
Abstract
Objective:
To evaluate the effect of antenatal breast milk expression (ABE) on exclusive breastfeeding.
Materials and Methods:
A randomized control study was performed with the primary outcome being formula use during the postpartum hospital stay. Secondary outcomes were the exclusive breastfeeding rate at 6 months postpartum and peripartum safety outcomes. Participants included multiparous and nulliparous patients who planned to breastfeed. Exclusion criteria included exclusively breastfeeding in prior pregnancies for greater than 6 months, medical contraindications for breastfeeding, multiple gestation, history of preterm delivery, or any contraindication to vaginal delivery. ABE group participants were instructed to pump for 20 minutes, three times daily, starting at 37 weeks of gestation.
Results:
Three-hundred four participants from two clinics were enrolled. There was no significant difference in formula use during hospital admission (odds ratio [OR] 0.64, 95% confidence interval [CI] 0.34–1.22) or in exclusive breastfeeding at 6 months postpartum (OR 0.66, 95% CI 0.34–1.29). Colostrum use was more prevalent in the ABE group (OR 5.31, 95% CI 2.63–10.76). ABE participants were more likely to present in spontaneous labor (OR 2.09, 95% CI 1.05–4.14).
Conclusion:
ABE did not significantly improve exclusive breastfeeding rates, but safely provides women opportunities to become familiar with breastfeeding before delivery and can provide readily available colostrum. There was no negative secondary safety outcome related to ABE identified. Prenatal care providers can consider recommending ABE to patients with minimal to no experience with breastfeeding.
Introduction
Breastfeeding provides significant biological, psychological, and social benefits for birthing persons and babies. 1 The American Academy of Pediatrics recommends that infants are exclusively breastfed for 6 months after birth because of these benefits. 1 Given low 6-month exclusive breastfeeding rates in the United States, Healthy People 2030 set a goal in 2015 to increase the rate from 24.9% to 42.4%. However, the rate was only 25.8% in 2018. 2 Patient education, provision of breast pumps, and extra social support can improve breastfeeding initiation, but do not consistently increase exclusive breastfeeding rates.3,4 This gap in outcome creates an opportunity to try antenatal breast milk expression (ABE) to improve exclusive breastfeeding rates. Potential mechanisms for this improvement include earlier onset of stage II lactogenesis, perhaps by removal of colostrum and mechanical stimulation, 5 and increasing the birthing person's subjective sense of confidence in their ability to breastfeed. 6
ABE was once recommended for the preparation of breast tissue before breastfeeding in the mid-20th century, but fell out of favor with increasing formula use. 7 However, ABE is resurfacing on lactational support websites and is not typically recommended by obstetric providers. 8 A cross-sectional survey in the United Kingdom found that two-thirds of respondents had heard of ABE, but only 8% had been recommended to do so by their prenatal provider. 8 However, the survey also showed that 80–95% of patients would implement ABE if it was shown to be helpful for breastfeeding and safe in pregnancy. 8 A vast majority of studies examining various outcomes of ABE have done so using hand expression as the means of milk expression. 9 Our study aims to evaluate the effect of ABE on exclusive breastfeeding and its peripartum safety profile.
Materials and Methods
Design
This randomized prospective trial was conducted at Loma Linda University Health and approved by our internal institutional review board. We sought to evaluate the effect of antenatal breast milk expression with a dual electric breast pump from 37 weeks until delivery on exclusive breastfeeding rates in a diverse obstetric population. An electric pump modality was studied because electric pumps are used by the majority of birthing parents postpartum because of increased insurance coverage, marketing, and desire to return to work. 10
Birthing patients who desired to breastfeed were approached by research staff during routine antenatal clinic visits and invited to participate between 2020 and 2021. Patients were pre-screened for contraindications to participation through the electronic medical record (EMR). Researchers outlined the hypothesized benefits and risks of ABE, and patients who desired to participate in the trial underwent a simple 1:1 randomization after written informed consent was obtained. Battery-operated pumps were primarily supplied by the patient's medical insurance (models varied), and five units (from companies Zomee Opera and Unimom) were donated to study participants with inadequate insurance coverage. Research staff and patients were not blinded to allocation, but providers on Labor and Delivery were kept unaware of a subject's enrollment status during the peripartum admission. Data were collected from direct patient questionnaires or by review of the EMR. Enrolled patients were followed through 6 months postpartum.
Outcome variables
Our primary outcome was formula use during the hospital admission, which was based on the California Maternal Quality Care Collaborative (CMQCC) guidelines followed at our institution. 11 Secondary outcomes were exclusive breastfeeding at 6 months and birthing person-baby peripartum outcomes.
Population
The study population included nulliparous and multiparous pregnant patients who had not exclusively breastfed their prior infants for 6 or more months. Multiparous patients were included to examine if ABE could be broadly applied to improve breastfeeding rates in a low-risk birthing population, and as 6 months of exclusive breastfeeding is recommended by the American College of Obstetricians and Gynecologists (ACOG), World Health Organization (WHO), Department of Health and Human Services (DHHS), and American Academy of Pediatrics (AAP), we utilized this metric to delineate our study population.1,12–14 Participants all desired to breastfeed their babies from their current pregnancy as denoted on routine antepartum visit questionnaires.
Subjects were excluded if they had exclusively breastfed an infant from a prior pregnancy for greater than 6 months, had a medical contraindication for breastfeeding at the time of enrollment (e.g., positive urine drug screen), had a current multiple gestation, history of preterm delivery, or had any contraindication to a vaginal delivery (e.g., placenta previa or more than one prior cesarean section). In addition, subjects with infants diagnosed with cleft lip or palate, chromosomal abnormalities that would affect the ability to suckle, metabolic disorders such as phenylketonuria, or a significant heart condition were excluded from the study upon diagnosis.
Setting
Participants were enrolled from two clinics by a clinical researcher and gave birth at a single quaternary referral hospital. One clinic is a Federally Qualified Health Center (FQHC) in a large urban center, and the second is a university-affiliated private practice. Both clinics are managed by generalist obstetricians, and patients seen in a separate high-risk obstetrics clinic were not approached for enrollment. Our protocol was reviewed with all obstetric providers at our institution, and their safety concerns were discussed to minimize conflicts in counseling regarding ABE during prenatal visits.
ABE protocol
The intervention group underwent a standardized orientation through a video call session (led by ABT, RN, and KS, MD). The rationale for ABE, detailed assembly, pump troubleshooting advice, and storage information was reviewed with all ABE patients. Educational content was scripted and offered in English or in Spanish according to participant preference, who were instructed to pump both breasts simultaneously, three times per day, for 20 minutes per session, starting at 37 weeks of gestation. This script was provided to all research staff to ensure uniform application and follow-up across the duration of the trial (Supplementary Fig. S1). A brief patient handout was also provided at each training (Supplementary Fig. S2). As there was no standard protocol established at the onset of our study for electric ABE, the duration of pumping was extended beyond comparable hand expression research protocols since electric pumps are typically less extractive than hand expression due to less global compression of breast tissue. 15
Subjects were counseled about prior ABE studies, indicating that scant or no breast milk production was common.16,17 The control subjects received only standard education on lactation from their obstetric providers and peripartum lactational support at the hospital. Subjects were given 1, 3, 5, and 10 mL syringes to collect and store colostrum. Extra syringes were supplied as needed. Milk storage instructions provided to patients followed Centers for Disease Control (CDC) guidelines. 18 A paper booklet was used to record the dates, times, and amounts of colostrum pumped from 37 weeks of gestation to birth. This booklet was collected by a researcher during an in person visit during the postpartum admission or through photographs sent by text message.
Follow-up
ABE participants were instructed to bring a portion of their frozen colostrum to their hospital admission for labor, where it was kept frozen and accessible for use postpartum in the Birthing Person-Baby unit. Stored colostrum was thawed and given to the newborn through a supplemental nursing system or directly from the syringe. Control participants were able to pump colostrum postpartum, as desired, following standard unit practices, and these feedings were recorded by nursing staff in the EMR.
Peripartum data collection from the medical record was performed by trained study personnel and audited by one author (A.B.T.). A researcher visited both intervention and control groups during one to two subsequent antepartum visits to confirm participants' desire to continue in the trial, as well as in person during the postpartum admission and/or through text message for a general check-in. Postpartum encounters sought to determine individual onset of postpartum lactogenesis and reasons for formula supplementation if applicable. Control participants were asked if they implemented ABE. In-person interview was preferred over phone communication; however, this was complicated by variable researcher hospital access due to COVID-19 restrictions.
Clinical documentation from the infant's 6-month pediatric visit was reviewed to determine if they were exclusively breastfed. Age-appropriate, supplemental foods were not considered. Participants were texted in a standardized manner by a researcher if the postpartum information was inaccessible by chart review due to follow-up inconsistencies. Any formula use for any duration of time was interpreted as the participants were not exclusively breastfeeding. Patients who formally withdrew from the study were not eligible for further data collection or analysis per the informed consent protocol.
Statistical analysis
A priori power analysis for the outcome of exclusive breastfeeding was difficult to determine due to limited effect data from ABE with electric breast pumps. Based on a power of 90% and a medium effect from ABE, the estimate of sample size was 148 in total, or 74 in each intervention arm. Enrollment was over target due to high ABE subject dropout rate. Statistical analysis included the Chi-square test for categorical variables and the t-test for continuous variables. Odds ratios (OR) were calculated for variables of interest. Intention to treat analysis was performed separately to include participants randomized to ABE, which did undergo orientation, but did not express antenatally. Descriptive statistics were displayed with box plots to highlight associations between the amount of colostrum pumped or the amount of time spent pumping, and if exclusive breastfeeding was observed. Analysis was performed with Stata 17 (College Station, TX, USA) and Excel (Microsoft Corporation, 2021).
Results
A total of 304 participants underwent randomization (164 in the intervention group and 140 in the control group) (Fig. 1). Allocation between groups was unequal due to post-randomization withdrawal from the study. Per our informed consent protocol, these patients were removed from the trial. Sixty-six (40%) subjects in the ABE group completed the protocol, which was defined as any amount of ABE performed. Seventy-one patients randomized to the ABE group did not receive their orientation as outlined in the Methods. Of these participants, 34 (21%) withdrew from the study, 19 (12%) gave birth before implementing ABE or developed exclusionary criteria, and 18 (11%) were lost to follow-up prior. Four (2%) participants withdrew from the study or birthed at a different facility after their orientation and were also excluded from analysis. Eleven participants (7%) did not pump after their orientation (the most commonly cited reason was lack of time) and an additional 12 (7%) were lost to follow-up after giving birth. These 12 participants did not provide ABE data, but did deliver at our institution, so their peripartum data were available.

Consort flow diagram.
Intention to treat analysis included the 89 participants who received their orientation, did not withdraw, and had peripartum data available for review. In total, 98 (60%) patients randomized to ABE did not implement ABE. Three (2%) participants in the control group withdrew from the study, 8 (6%) were excluded because they implemented ABE on their own, and 7 (5%) were excluded due to preterm birth or developing exclusionary criteria. The dropout rate for both groups was similar between the FQHC and private practice enrollment sites.
The intention to treat analysis was essentially identical to the comparative analysis of ABE participants who successfully completed the protocol; thus, all reported results are from the comparative analysis of subjects who adhered to the protocol. The demographic distribution is listed in Table 1. Breastfeeding outcomes are listed in Table 2.
Demographics
SD, standard deviation.
Breastfeeding Outcomes from a Direct Comparison Analysis
This table excludes ABE subjects who did not adhere to the protocol.
Use refers to pumped colostrum given to the newborn infant for feeding, as opposed to direct breastfeeding from the birthing person's breast.
Indicating a significant p-value.
ABE, antenatal breast milk expression; CI, confidence interval.
The ABE group demonstrated a 30% formula use rate versus 40% formula use rate in the control group during the postpartum admission (OR 0.64, 95% confidence interval [CI] 0.34–1.22). The exclusive breastfeeding rate at 6 months was 26% for ABE participants versus 34% in the control group (OR 0.66, 95% CI 0.34–1.29). ABE participants were more likely to supplement their infants with expressed colostrum than the control group in the postpartum period (OR 5.31, 95% CI 2.63–10.76). The average amount of breast milk produced antepartum among all patients who performed ABE was 54 mL (median 6.8 mL, range 0–611 mL, n = 66). Twenty-five patients (38%) who implemented ABE did not produce any colostrum, or only produced drops that could not be collected. The amount of colostrum produced antenatally did not have a significant effect on the exclusive breastfeeding rate in the ABE arm during the postpartum hospital admission (Fig. 2). Similarly, the amount of time spent pumping antenatally was not associated with increased exclusive breastfeeding in the ABE group (Fig. 3).

Box plot examining the volume (milliliter) of colostrum expressed by ABE subjects, comparing those who did and did not supplement with formula during the initial postpartum admission. Patients who exclusively breastfed tended to produce more antepartum colostrum, but the effect was not statistically significant. ABE, antenatal breast milk expression.
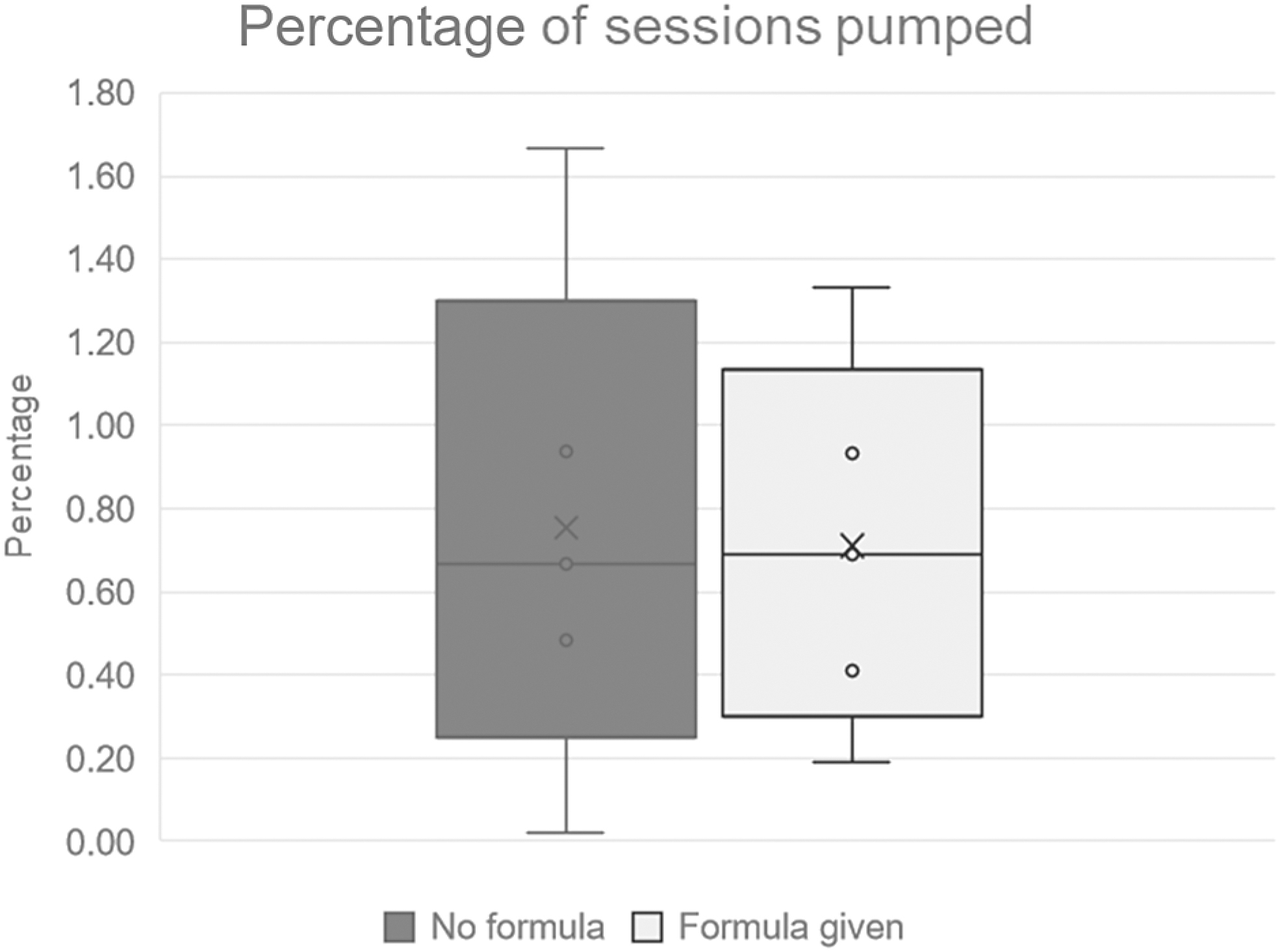
Box plot examining the percentage of sessions pumped by ABE subjects, comparing those who did and did not supplement with formula during the postpartum hospital admission. Birthing parents who exclusively breastfed pumped a similar amount of time antenatally to those who supplemented with formula. For clarification, those who pumped more than three times daily are denoted as greater than 100%.
Secondary birthing person-baby safety outcomes are listed in Table 3. There was no significant difference in safety outcomes between the ABE and control groups, including gestational age at delivery (39 weeks 2 days versus 39 weeks 0 days, p-value 0.06), infant weight loss at discharge (mean 1.4% in ABE versus 3.1% in control, p-value 0.07), 5-minute appearance, pulse, grimace, activity, respiration <6, or NICU admission rates. The rate of vaginal versus cesarean birth was similar between groups. However, the proportion of participants who presented for the peripartum admission in spontaneous labor was significantly higher in the ABE group than the control group (OR 1.97, 95% CI 1.00–3.91; p-value 0.047); the mean gestational age for this subgroup of patients was 39 weeks and 1 day. All other indications for admission were statistically similar. Postpartum onset of lactogenesis and reasons for formula supplementation were not reliably collected due to lack of response from the control group, so these outcomes were not analyzed.
Secondary Outcomes
The only outcome that differed was spontaneous labor as an admission diagnosis.
Indicating a significant p-value.
APGAR, appearance, pulse, grimace, activitiy, respiration; NICU, neonatal intensive care unit.
Discussion
Our study did not identify a statistically significant difference in formula use during the postpartum hospital stay or exclusive breastfeeding rates at 6 months postpartum either with an intention to treat analysis or a comparative analysis of ABE subjects who adhered to the protocol. Nevertheless, while our study was not powered to assess labor and safety outcomes directly, we did not observe any complication associated with ABE. Proposed mechanisms for improving breastfeeding with ABE include the use of stored colostrum during the postpartum hospital admission and improved patient self-efficacy, but these factors did not appear to have an independent effect on exclusive breastfeeding in our study.5,19,20
Our ABE participants were statistically more likely to utilize pumped colostrum for supplementation than the control arm, as control participants were allowed to pump postpartum per standard hospital practice. Our study revealed a median expressed volume of 6.8 mL, which is similar to results of the Diabetes and Antenatal Milk Expression (DAME) study, 5 mL, 16 and another randomized control trial, 5.8 mL 17 ; while DAME participants were instructed to engage in ABE twice daily for 10 minutes, our participants were instructed to aim to pump three times daily for 20 minutes.
The DAME study did find a moderate improvement in exclusive breastfeeding in a diabetic patient population when using stored breast milk from ABE, although their observed effect was only statistically significant within the first 24 hours postpartum, which their authors concluded was due to the availability of antenatally expressed breast milk. Our findings trended in that direction as well. We further hypothesized that utilizing stored colostrum at maternal request in the first few days after delivery avoids initiating the use of formula during a crucial period of lactogenesis and therefore improves breastfeeding exclusivity.
Although it was not this study's primary outcome, improvement in self-efficacy should not be overlooked. One of the strongest reported benefits to ABE in the literature is increased patient self-efficacy regarding breastfeeding and expressing breast milk.6,8,21,22 Although self-efficacy was not objectively measured in our study, anecdotal reports from participants in the ABE group support this as many women reported improved self confidence in milk production, and familiarity with breastfeeding supplies. Even participants who did not produce any breast milk antenatally, or only produced small amounts, expressed positive sentiments about preparing for breastfeeding before giving birth. Results from this study also suggest the act of putting together a pump and using it ahead of the arrival of the baby, independent of success in milk production, is valuable and contributes to confidence in breastfeeding.
Currently, most insurance companies will not provide pumps until after childbirth. The results of previous literature supported by this study suggest health care payers should consider providing access to pumps before birth to improve maternal self-efficacy, and thus potential success, in breastfeeding.
That said, nipple stimulation during pregnancy is known to cause uterine contractions due to oxytocin release and has been studied as a method to induce labor. 23 Consequently, ABE may not be recommended by some providers due to concern that it could induce labor in patients without a medical indication for early term induction. However, the implication of ABE on causing spontaneous labor has not been widely discussed in the literature. Our study did not identify differences in average gestational age at birth, cervical examination at admission, or likelihood of vaginal delivery, which is concurrent with the DAME trial. 16 Participants in the ABE group started pumping at 37 weeks of gestation and had a mean gestational age at delivery concurrent with recommended ACOG practice standards. 24 In addition, participants with prior cesarean deliveries were included in both arms of the study and no adverse safety outcome was observed for patients with uterine scar who completed ABE.
It is noteworthy that the ABE group participants were more likely to be admitted in spontaneous labor, although the effect appears small. Providers may consider counseling regarding this observation with ABE to term patients without contraindications to labor as the mean gestational age at delivery for the ABE group and the subgroup of patients who presented in spontaneous labor was more than 39 weeks.
The most significant limitations to this study are the high withdrawal rate and low completion of the protocol. Sixty percent of patients randomized to the ABE group did not pump adequately or at all. Patients cited not having time to perform ABE or being told by a family member to not perform any ABE. Among ABE participants, data collection booklets demonstrate nonuniform implementation of ABE, despite standardized individual orientation. In addition, although a similar rate of medically indicated induction occurred across both groups, we observed that medically indicated inductions cut short the available time to implement ABE for a third of our participants. Finally, a post hoc power analysis was performed to plan for another future trial. Comparing our observed improvement in breastfeeding utilizing ABE compared to regional breastfeeding data yields a necessary sample size of 4,225 patients, which is prohibitively large, given the high noncompletion rate experienced in this study.
While a majority of studies examining ABE utilized hand expression, our study incorporated the use of electric pumps. Our decision to utilize this method was due to the paucity of research in this area as well as the potential advantages of pumping over hand expressing, including, but not limited to, being less labor intensive than hand expression (e.g., could potentially be performed hands-free) and both breasts could be pumped simultaneously, which could especially benefit birthing parents with time-limiting schedules. There is also conflicting evidence as to whether a greater volume of breast milk may be expressed by the use of an electric breast pump or through hand expression.15,25,26 Nonetheless, much work is still needed to continue to examine the advantages of electric pumps and hand expression over each other.
Overall, our findings in the ABE group of increased colostrum use and anecdotal reports of increased self efficacy with breastfeeding imply that, while antepartum breastfeeding interventions such as ABE could optimize breastfeeding success, the lack of statistical significance indicates that there may be more effective interventions to improve exclusive breastfeeding rates. Previous studies have shown that improving the exclusive breastfeeding rate requires a multifactorial approach. ABE is worth considering as part of a composite strategy for optimizing breastfeeding success if a patient is interested in pursuing the practice.
Conclusion
While ABE did not show a statistically significant difference in the primary outcome of exclusive breastfeeding, there was no negative secondary safety outcome related to ABE identified even after an intention to treat analysis. As ABE provides patients with opportunities to become familiar with breast pumping techniques before birth and can provide increased access to colostrum supplementation, prenatal care providers are encouraged to provide education regarding ABE if the birthing person desires. In addition, ABE has implications for initiating spontaneous labor at term, which requires more specific study.
Footnotes
Authors' Contributions
Each author participated in various stages of the project, including implementing the study design, conducting analyses, drafting sections of the article, and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by an American College of Obstetricians and Gynecologists mini grant, and a donation of breast pumps from Unimom USA for patients without access to a pump.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.