
Abstract
Background:
Donor human milk (DHM) is the recommended feeding for preterm infants when mother's own milk is unavailable or insufficient. DHM macronutrient's variability may have significant implications on preterm growth. Different pooling strategies could be used to improve the macronutrient content, facilitating the achievement of nutritional requirements of preterm.
Objective:
The aim was to compare the impact of random pooling (RP) and target pooling (TP) strategies on the macronutrient content of DHM and to identify which RP practice allows the achievement of a macronutrient composition as similar as possible to that achievable with TP.
Methods:
The macronutrient content of 1,169 single-donor pools was analyzed, and a TP strategy combining 2,3,4, or 5 single-donor pools was adopted. On the bases of single-donor pools' analyses, a simulation of 10,000 randomly selected pools for each configuration of donor considered and for different milk volume proportions was performed.
Results:
Regardless of the type of strategy and milk volume, as the number of donor per pool increases, the percentage of pools with a macronutrient content equal or higher than the reference values for human milk increases.
Conclusion:
When a TP strategy is not feasible, a RP strategy combining at least five donors should be performed to obtain a better macronutrient content of DHM.
Introduction
Mother's own milk is the best option for both term and preterm infants' feeding. When mother's own milk is not available, donor human milk (DHM) is considered the preferable alternative for feeding preterm infant as recommended by the American Academy of Pediatrics. 1
The composition of human milk is dynamic and changes in relation to several factors such as method and time of milk collection, stage of lactation, and maternal diet and nutritional status. 2 Stage of lactation has an impact on the macronutrient content of human milk: protein declines during the lactation period, while fats' and carbohydrates' concentration increases. Human milk of women who delivered at term, compared to those of women who delivered prematurely, has a lower protein concentration mainly in the first 4 weeks postpartum. 3 Since DHM is commonly collected from mothers of term infants later in lactation, one major concern regarding its use for feeding preterm infants is the nutritional adequacy, particularly in terms of protein concentration. In addition, milk banking procedures, such as freezing and thawing cycles or pasteurization, can affect even more DHM composition, leading to a depletion of the macronutrients' content. 4 Frozen storage leads to rupture of the fat globule membrane, resulting in reduction of fat content and total energy, which is clinically significant when considering the nutritional needs of preterm infants. 5 In addition, the pasteurization process, a mandatory step to inactivate pathogenic microorganisms eventually present in DHM, reduces protein, fat, and energy content of unpasteurized DHM by 12.5%, 25%, and 16%, respectively.6,7
To implement the macronutrient content of DHM, Human Milk Banks (HMBs) adopt the practice of pooling, generally before the process of pasteurization. Two possible strategies of pooling are known: a target-pooling (TP) strategy, performed combining milk of single donors on the bases of their macronutrient content, and random pooling (RP) strategy, which occurs randomly regardless of the macronutrient content. The type of pooling strategy, the number of donors per pool, the type of container used to store DHM pools, and the method of mixing may also contribute to the macronutrient content of the resulting product. In their research, Friend and Perrin analyzed the potential relationship of all these factors with fat and protein content variability in DHM, and they found that, with regard to RP strategy, nonplastic containers were associated with a greater variability in proteins but not fats than plastic containers. 8 Similarly, mixing method (manual vs. mechanical) affects the variability of both fat and protein content in random pools. Instead, containers' material and mixing method did not affect nutrient variability in targeted pools.
Given that DHM is intended for the feeding of premature infants, it is important to reach a macronutrient content as close as possible to the special requirements of this kind of population, as suggested by the ESPGHAN. 9
Thus, the aim of this study was to compare the impact of RP and TP strategies on the macronutrient content of DHM. Second, we aimed to identify which RP practice allows the achievement of a macronutrient content as similar as possible to that achievable with a TP strategy.
Materials and Methods
An observational study on the macronutrient content of single donor pools of PDHM, collected by donors of the author's institution Human Milk Bank, was conducted. DHM was provided by donors between January 2018 and November 2021 following the recommendation of Italian Guidelines for the Establishment and Operation of a DHM Bank. 10 In our HMB, donation of human milk was permitted from 15th day up to 1 year after delivery both for preterm-delivering and term-delivering mothers. Before collecting their milk, all donors completed a specific questionnaire about their medical history, eating behaviors, and lifestyle; they carried out serological screening and provided a written informed consent for donation and research purpose. The study was approved by Ethics Committee of the Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico (Approval nr. 289_2017).
Collection and processing of DHM
Eligible donors collected DHM using sterile bottles provided by the hospital, and custom labels were used to identify each bottle. Each label reported information about bottle ID, donor's name, collection date, milk volume, and use of medication. All milk bottles were stored at donor's home for at least 24 hours in the refrigerator and then frozen at −20°C, before being delivered to HMB.
Before pasteurization, DHM was selected on the bases of the expiration date and was thawed overnight in a refrigerator. For each donor selected, DHM was blended until forming a batch of milk from a single donor. Each single donor pool was portioned into 130 mL bottles and then pasteurized by Holder method at 62.5°C for 30 minutes. In addition, two milk aliquots, each 1 of 10 mL, intended for microbiological and macronutrient analyses, were picked up from each single donor pool prior the pasteurization and then analyzed.
Macronutrients' and energy content was measured using a Human Milk Analyzer (HMA; Miris®, Uppsala, Sweden). This device was based on Mid-Infrared Spectroscopy, a validated and accurate method used for the measurement of human milk macronutrient content, essential for the nutritional management of preterm infants. The instrument was calibrated for breast milk measurements using the Kjeldahl method for protein, HPLC for lactose, and the Rose–Gottlieb method for fat. 11 A check procedure was implemented routinely at the start-up and after every cleaning of the instrument. Before analysis, each sample was warmed and homogenized using an ultrasonic homogenizer (Miris, Uppsala, Sweden). The temperature of milk samples, which must remain within the range of 35–40°C, was checked by a food probe. The analysis of each sample was performed in duplicate, and for the result, we considered the average of two measurements.
The concentrations of total and true proteins, fat, lactose and oligosaccharides, and total solids were obtained in grams per 100 mL and energy in kilocalories per 100 mL. The energy content was calculated considering the calorific values of protein, fat, and carbohydrates using the following formula: total energy content of 9.25 × fat +4.40 × total nitrogen +3.95 × carbohydrates. 12 The value of total protein that is referred to the total nitrogen level included all protein and nonprotein nitrogen sources. Total protein refers to total nitrogen × 6.25, and true protein is total protein minus 24% for nonprotein nitrogen.
TP and simulated RP
In our Human Milk Bank's daily practice, the TP is performed after the pasteurization, mixing single-donor pool; this strategy was adopted to limit Bacillus cereus' contamination and to reduce PDHM waste in our HMB. 13
Single donor pools of PDHM resulting in negative to microbiological analysis were mixed with each other following a TP strategy, thus selecting them on the bases of their macronutrient content. Given the published clinical reference values for human milk composition, 14 we considered as reference value for the TP the following values: 0.9 g/dL for protein content, 3.5 g/dL for fat content, 7.2 g/dL for lactose, and 65 kcal/dL for energy content.
So, multiple donor pools were created mixing different milk volumes of minimum 2 and maximum 5 single-donor pools. A 10 mL sample of the multiple donor pool was homogenized and then analyzed by Miris to obtain its macronutrient composition. This multiple donor pool is the postpasteurization pool used for feeding preterm infants.
RP strategy was simulated using combinations of 2, 3, 4, and 5 of single donor pools, as for TP. Moreover, the simulation was conducted considering both equal and different proportion of single-donor pool's volume. For different proportions of milk volume, following mix ratio was used: 1:2 for the combination of 2 donors, 1:2:3 for 3 donors, 1:1:2:2 for 4 donors, and 1:1:2:2:3 for 5 donors.
Statistical analysis
Maternal characteristics and the characteristics of the single-donor's pools composition were presented by descriptive statistics. Mean (standard deviation) and median (interquartile range) were used for continuous variables with normal and non-normal distribution, respectively. Absolute frequency (Percentage) was used for categorical variables. A simulation study was conducted to evaluate the macronutrient composition obtained by randomly selecting without replacement from the dataset k single donor pools (k = 2,3,4,5) and mixing them in equal or in different proportions (1:2 for the combination of 2 donors, 1:2:3 for 3 donors, 1:1:2:2 for 4 donors, and 1:1:2:2:3 for 5 donors). The macronutrient composition was calculated for each multiple-donor pool. We repeated this sampling 10,000 times for all k values. To categorize pools, there has been established cutoff values below the reference for each macronutrient: values <0.7 g/dL, (0.7–0.8) g/dL; (0.8–0.9) g/dL and ≥0.9 g/dL for proteins; values <6.8 g/dL, (6.8–7.0) g/dL, (7.0–7.2) g/dL, and ≥7.2 g/dL for carbohydrates; values <2.5 g/dL, (2.5–3.0) g/dL, (3.0–3.5) g/dL, and ≥3.5 g/dL for lipids; values <53 kcal/dL, (53–58) kcal/dL, (58–65) kcal/dL, and ≥65 kcal/dL for energy.
The results are presented in terms of the average content and range of the multiple donors' pool distributions, as well as the number and percentage of pools that have reached the cutoff values described above for each macronutrient. The comparison between TP and RP strategies was assessed using t test. All data were analyzed and simulations done with R software. 15
Results
During the period from January 2018 to November 2021, 409 donors were enrolled and then collected 2,500 liters of DHM, which was donated to the Human Milk Bank of the author's institution. The mean age of donors at the enrollment was 34.2 ± 4.9 years (range: 19.0–47.0), and the mean gestational age was 38.3 ± 3.0 weeks (range: 24.0–42.0). The 54.1% was primiparae, 38.8% secundiparae, and 7.1% multiparae; 71.2% of donors carried out a vaginal delivery. The 13.6% of enrolled donors delivered prematurely, and their preterm infants were hospitalized at Neonatal Intensive Care Unit of the hospital.
They started the donation at 3.0 ± 2.5 months of lactation, and they collected milk for 106.3 ± 89.7 days.
TP strategy
The average macronutrient content of 1,169 single donor pools analyzed was 0.97 ± 0.20 g/dL of proteins, 8.33 ± 0.36 g/dL of carbohydrates, 3.29 ± 1.00 g/dL of fats, and 69.12 ± 9.86 kcal/dL of energy. The distribution of macronutrients and energy of the single donor pools are showed in the Figure 1.
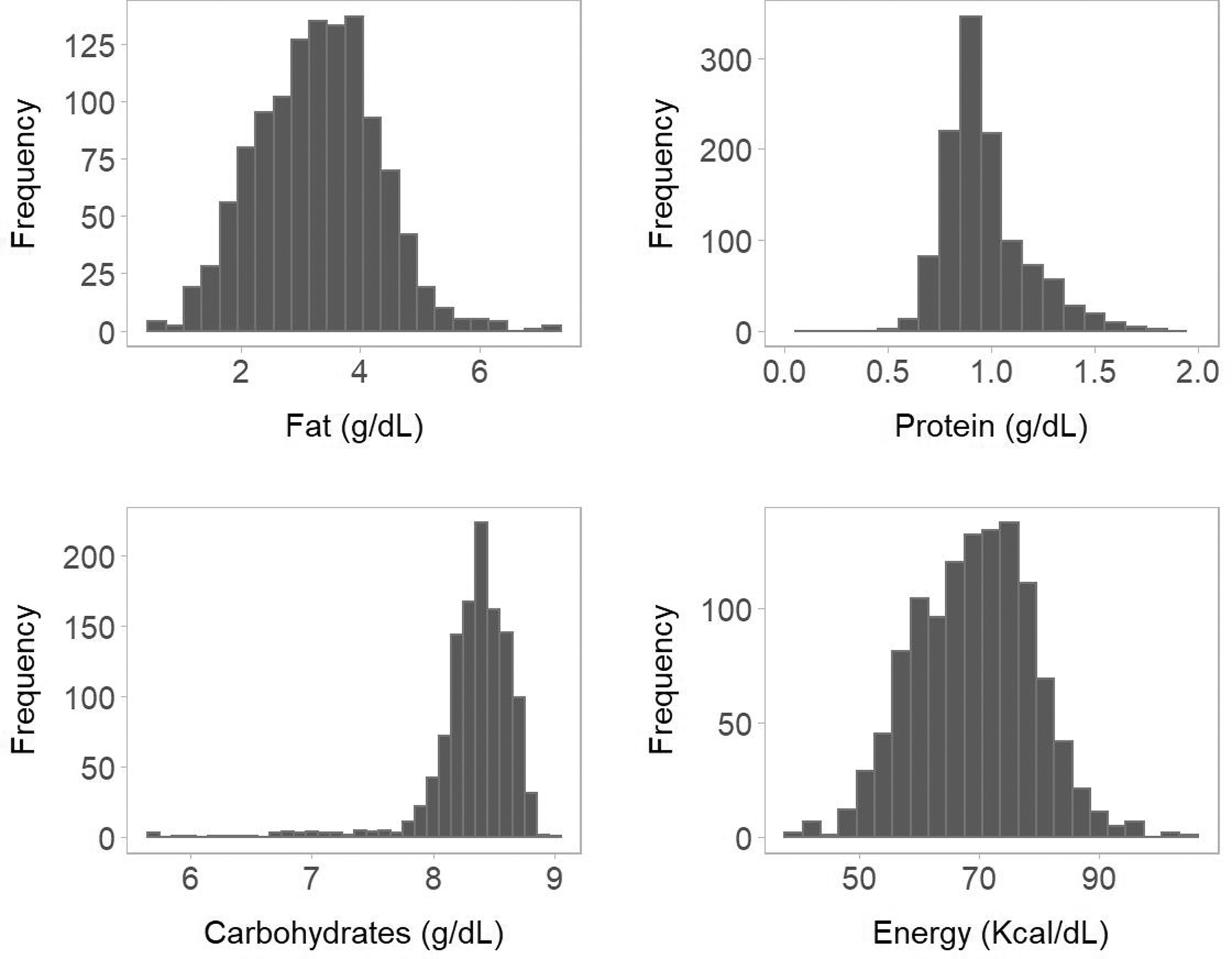
Distribution of fats
In Table 1 are presented average values of fats, proteins, carbohydrates, and energy of multiple donor pools of PDHM obtained by TP, considering combinations of 2, 3, 4, and 5 of different single donor pools.
Macronutrient and Energy Content of Multiple Donors' Pools of Pasteurized Donor Human Milk Obtained by Target Pooling Strategy
Values were described as mean ± SD (range).
SD, standard deviation.
Simulated RP strategy
A simulation study based on the single-donor pools' analyses was performed. A total of 10,000 samples of multidonor pools were randomly generated for each TP configuration, both for equal and different milk volume proportions. Average values and ranges of proteins, fats, carbohydrates, and energy of multiple donors' pools obtained from the simulation are presented in the Table 2.
Macronutrient Content of Multiple-Donor Pools of Pasteurized Donor Human Milk, Obtained by a Simulated Random Pooling Strategy, Considering Equal and Different Proportion of Milk Volumes
Values were described as mean (SD) and range.
In Table 3 are shown the percentages of pools categorized for macronutrient content, obtained by TP and RP strategy mixing equal or different milk volume of 1 to 5 donors.
Percentages of Pools Categorized for Macronutrient Content, in Relation to Type of Pooling Strategy (e.g., Random Pooling or Target Pooling), Equal or Different Milk Volume's Proportion and Number of Donors/Pool
Values were described as percentage, representative of the number of pool with a specified macronutrient content.
RP, random pooling.
Values were described as percentage, representative of the number of pools with a specified macronutrient content.
With regard to fats, as the number of donor per pool increases, the RP strategy allows a reduction of the percentage of pools with a fat concentration lower than 2.5 g/dL, independent of the milk volumes' proportion. Specifically, when 5-donor pools were created, this percentage is comparable to that obtained with TP strategy.
With regard to protein content, no pool had a concentration of proteins lower than 0.7 g/dL, independent of the type of strategy used. Considering the reference value for protein of 0.9 g/dL, as the number of donor/pool in RP increases, the percentage of pool with a protein content equal or higher than the reference increases. Specifically, when 5-donor pools were created, the percentage is closer to that obtained with TP.
Almost all pools had a concentration of carbohydrates higher than reference value, equivalent to 7.2 g/dL, both for RP and TP strategy, independent of the milk volumes' proportion.
Discussion
The results of the present study confirm the already known high variability of nutritional content of DHM.16,17 Therefore, strategies to limit this variability are advisable.
The macronutrient content in terms of fats and proteins has been found to be highly variable in our single-donor pools. Several factors could be responsible for this variability, in particular maternal factors such as gestational age, nutritional status, stage of lactation, and dietary habits.2,8 In our HMB, the majority of donors delivered at term, and they commonly collected milk from the 1st up to the 12th month of lactation, while the minority of donors delivering prematurely commonly donated in the first 2 or 3 months of lactation, given the lower volumes consumed by their hospitalized infants.
Several strategies to reduce DHM variability, thus guaranteeing a better macronutrient content, have been suggested. The TP strategy is generally the best option, especially with regards to fats and proteins. In our study, a simulated RP strategy was conducted to compare its results in terms of macronutrient content to those of TP strategy. A simulated RP strategy combining at least five donors could reduce the variability of pooled PDHM and it could allow the achievement of a macronutrient content more similar to TP and therefore to the reference values of human milk.
John et al. 18 investigated how RP affects nutrient content. They performed a simulation test to obtain 2,000 simulated pools containing DHM of 1 up to 5 donors. The authors demonstrated that as the numbers of donors in randomly simulated pools increase, the range of nutrients and, therefore, macronutrient variability decreases. Indeed, increasing the number of donor per pool, they found that more randomly simulated pools were going to meet reference values for human milk. Considering 1 g/dL protein and 3.5 g/dL fat as reference values for human milk, John and colleagues found that 28.8% of 1-donor pools fell below 1 g/dL protein, compared to 9.7% of randomly generated 5-donors' pools. Similarly, 40.2% of 1-donor pools fell below 3.5 g/dL of fat, compared to 29.3% of randomly generated 5-donors' pools.
These results are consistent with our findings. Indeed, we found that for simulated RP strategy as the number of donor per pool increases, the percentages of pool with a content of fat and protein equal or higher than the reference increase and it became closer to that obtained with TP. Specifically, with regard to protein we found that considering 5 donors, 81% (equal milk volume's proportion) and 74% (different milk volume's proportion) of simulated RP pools presented a protein content greater than or equal to 0.9 g/dL compared to 94% of TP pools. Making a comparison with results of John et al. that found that 9.7% of simulated RP pools has a protein content <1 g/dL meaning 90.3% of pool with a protein content >1 g/dL, we obtained a lower percentage although the reference we used is slightly lower. It has to be considered that the ranges for protein content are different: in our study, considering 5-donor pools the range for protein was 0.69–1.36 g/dL (considering equal milk volumes' proportion) and 0.67–1.46 g/dL (considering different milk volumes' proportion), while the range for John and colleagues was 0.8–1.6 g/dL.
With regard to fats, we found that considering 5-donors' pools, 35% (both for equal and different milk volume's proportion) of simulated RP pools presented a fat content greater than or equal to 3.5 g/dL compared to 35% of TP pools. Making a comparison with results of John et al. that found that 29.3% of simulated RP pools has a lipid content <3.5 g/dL meaning 70.7% of pool with a lipid content >3.5 g/dL, we obtained a lower percentage. It has to be considered that the ranges for lipid content are different: in our study, considering 5-donors' pools the range for lipid was 1.66–5.0 g/dL (considering equal milk volumes' proportion) and 1.64–5.02 g/dL (considering different milk volumes' proportion), while the range for John and colleagues was 2.1–5.4 g/dL. Moreover, exploring ranges below the reference for the lipid content, we found that the percentage of simulated RP pools with a fat content lower than the lower cutoff of 2.5 g/dL decreases as the number of donors per pool increases. It varies from 12% (2-donor pool) to 3% (5-donor pool) considering equal milk volumes' proportion, while for different milk volumes' proportion it varies from 14% to 4%. Thus, increasing the number of donor per pool a 10% reduction of number of pools with a very low fat content could be observed.
Almost all pools present a carbohydrate content, inclusive of both lactose and oligosaccharides' aliquots, higher than the reference value of 7.2 g/dL which is referred to lactose, both in simulated RP pools and TP pools. Hence, carbohydrates remain constantly higher than the reference (with a mean value of 8.3 g/dL) independent of the number of donors per pool, the milk volumes' proportion, and the strategy of pooling used. A recent study conducted by Young et al. 19 confirmed what both we and John et al. have found: they demonstrated that the protein content was highly variable in 1 or 2 donor pools compared to those containing 3 or more donors.
Our findings show that performing 5-donor pools, random and TP strategies could be considered comparable in terms of percentage of pools which have proteins, fats, carbohydrates, and energy content equal or higher than reference values for human milk composition. Both target-pooled DHM and DHM pooled randomly using at least five donors could provide an excellent starting point to perform an individualized fortification,20–22 with the addition of proteins and, to a lesser extent, fats. Thus, the increase in osmolality resulting from this type of fortification is marginal and this could lead to an improvement of the feeding tolerance. 23 One of the strengths of this study is the large sample size, a detailed characterization of the variability in terms of pools' macronutrient content. Furthermore another point of strength is that performing a TP strategy in a context of a standardized milk banking procedure as that used in authors' Human Milk Bank allowed to obtain a very reliable reference for the simulation of a RP strategy.
Conclusions
In conclusion, this study provides useful tips about optimal RP. This practice could be useful to be adopted when TP is not feasible, leading to a better macronutrient content and feeding tolerance of premature infants to which DHM is intended for.
Footnotes
Acknowledgments
The authors gratefully acknowledge the valuable contribution of all donors of our Human Milk Bank, who kindly support us and our NICU donating their milk.
Authors' Contributions
Conceptualization, P.R., F.M., and C.T.; methodology, P.R., P.P., C.T., and N.P.; validation, P.R., N.P., and P.P.; formal analysis, C.T. and N.P; resources, M.P, C.M., D.M., N.L., O.A., and A.O.; data curation, C.T., D.M., C.M., M.P., O.A., N.L., and A.O.; writing—original draft preparation, C.T., P.P., and D.M.; writing—review and editing, C.T, P.R., and P.P.; visualization, F.M. and P.R.; supervision, P.R.; project administration, P.R. All authors have read and agreed to the published version of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.