
Abstract
Background:
Breastfeeding is widely recognized as the optimal feeding method for infants. However, breastfeeding goals are often unmet, especially in mothers with excessive weight. Potential factors associated with unmet goals could be disparities in care for women with higher body mass index (BMI) or mental health symptomology.
Methods:
Women enrolled in a longitudinal study were stratified by BMI into three groups: mothers with normal weight (18.5–24.9 kg/m2, n = 101), with overweight (25–29.9 kg/m2, n = 78), and with obesity (OB; 30–35 kg/m2, n = 48). Breastfeeding intention and standardized mental health questionnaires were administered at gestational weeks 12 and 36. The prevalence of initiation and duration of breastfeeding were determined based on self-reported breastfeeding start and end dates. Wilcoxon tests, pairwise proportion test, Cox proportional hazards regression, and linear regression were used.
Results:
Higher maternal weight status (OB) was significantly associated with lower breastfeeding intention and duration. As expected, higher breastfeeding intention scores were associated with significantly longer breastfeeding duration. Higher scores on the Beck Depression Inventory (BDI), associated with a greater number of depression symptoms, mediated the negative impact of weight status on breastfeeding intention.
Conclusions:
breastfeeding outcomes are negatively associated with maternal weight status and prenatal mental health with the relationship between the two being interconnected, despite subclinical scores on the BDI. Further research is needed to explore the role of mental health on breastfeeding outcomes. From these findings, targeted prenatal interventions for women with excessive weight and depressive symptoms would likely promote and improve breastfeeding outcomes.
ClinicalTrials.gov:
www.clinicaltrials.gov, ID #NCT01131117.
Introduction
The World Health Organization and the American Academy of Pediatrics (AAP) recommend exclusively breastfeeding for 6 months with continued breastfeeding, along with the addition of appropriate complementary foods, up to the age of 2 years.1,2 Breastfeeding serves as the biological norm for infant development. In the absence of breastfeeding, infant growth and development, the development of a healthy gut microbiome and the immune system, and disease prevention are impacted. 3 Despite the recognized benefits, in the United States, 16% of mothers never initiate breastfeeding, and of the ones who do, only 58.3% continue breastfeeding to 6 months of age.4,5 Disparities within health care affect breastfeeding success. Non-Hispanic black women have lower breastfeeding initiation and Hispanic women have early cessation risk resulting in these minority populations not achieving the breastfeeding recommendations compared with non-Hispanic white women.1,6
Other inequities have been noted to be associated with not meeting the breastfeeding recommendations, such as lower income characterized by Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) eligibility, <20 years of age, lower education level, and higher body mass index (BMI).1,6 Over the past decade, studies have shown that women with obesity (OB) in prepregnancy are less likely to initiate or meet breastfeeding recommendations than women with normal weight (NW).7–10 A cohort study from Verret–Chalifour found that mothers with OB have a twofold higher rate of not initiating breastfeeding compared with mothers with NW. 11
In 2009, Stuebe found that mothers who do not breastfeed experience increased risks of retained gestational weight gain, type 2 diabetes, myocardial infarction, and metabolic syndrome compared with prolonged breastfeeding. 12 As the prevalence of women with OB during prepregnancy continues to rise in the United States (from 26.1% in 2016 to 29% in 2019), more women will be at risk for not meeting breastfeeding recommendations and having negative postpartum health outcomes. 13
To find targets for intervention that aim to increase breastfeeding rates in women with OB, some studies have investigated whether breastfeeding intention differs among BMI groups. Guelinckx et al. reported that when reflecting on intention to breastfeed during pregnancy, significantly fewer women with OB reported intending to breastfeed along with significantly lower breastfeeding initiation and lower median breastfeeding duration compared with women with NW. 14 Another study by Marshall et al. found that mothers with OB were less likely to intend to exclusively breastfeed compared with mothers with NW. 15 Recent studies have shown that women with greater breastfeeding intentions are more likely to initiate breastfeeding and have longer duration of breastfeeding.15,16 This suggests that targeting breastfeeding intentions in women with OB may be a means to increase breastfeeding initiation and breastfeeding duration in this population.
Current research has examined the relationship between psychological factors and breastfeeding initiation and duration, but the role of BMI on this relationship is less explored.17,18 In women, a higher BMI is associated with depression and there is a positive trend between OB and anxiety disorders.19,20 Wallwiener et al. observed that increased maternal state anxiety was an important predictor of lower breastfeeding initiation. 21 In contrast, a study by Mehta et al. in 2011 found that psychological factors, such as depressive symptoms, stress, anxiety, and self-esteem, did not influence breastfeeding initiation. 22 O'Brien et al. also reported that higher anxiety was associated with earlier weaning, while observing that depression had no statistically significant relationship to breastfeeding duration. 23 Thus, further studies are needed to better understand the associations between anxiety, depression, and breastfeeding outcomes in women of diverse BMI.
The aim of this study is to investigate how BMI impacts breastfeeding intention throughout pregnancy and how psychological depression and anxiety scores during pregnancy influence intention to breastfeed when stratified by BMI. We hypothesize that BMI is negatively associated with intention to breastfeeding. We also hypothesize that women with overweight (OW) and OB are more likely to have a shorter duration of breastfeeding compared with women with NW. Finally, we hypothesize that depression and anxiety scores will negatively correlate with intention to breastfeed in women with excessive weight.
Methods
Participants
Participants were from a cohort of 284 dyads (women and offspring) enrolled in a longitudinal study, between 2010 and 2014 (www.clinicaltrials.gov, ID #NCT01131117) Recruitment criteria for participants were <10 weeks of gestation, second parity, singleton pregnancy, and >21 years of age. Exclusion criteria included smoking, alcohol use, preexisting medical conditions, sexually transmitted infections, medical conditions or medications that are known to influence fetal growth (including gestational diabetes, thyroid disease, preeclampsia), and use of fertility treatment to aid in conception. At enrollment, participants were categorized into three BMI groups (18.5–24.9 kg/m2 for mothers with NW, 25–29.9 kg/m2 for mothers with OW, and 30–35 kg/m2 for mothers with OB). Participant pregnancies were uncomplicated and infants included in study analyses were term (≥37 weeks of gestation). Study data included in this report were collected at gestational weeks 12, 36, and postpartum age 2 weeks.
Some data were not collected for every participant due to participants missing 36-week visits. Informed consent was obtained from participants before study procedures. Study approval was through the Institutional Review Board of the University of Arkansas for Medical Sciences.
Demographics
Cohort demographic information was self-reported by participants at study visits. This included maternal race, maternal date of birth, maternal education, and delivery method.
Breastfeeding outcome measurements
Breastfeeding intention scores were determined by an Infant Feeding Intention (IFI) questionnaire that was administered at gestation weeks 12 and 36. The questionnaire developed by Nommsen–Rivers and Dewey had scores that ranged from 0 to 16, with 0 demonstrating a strong intention to formula feed and 16 meaning a strong intention to breastfeed. 24 A previous study looked at IFI validity across different ethnic groups and demonstrated internal consistency in the questionnaire across groups with excellent Cronbach's alpha coefficients. 25 Breastfeeding initiation was determined if the length of breastfeeding in days was a least 1 day. Breastfeeding duration was calculated based on the participant-reported start and end date of breastfeeding.
Maternal anthropometrics
Maternal anthropometric measurements were obtained at study visits using standardized techniques. Maternal weight was obtained using a tared standing digital scale and measured to the nearest 0.1 kg. (Tanita, Arlington Heights, IL, USA). Maternal height was measured to the nearest 0.1 cm using a wall-mounted stadiometer (Perspective Enterprises, Portage, MI, USA). BMI (weight [kg]/height [m] 2 ) was calculated for all participants at enrollment. Gestational weight gain was calculated as the difference between the weight taken at the participants' 12- and 36-week study visits.
Psychological evaluation
The State-Trait Anxiety Inventory 2nd Ed. (STAI-2) and the Beck Depression Inventory II (BDI-II) were administered to evaluate participant anxiety and depression, respectively.26,27 These measures were administered and scored by state-licensed psychological examiners or psychological technicians supervised by state-licensed psychologists. The STAI comprised two subscores: State (S) for current anxiety and Trait for general or long-standing anxiety (T). The Trait component was only given once during pregnancy and the State was given at every visit. BDI was given at every visit and scores were stratified by diagnostic criteria for minimal, score of 0 to 13; mild, 14 to 19; moderate, 20 to 28; and 29–63 severe. 27 For analysis purposes, the scores from the 36-week visits were utilized due to missing data in first-trimester psychological tests.
Statistical analyses
Descriptive statistics (mean and standard deviation of the mean or counts and percentage) were calculated for maternal demographic data, gestational weight gain, gestational age, infant sex, and birth weight and length. Significance for all statistical analyses was set at p ≤ 0.05. To compare the NW group to OW and OB groups, Wilcoxon tests were used. Pairwise proportion test was used to compare breastfeeding initiation proportions for NW, OW, and OB groups. Cox proportional hazards regression with covariates was used for survival curve analysis of breastfeeding duration between BMI groups. Linear modeling was used to investigate the impact of covariates for the continuous variables of breastfeeding intention and duration. Mediation analysis was conducted with BDI score serving as the mediator between BMI and breastfeeding intent score. Statistical analysis was performed using R version 4.1.3. 28
Results
Cohort characteristics
A total of 320 women were evaluated for study eligibility, and 36 did not qualify for enrollment (Supplementary Fig. S1). Of the 284 women enrolled, 222 of these mother–infant dyads were included in the analysis, while 15 were excluded due to gestational diabetes, 10 due to miscarriage, 8 due to preterm or stillbirth, and 29 due to breastfeeding intention data not collected (Supplementary Fig. S1). There were 101 women with NW, 78 with OW, and 43 with OB (Table 1). By study design, the average BMI differed significantly between groups, with the average BMI for mothers with NW of 22 kg/m2, 27 kg/m2 for mothers with OW, and 33 kg/m2 for mothers with OB (p < 0.001, Table 1). The cohort was primarily non-Hispanic white (87%), and most had at least a partial college education (89%). The average age at delivery was 30 years (Table 1).
Cohort Characteristics' Table
BDI, Beck Depression Inventory; BMI, body mass index; IFI, Infant Feeding Intention; NW, normal weight; OB, obesity; OW, overweight.
At 36 weeks of gestation, the depression score differed significantly across BMI groups, with mothers with OB having higher scores (p = 0.044, Table 1). The average BDI score for the entire cohort (average = 6.91) demonstrated minimal depression for most women (91%, Table 1). Most mothers delivered vaginally (65%) at an average of 39 weeks of gestation (Table 1). There was a significant difference in delivery methods, with 74.3% of mothers with NW having vaginal deliveries, while only 59% of mothers with OW and 55.8% of mothers with OB delivered vaginally (p = 0.036, Table 1). There was a significant difference between groups in gestational weight gain, with women with OB having a lower weight gain compared with women with NW (p < 0.001, Table 1).
Intention
Throughout all the trimesters of pregnancy, the average breastfeeding intention score of all participants was 13, with an average score of 14 for mothers with NW, 13 for mothers with OW, and 12 for mothers with OB (Table 1). Mothers with OB had significantly lower average breastfeeding intention scores compared with mothers with NW in both the first and third trimesters of pregnancy (p = 0.015 and 0.012, respectively; Fig. 1). Mediation analysis showed that BDI significantly mediated the impact of BMI on breastfeeding intention score for the entire cohort (β = −0.026, p = 0.044; Fig. 2).

BF intention scores by BMI group (mothers with normal weight, with overweight, and with obesity) during the first and third trimesters of pregnancy.

Mediation analysis with BDI score as the mediator of the impact of BMI on BF intention scores at 36 weeks of gestation. BDI, Beck Depression Inventory.
Breastfeeding initiation
Of all the dyads, 81% of mothers initiated breastfeeding (Table 1). Within the BMI groups, 85.1% of mothers with NW, 78.2% of mothers with OW, and 74.4% of mothers with OB initiated breastfeeding (Table 1). There were no significant differences in breastfeeding initiation between the three groups.
Breastfeeding duration
Women engaged in breastfeeding for an average of 253 days (Table 1). The average breastfeeding duration for mothers with NW was 265 days, 271 days for mothers with OW, and 184 days for mothers with OB (Table 1). The average duration of breastfeeding for the mothers with OB was significantly lower than the mothers with NW and OW (p = 0.019 and 0.027, respectively; Fig. 3). Cox proportional hazards regression analysis of the probability of breastfeeding over time showed that over the 1st year of the infant's life, the probability for women with OB was significantly lower than women with NW when adjusted for maternal age, race, and education (hazard ratio = 1.51, p = 0.0495; Fig. 4; Table 2).
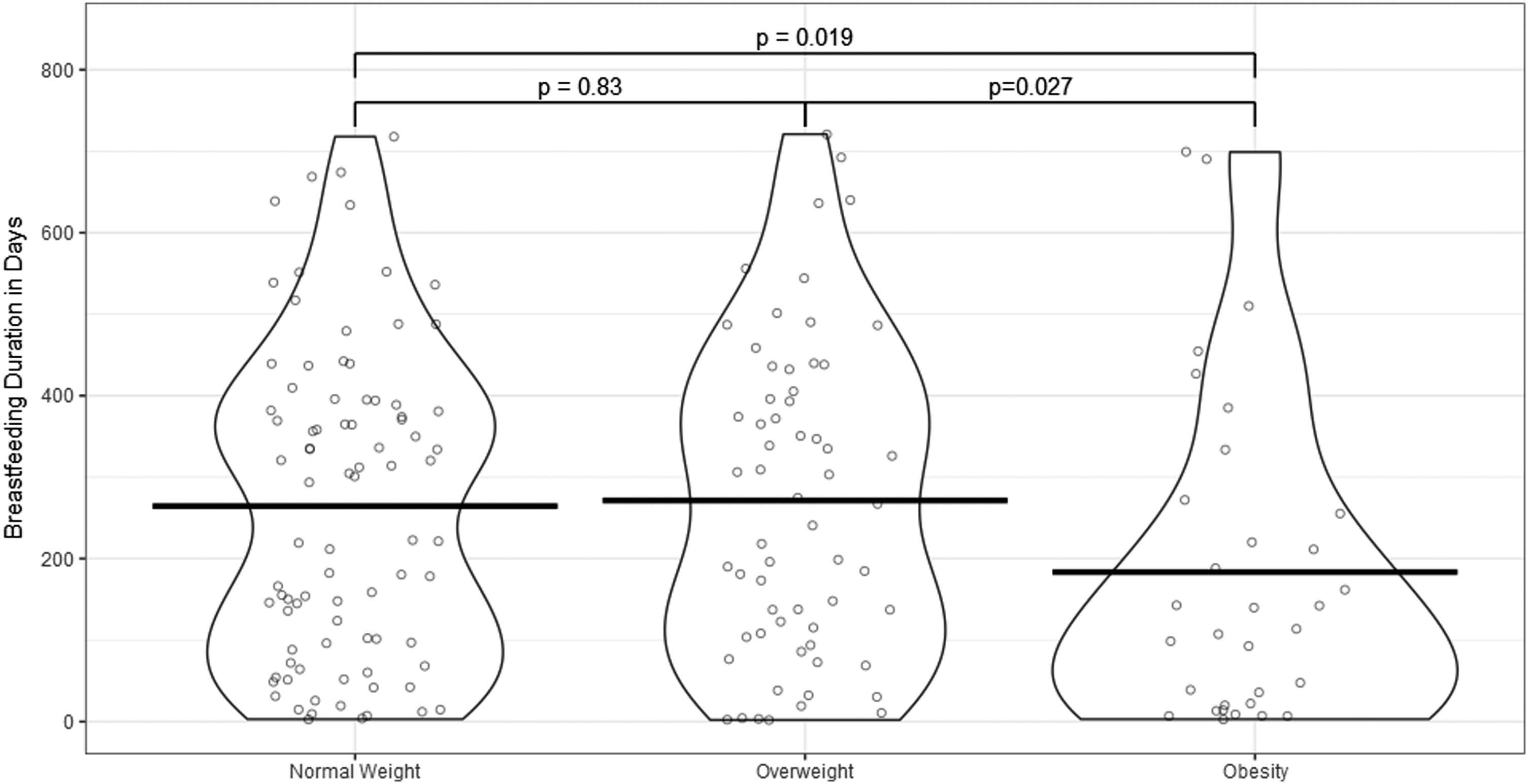
BF duration by BMI group (mothers with normal weight, with overweight, and with obesity).
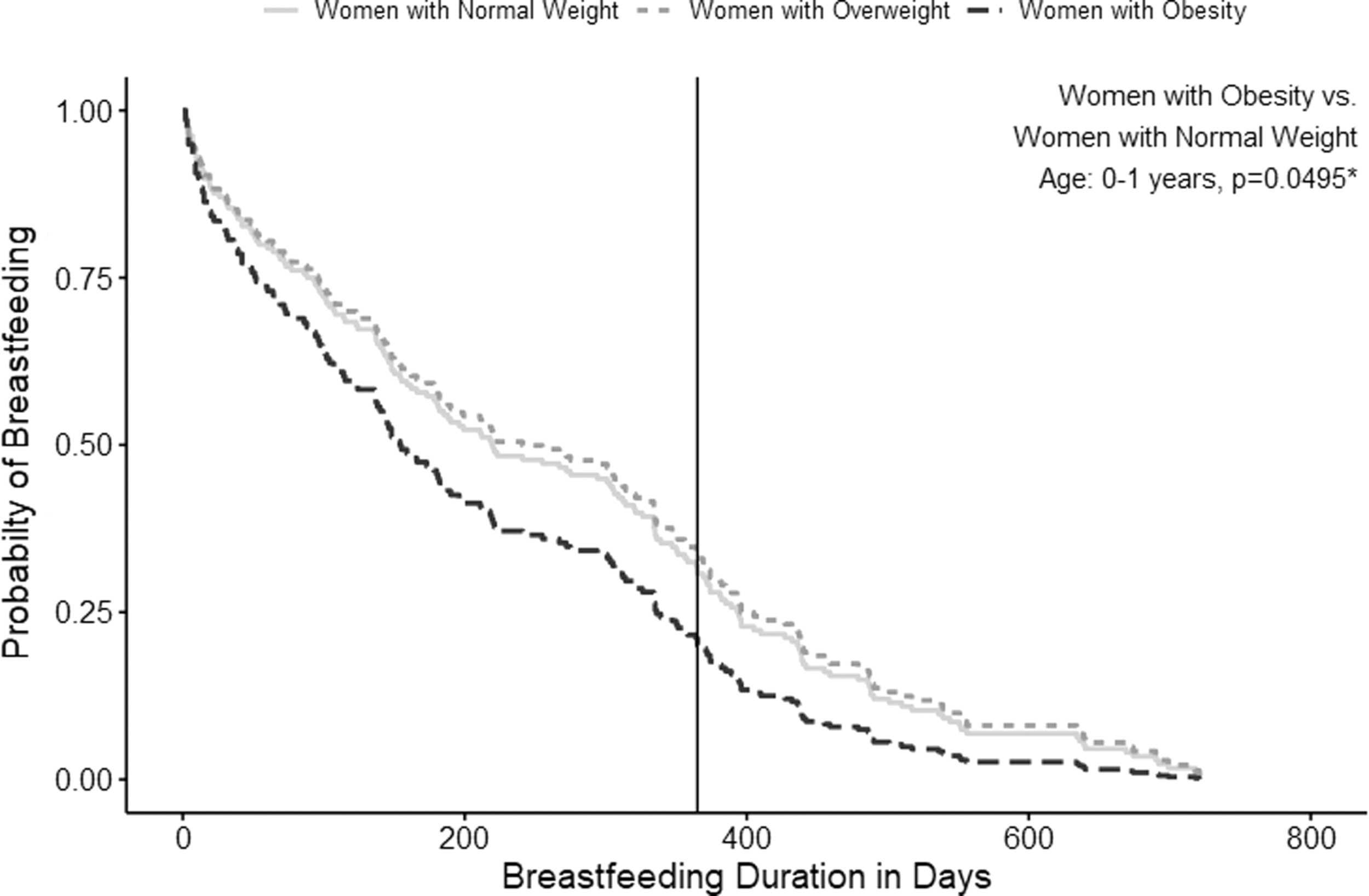
Survival curve depicting time to cessation of BF demonstrated by probability of BF at each time point. Cox proportional hazards regression analysis between BMI groups (mothers with normal weight, with overweight, and with obesity) at year 1 and year 2 of life. The model was adjusted for maternal age, race, and education.
Cox Regression Analysis of Breastfeeding Duration with Adjustment for Maternal Age, Race, and Education
CI, confidence interval.
There were no differences in breastfeeding duration probability among BMI groups during the cumulative first 2 years of life nor was there a difference between women with OW and women with NW (Fig. 4; Table 2).
Discussion
To our knowledge, this is one of the largest longitudinal studies simultaneously comparing the relationship between maternal BMI and breastfeeding intention prenatally, as well as maternal BMI and postnatal breastfeeding initiation and duration. We used standardized assessments and questionnaires to measure maternal BMI, feeding intention, maternal anxiety, and depression. We found that breastfeeding intention scores were significantly impacted by maternal BMI, with BDI scores mediating this impact. As we anticipated, breastfeeding intention scores were significantly lower among mothers with OB compared with their OW and NW counterparts. These data suggest that women with OB have a lower intention to breastfeed, and therefore are less likely to initiate and continue breastfeeding compared with their NW counterparts.
Previous studies have noted no significant relationship between breastfeeding intention and BMI or BMI group.29,30 Based on our results, breastfeeding intention score was significantly lower in women with OB compared with women with OW and NW, and the score did not significantly change between the first and third trimesters. Differences between our findings and prior literature may be due to cohort size and different societal standards, due to studies being conducted in the United Kingdom and Australia. In the context of any breastfeeding, the United States has initiation rates of 84.1% and Arkansas of 70.1%, whereas the United Kingdom has initiation rates of 81% and Australia at 96%.5,29,31 At 6 months, breastfeeding rates are higher in the United States (25.6%) compared with Australia (15.4%) and the United Kingdom (1%). 31
According to the Centers for Disease Control 2021 data, the prevalence of OB within the United States is 33% and 38.7% in Arkansas, which is higher than Australia (31%) and the United Kingdom (25.9%).32–34
There are limited studies that investigated the impact of maternal mental health on breastfeeding outcomes. One study found that higher maternal anxiety, but not depression, significantly reduced breastfeeding duration. 23 While we did not observe a relationship between maternal depression scores and breastfeeding duration, perhaps due to our cohort having low depression scores on average, we did find that breastfeeding intention was negatively associated with a higher depression score. We further found that maternal depression score mediates the negative impact of maternal BMI on breastfeeding intention, suggesting that women experiencing symptoms of depression during pregnancy may have lower intention to breastfeeding. This finding is in line with previous reports of a significant relationship between depression and breastfeeding intention. 35
While our current study and the previous work of Liu et al. differed in terms of the race and BMI of participants, and how depression was assessed, the fact that these independent studies both demonstrate a relationship between maternal depression scores and breastfeeding intention suggests an important role for maternal mental health in breastfeeding behaviors. Our current data indicate that mothers with excessive weight may be at greater risk for depression and reduced breastfeeding intention
Mothers with OB breastfed for a significantly shorter time than both mothers with OW and NW. This is in line with other studies that demonstrated that BMI is associated with reduced breastfeeding duration and with results from 9 other studies included in a systematic review.6,36,37 Our results showed that the difference between mothers with OB and OW/NW dissipates after a year and that all groups are below 25% probability by this time. This is in line with recent U.S. data on reporting breastfeeding rates of 58% and 35% at 6 and 12 months, respectively. 5 The discontinuation at 1 year could also be due to the AAP guidelines only recently being changed to 2 years of breastfeeding. Based on these results, prenatal interventions to increase breastfeeding intention, initiation, and duration in women with OB should be delivered as early as possible.
Retrospective chart review and postnatal self-reporting are the most common methodologies used by previous studies to analyze the relationship between BMI and breastfeeding practices. Strengths of our study include a large sample size (n = 222), the prenatal evaluation of intention scores at two time points, the prospective design, and the assessment of breastfeeding intention, depression, and anxiety using validated tools. A limitation of this study is that the cohort consisted of predominantly non-Hispanic white women with partial college education. Another limitation is the low incidence of mild and moderate depression in the cohort. Due to the homogenous nature of our cohort, the broader applicability of our findings may be limited.
Conclusion
The present investigation illuminates prenatal intention and BMI as the main influences of breastfeeding outcomes. Prenatal intervention strategies, which aim to increase intention scores in at-risk populations, may increase the likelihood that mothers will meet breastfeeding recommendations. Mindfulness interventions that have been observed to reduce levels of depression during pregnancy and improve prenatal well-being may be logical targets for future interventions. 38 Indeed, since a higher BDI score is negatively associated with breastfeeding intention, interventions targeting pregnant women experiencing depression symptoms may also serve to improve breastfeeding outcomes, particularly in women with OB. There are also major health disparities and inequities in breastfeeding research, and future studies in this area should focus on ethnically diverse sample populations. 39 Prospective research should explore this relationship to determine if antenatal psychological interventions may increase the likelihood that mothers will intend to breastfeeding.
Footnotes
Authors' Contributions
M.R.C. contributed to the literature review, drafted sections of the article, assisted in data interpretation, and reviewed and revised the article. M.H. and H.S. contributed to the literature review, drafted sections of the article, and reviewed and revised the article. J.B. reviewed and revised the article. C.R.S. and A.A. assisted in data interpretation and reviewed and revised the article. S.S. participated in literature review, drafted sections of the article, interpreted the data, and reviewed and revised the article. All authors reviewed the article critically for important intellectual content and approved the final article as submitted and agree to be accountable for all aspects of the work.
Disclosure Statement
The authors have no financial relationships relevant to this article to disclose. The authors have no conflicts of interest to disclose.
Funding Information
This research was funded by USDA-ARS #6026-51000-01206S.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.