time. These findings are consistent with previous reports of low HM and BF prevalence for infants with CHD.
S1P preoperative HM and direct BF prevalence
For infants who were preoperatively fed in our sample, the prevalence of any HM before S1P was 85.7%, with 73.0% receiving exclusive HM. This prevalence is in line with current U.S. rates of 83.2% postnatal HM feeding initiation, 26 suggesting that lactating parents of infants with SV CHD have similar infant feeding goals as parents of infants who are born healthy. In comparison, a 2019 U.S. single-site study 27 found that 54.5% of preoperatively fed infants with various CHD diagnoses received exclusive HM. Interestingly, a 2021 study 28 at the same institution revealed that the subsequent implementation of a preoperative feeding protocol resulted in 100% exclusive preoperative HM, underscoring the key role of institutional practices in feeding these hospitalized infants.
Only 27.8% of preoperatively fed infants in our sample directly BF before S1P. To our knowledge, the only previous report on the topic is a 2004 study, 14 with 44% of infants (n = 30) BF before neonatal surgery for various CHD diagnoses. This 2004 study was conducted at a site that had implemented a system-wide lactation support program, with results representing an increase from 14% postnatal direct BF initiation before this institutional change. The comparatively lower BF rate in our study substantiates recent qualitative work 29 in which lactating parents of infants with critical CHD from 26 U.S. cardiac centers explained that, while HM expression was typically supported, direct BF was often discouraged during the neonatal hospitalization.
Direct BF as the first method of oral feeding benefits other hospitalized neonatal populations (e.g., increased HM at discharge, 30 shorter length of stay, 30 improved parental satisfaction with care29,31). While some infants with SV CHD are not physiologically able to eat by mouth, future work is needed to identify interventions to increase the prevalence of BF for infants who can be orally fed during the S1P preoperative time.
Approximately half of the infants in our sample did not receive preoperative enteral feedings due to clinical reasons or institutional policy. When considering all the infants in our sample, the prevalence of HM feeding during the early days of life was much lower than the U.S. average, at 49.3%. This is concerning, as delayed HM feeding and direct BF may negatively impact immune development 32 and the gut microbiome. 33 Considering that the SV CHD population is at risk for serious complications such as necrotizing enterocolitis, 34 this low prevalence of preoperative HM and BF warrants further attention.
Stage 1 hospital discharge HM prevalence
At S1P hospital discharge, 63.4% of infants received any HM, with only 9.3% fed exclusive HM. Previous reports of HM feeding at neonatal cardiac surgery discharge vary.8,11,19 A 2021 U.S. study 8 described 35% any HM and 21% exclusive HM at discharge in a small number of infants with CHD (n = 37). A 2021 study 11 from Brazil including 22 infants with cardiac anomalies reported 77.3% any HM and 36.4% exclusive HM at discharge. However, the diagnoses in this study were not reported and, as length of stay ranged from 3 to 66 days, it is unlikely that all infants underwent intervention. A 2022 Irish study 19 (n = 90) reported an increase in HM for infants with SV CHD at S1P discharge over time (i.e., 24% predominant HM in 2014 to 86% in 2018) due to a system-wide quality improvement project.
The prevalence of any HM at S1P discharge in our study falls between these reports; however, exclusive HM prevalence was lower in our sample than has been described, possibly due to widespread fortification practices.
HM prevalence at S2P
After S1P discharge, the prevalence of HM for infants with SV CHD dropped below the U.S. average, which is consistent with previous studies of infants with all CHD diagnoses.7,12 A 2020 Brazilian study 7 reported 40.7% any/15.7% exclusive HM at 6 months old, but included infants with CHDs that may not have required intervention. Our findings of 37.1% any/7.0% exclusive HM at S2P (median age, 4.7 months) are lower at an earlier time point, but slightly higher than Shine et al.'s 19 Irish study, in which 30% of infants with SV CHD received all/partial HM at S2P. In contrast, a 2010 Norwegian national survey 6 found that 74% of infants with moderate–severe CHD received at least some HM at 6 months.
This substantially higher rate could reflect comprehensive national BF support and high population HM feeding. 35 The disparity in prevalence between this Norwegian cohort and our sample points to socioecological factors as contributors to the suboptimal HM prevalence in our study.
Direct BF prevalence post-S1P
In our sample, the low number of infants BF before S1P declined quickly, with only 14.4% of infants BF at S1P discharge (median 1.3 months old) and 9.2% at S2P discharge (median 5.3 months old). Exclusive BF prevalence was extremely low across all time points. It is difficult to compare our results with previous studies, as there are few reports of direct BF for infants with CHD. Torowicz et al.'s 5 2015 U.S. study reported that, for infants hospitalized for CHD and receiving HM, 13% of feeds occurred via direct BF. Spence et al.'s 12 2011 Australian study found that, while almost 68% of infants with CHD were BF at hospital discharge, this number dropped to ∼30% at 6 months; however, only 59% of infants in this study underwent neonatal open-heart surgery with cardiopulmonary bypass. 12
Our results echo qualitative reports that direct BF in this population is not often prioritized by health care teams and institutions,29,36 and may be complicated by lengthy fortification and an exclusive concern about weight gain as the important outcome variable. 29
Variation among sites
We found that HM and BF prevalence varied widely among NPC-QIC sites, which is unsurprising given the documented variation in clinical feeding practice for infants with SV CHD. 37 Our findings suggest that site-specific practices have a substantial impact on feeding outcomes, which aligns with previous research identifying institutional culture and policy as key to HM and BF.28,31,38 Interventions to increase HM/BF prevalence in hospitalized neonates have been described2,31,39 (e.g., pre- and postnatal condition-specific lactation counseling; sustained skin-to-skin contact; direct BF as the first oral feed; specialized staff training), but these interventions have not been applied across settings. A cohesive, institution-wide approach to lactation support is particularly important for infants with SV CHD, whose feeding practices are heavily monitored by various teams throughout the first year of life. 29 The variation in HM feeding and BF in our sample indicates that there is substantial room for population-level improvement, despite clinical challenges inherent to this population.
Interestingly, there did not appear to be consistent differences in HM and BF prevalence based on the NPC-QIC site size. Associations between high-volume institutions and outcomes such as length of stay and postoperative complications have been demonstrated, 15 and it is plausible that larger institutions could have specialized lactation, speech, and feeding support; access to pasteurized donor HM; and experience supporting HM/BF. Alternatively, larger sites may care for high-risk infants who could be less likely to feed preoperatively. While the top-performing site in our sample was in the largest size quartile, other sites with consistently strong HM and BF prevalence varied in size.
Association between direct BF at S1P discharge and HM feeding at S2P
We found that direct BF at S1P discharge was a significant predictor of HM feeding by any route at S2P—an association that has not been previously demonstrated for infants with CHD. Our results are consistent with qualitative accounts highlighting the burden of extended milk expression 29 and with research in preterm populations. 18 These findings underscore the critical need to improve institutional support not only for HM, but also for direct BF during neonatal hospitalization for SV CHD. For these infants, who experience risk factors for necrotizing enterocolitis, infection, and neurodevelopmental delay throughout the first year of life, increased duration of exposure to the protective benefits of HM may be particularly important in optimizing health. Moreover, for many lactating parents, direct BF is deeply meaningful in ways that extend beyond nutritional and immunological concerns. 29 For these parents, institutional support of BF goals is a crucial component of care. 29
Unfortunately, a recent study 29 revealed that few U.S. institutions or providers prioritized direct BF for infants hospitalized for CHD, with many actively discouraging the practice. A consequent breakdown in trust resulted in some parents going against feeding recommendations to protect the BF relationship with their child. 29 The lack of support for parental feeding goals often exacerbated parents' psychological distress at a highly traumatic time 29 and is in opposition to individualized, family-centered, developmental care. 40
Future research is needed to identify factors that support or limit HM and BF for infants with SV CHD, thus highlighting modifiable targets for improvement. Given the variation identified in this study, investigation of institutional factors that contribute to above-average HM and BF prevalence is warranted. There is an urgent need for translational research and quality improvement to develop clinically appropriate, family-centered interventions particularly focused on the S1P hospitalization, to improve the low prevalence of HM and BF for these vulnerable infants.
Strengths and limitations
Our findings address limitations of the current evidence by focusing specifically on SV CHD; examining prevalence over time in a large, multisite sample; and distinguishing between HM feeding and direct BF. Limitations include those inherent to analysis of a national registry, including possibly inaccurate, inconsistent, or missing data. It was not possible to determine which infants were physiologically incapable of direct BF. In addition, no information was available on dose or frequency of HM and BF. It is unclear whether BF included non-nutritive practice at the breast, and oral care with HM—a common practice—was not reported. We were unable to determine whether infants fed HM received mother's own milk, donor HM, or a combination. Lastly, data on feeding practices at S1P discharge were based on the route/type of nutrition recommended by providers, but actual feeding practices by family caregivers may have differed.
Conclusion
In this study of a large national registry, the prevalence of HM and direct BF for infants with SV CHD was low and declined over time. Direct BF at neonatal S1P discharge was associated with increased odds of HM feeding by any route at the subsequent S2P. Wide variation across NPC-QIC sites suggests that site-specific practices impact feeding outcomes. HM and BF prevalence is suboptimal in this population, and future research is needed to identify factors that support or limit these feeding practices for infants with SV CHD. Evidence-based, family-centered interventions adapted for the physiological needs of this unique population are warranted. Direct BF before S1P discharge appears to be an important intervention to improve HM duration. HM/BF research is urgently needed to facilitate parental feeding goals and optimize the health of these vulnerable infants.
Footnotes
Acknowledgments
The authors would like to thank the NPC-QIC for providing the data for this study, and also Barbara McMorris, PhD, for providing helpful feedback in refining the study design.
Authors' Contributions
The authors affirm that they have each met the criteria for authorship as defined by the International Committee of Medical Journal Editors.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Institutes of Health (NINR, Award #F31NR020577). Content is the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.