
Abstract
Background:
Breastfeeding has health benefits for both mothers and children. Nipple problems may result in the child being weaned prematurely before the recommended 6 months minimum period of exclusive breastfeeding.
Purposes of the Study:
The study aimed to compare the effectiveness of topically applying olive oil and breast milk in treating nipple pain and soreness in breastfeeding mothers during the early postpartum period.
Methods:
A quasi-randomized controlled trial was conducted in a maternity ward of a medical center in northern Taiwan. Eighty breastfeeding mothers were recruited, and randomly assigned to the olive oil or breast milk group. Visual analogue pain scale (intensity of nipple pain) and nipple soreness scores were collected at 24, 48, and 72 hours after delivery. Differences in postintervention outcomes between groups were examined using the Generalized Estimating Equation model.
Results:
The results indicated that both olive oil and breast milk groups reported a significant increase in the intensity of nipple pain and nipple soreness at 24, 48, and 72 hours after delivery. However, differences in the outcome measurements between olive oil and breast milk groups were statistically insignificant at p-value >0.05.
Conclusion:
This study found that olive oil had similar effects on nipple pain and soreness to breast milk. In addition, most breastfeeding mothers provided positive feedback on using olive oil. Olive oil can be a safe, accessible, and alternative choice for breastfeeding mothers in treating nipple pain and soreness, especially early in the breastfeeding period. The Clinical Trail Registration Number: NCT03568370.
Introduction
Breastfeeding has health benefits for both mothers and children. Breastfeeding reduces the risks of not only newborn infections, sudden infant death syndrome, obesity, diabetes, and childhood and cancer1–3 but also maternal postpartum hemorrhage, type 2 diabetes mellitus, osteoporosis, and breast and ovarian cancer, and significantly lowers mortality rates and health care expenditures.4–6 Therefore, the WHO and UNICEF recommend that mothers breastfeed exclusively for 6 months, and continue breastfeeding through age two or beyond.7–9
Nipple pain or soreness is commonly reported among breastfeeding mothers. Studies have revealed that 29–76% of primiparous women experience nipple pain and soreness during breastfeeding, often occurring on the second and third postpartum days. If not properly managed, such discomfort puts breastfeeding mothers at increased risk of developing mastitis or breast abscess and further damage, which would, in turn, lead to cessation of breastfeeding.10–12
Therefore, developing effective measures for prevention and treatment of nipple pain and soreness during the early postpartum period is essential for successful breastfeeding. Several nonpharmacological methods, such as exposure of the nipples to ultraviolet light, air-drying, and application of glycerin gel, lanolin, peppermint, warm water, and breast milk, have been used to treat nipple pain and soreness; however, the effects of these preparations are controversial.11,13
Olive oil is a purely natural and pleasantly scented product with moisturizing and antibacterial properties, which is relatively cheap and easy to obtain. It contains three major components, vitamin E, polyphenols, and phytosterols, and it has moisturizing, wound healing, pain-relief, antibacterial, and antioxidant properties. Olive oil has been used as an effective and safe method for healing nipple soreness and relieving nipple pain in breastfeeding mothers.13–16
In Taiwan, health care professionals recommend lanolin cream or breast milk for treating nipple cracks and associated trauma; however, previous studies have indicated that topical application of olive oil is more beneficial than other fats and breast milk.15,17,18 To date, no study has investigated the effects of olive oil on nipple pain and nipple soreness in Taiwan. Therefore, this study aimed to compare the effect of olive oil and breast milk on nipple pain and soreness among breastfeeding mothers. The results from this study could provide a clinical practice based on scientific evidence.
Materials and Methods
Research design
A quasi-randomized controlled trial was conducted to evaluate the effect of olive oil and breast milk in treating nipple pain and soreness among breastfeeding mothers.
Participants/settings
The study was conducted in the maternity ward of a medical center in northern Taiwan, which records on average 50 to 80 births each month. Breastfeeding mothers were recruited based on the following inclusion criteria: age ≥20 years, healthy pregnancy weeks between 37 and 42 weeks, normal spontaneous delivery, breastfeeding during the first 12 hours after delivery, and willingness to participate.
Women who applied medication to the nipple, had nipple cracks, had an allergy to olive oil, and had maternal or infant health conditions that might interfere with breastfeeding, such as maternal postpartum complications or neonates requiring admittance to an intensive care unit, were excluded. The sample size was calculated based on a power of 0.8, alpha 0.05, and an effect size of 0.2. Anticipating a possible attrition rate of 5%, a target sample size of 40 participants per group was set.
Instruments
Basic information sheet
The research team developed a basic information sheet to collect sociodemographics and obstetrical data that included age, educational status, parity, mode of last delivery, and previous breastfeeding experience.
Bristol breastfeeding assessment tool
Breastfeeding assessment tool (BAT) was used to assess breastfeeding position, latch-on, sucking, and swallowing on a scale ranging from 0 to 2, “poor,” 1 indicating “moderate,” and 2 indicating “good” at the first breastfeeding session. 19 The Cronbach's alpha in this study was 0.84, and the inter-rater reliability (intraclass correlation coefficient [ICC]) was 0.67.
Breastfeeding knowledge scale
The breastfeeding knowledge scale was developed to assess breastfeeding knowledge, especially during the early postpartum period in the hospital setting. This scale contained 25 true or false questions. Correct answers received one point, while wrong and don't know answers received zero point. Scores range from 0 to 25, with a higher score indicating a higher level of breastfeeding knowledge (as supplements).
Visual analogue pain scale
Visual analogue pain scale was used to assess the intensity of nipple pain during breastfeeding on a continuum from 0 to 10. 20 Higher scores indicate worst or more severe nipple pain.
Nipple soreness score
Nipple soreness score was used to assess the severity of nipple soreness during breastfeeding, on a 6-point scale (0–5), where 0 indicates “no soreness,” 1 “slight soreness,” 2 “moderate soreness,” 3 “pain,” 4 “involuntary gasping,” and 5 “great pain.” Higher scores indicate more severe nipple soreness. ICC value in this study was 0.79. 21
Structured interview guide
The research team developed a structured interview guide to better understand the breastfeeding experience after applying olive oil and assess participants' willingness to use olive oil to reduce future nipple pain and trauma.
Study procedure
Participants who met inclusion criteria were informed individually about the study's purpose, procedure, and their rights to withdraw at any time by a trained senior registered nurse. Upon completion of the written consent form, participants were randomly assigned to either the olive oil or breast milk group according to the block randomization using an online tool (sealed envelope) identified at the start of the study.
To prevent the crossapplication of interventions and other potential biases, we chose a room as the unit of random allocation to ensure that only one type of intervention would be applied to eligible participants in a shared room. To ensure consistency of the evaluation, the first author evaluated breastfeeding performance and nipple soreness with the research nurse before the beginning of the study until obtaining the same results from three postpartum women consecutively.
All participants received routine postpartum care that included one-to-one instruction on skin-to-skin contact, breastfeeding principles, breastfeeding techniques, and pain management with 500 mg of acetaminophen four times a day. During baseline evaluation, the basic information sheet was used to collect demographic data; Bristol BAT and breastfeeding knowledge scale were used to assess breastfeeding performance and knowledge. The application of olive oil and breast milk was under the guidance of research nurses. Participants were able to demonstrate the procedure on their own body or on a breast model, allowing the research nurse to ensure that they fully understood the procedure and the application correctly.
In the breast milk group, participants were instructed to apply breast milk frequently to the nipples and areola after each breastfeeding. In the olive oil group, participants were offered a bottle (∼30 mL) of extra virgin olive oil, and instructed to apply two to three drops of olive oil to the nipples and areola after each breastfeeding. All participants were asked not to apply any other formulation to their breast.
Follow-up data on nipple pain and soreness, and breastfeeding frequency were collected at 24, 48, and 72 hours after delivery by a trained research nurse. Participants in the olive oil group were interviewed regarding their breastfeeding experience after applying olive oil, and their willingness to use olive oil to reduce future nipple pain and trauma.
Data management
Data were analyzed using SPSS for Windows version 22. Independent sample t-tests and chi-square tests were used to evaluate the differences between groups in sociodemographics and obstetric variables. Generalized Estimating Equation (GEE) model was employed to control for the effects of study covariates, breastfeeding knowledge, breastfeeding performance, and frequency of breastfeeding, and analyzed the independent effects of olive oil. A p-value of <0.05 (two tailed) was considered statistically significant.
Ethical considerations
Hospital Institutional Review Board and nursing and maternity departments approved this study (IRB No. 1-106-05-131). Each participant was informed in detail about the study's purpose and importance. Participants were assured that their data would remain anonymous and confidential, and they had the right to withdraw from the study at any time without giving any reason. Before data collection, written informed consent was obtained from each participant. All collected data were properly stored and secured, and used exclusively for academic research purposes.
Results
Of 106 postpartum women approached, 24 women who did not meet the inclusion criteria were excluded, and 2 refused to participate for personal reasons. Therefore, 80 subjects participated in the study, with 40 participants assigned to the breast milk group and 40 to the olive oil group. Table 1 describes the 80 participants' sociodemographics and obstetrical characteristics. The mean age of the 80 subjects was 32.03 ± 4.48 years. The breast milk and olive oil groups did not differ statistically in sociodemographics, obstetric variables, past breastfeeding experience, initial BAT score, or breastfeeding knowledge scale score (p > 0.05).
Participants' Backgrounds and Obstetrical Information (N = 80)
Table 2 presents the descriptive results of nipple pain and nipple soreness at 24, 48, and 72 hours after delivery across the two groups. The results indicated that both groups reported a significant increase in nipple pain and nipple soreness scores at 24, 48, and 72 hours after delivery (Figs. 1 and 2). The mean score of nipple soreness in the olive oil group was significantly lower than that in the breast milk group at 48 hours after delivery (t = 1.42, p < 0.05).
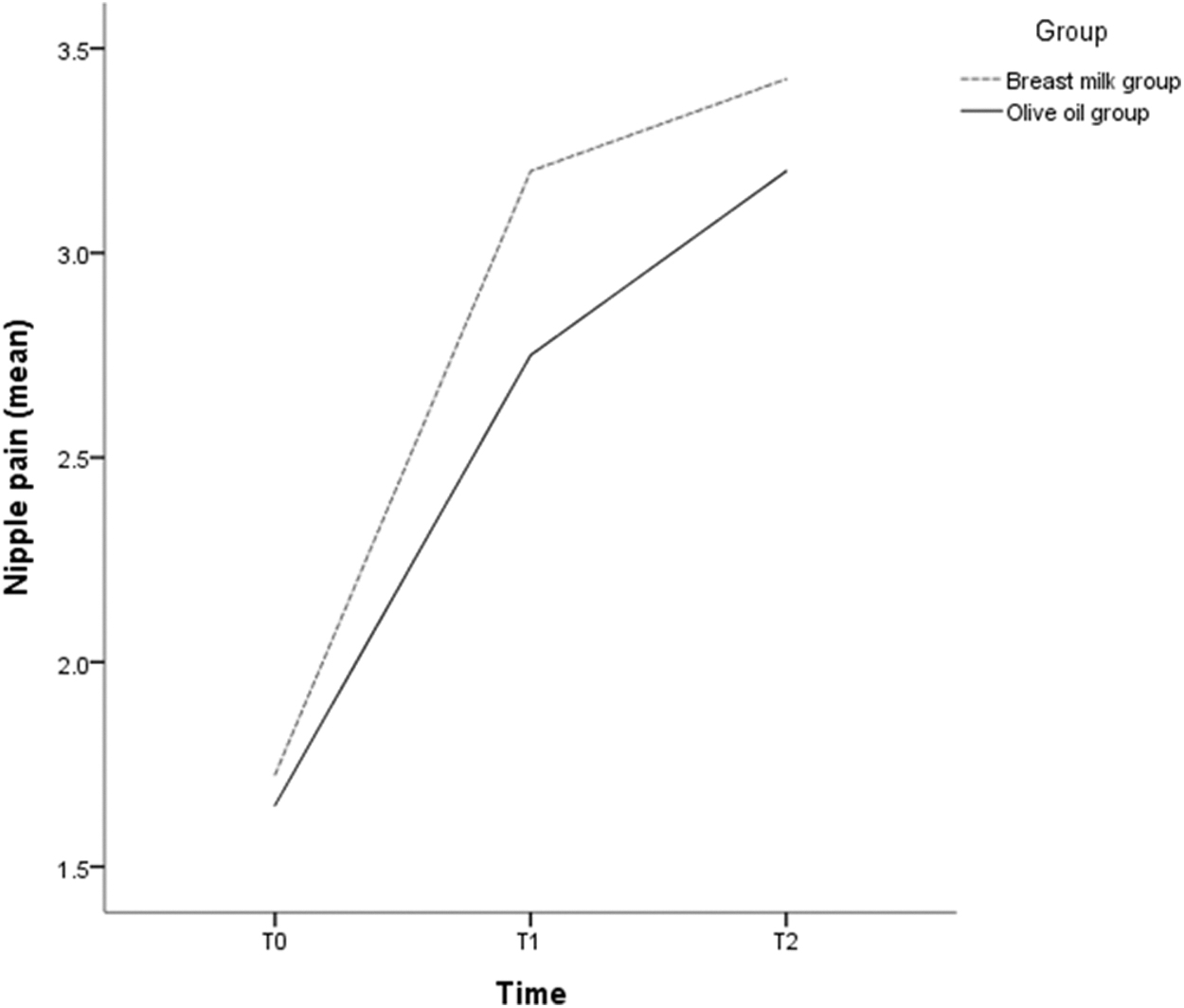
Changes in nipple pain scores at T0 (24 hours after delivery), T1 (48 hours after delivery), and T2 (72 hours after delivery).

Changes in nipple soreness scores at T0 (24 hours after delivery), T1 (48 hours after delivery), and T2 (72 hours after delivery).
Participants' Nipple Pain and Nipple Soreness at 24, 48, and 72 Hours After Delivery (N = 80)
Table 3 presents the GEE analysis of the effect of breast milk and olive oil on treating nipple pain and soreness. The results of GEE showed no significant differences between the olive oil and breast milk groups in the mean nipple pain scores (β = −0.08; p > 0.05). Time-dependent changes indicated an increasing trend of nipple pain and soreness scores.
Generalized Estimating Equation Model on the Effects of Outcome Variables for Olive Oil Application (N = 80)
The interaction effect (group difference and time) on nipple pain revealed no significant difference between the olive oil and breast milk groups (p > 0.05). The olive oil and breast milk groups did not differ significantly in the mean nipple soreness scores (β = −0.16; p > 0.05). Time-dependent changes indicated an increasing trend of nipple soreness scores. The interaction effect (group difference and time) on nipple soreness scores revealed no significant difference between the olive oil and breast milk groups (p > 0.05).
In addition, this study interviewed participants in the olive oil group using one open-ended question to understand their experience of using olive oil. Most women provided positive feedback on using olive oil, claiming that nipple pain and redness during the initial stages of breastfeeding had improved substantially, nipples had enough moisture, olive oil offered an extra layer of protection for nipples, olive oil smelled fresh, and the baby more enjoyed breastfeeding.
Discussion
Research shows that 34–96% of breastfeeding mothers experience nipple pain and soreness, which leads to premature breastfeeding cessation.10,12,22 For health care professionals, providing effective, accessible, and inexpensive interventions to manage nipple pain and soreness is important in clinical practices.
Olive oil is an easily accessible and relatively cheap substance. Several research studies have demonstrated that olive oil effectively reduces nipple pain and soreness without adverse effects observed on mothers and newborns.14,16–18 This study aimed to compare the effectiveness of the topical application of olive oil versus breast milk on nipple pain and soreness in a Taiwanese population. Results obtained from this study suggest that breastfeeding mothers experienced a significant increase in nipple pain and soreness at 24, 48, and 72 hours after delivery.
The mean score of nipple soreness in the olive oil group was significantly lower than that in the breast milk group 48 hours after delivery. However, no significant difference emerged between olive oil and breast milk groups in relieving nipple pain and soreness. This study's findings are consistent with those of Pezeshki et al 23 who also reported an insignificant difference between breast milk and olive oil to heal sore nipples.
The findings of this study are inconsistent with some previous studies. An experimental, prospective, and randomized study of 300 lactating women conducted by Cordero et al 17 found a lower rate of nipple cracks in the olive oil group than in the breast milk group when investigating the effectiveness of olive oil versus breast milk in reducing nipple cracks. Another experimental study involving 135 postpartum women conducted by Hables and Mahrous 18 found that olive oil, coconut oil, and breast milk had a positive effect on treating nipple soreness, although the olive oil group reported a greater effect than the coconut oil and breast milk groups.
A randomized controlled trial conducted by Ahmed et al 14 found that the olive oil group had significantly lower nipple pain, lower nipple trauma, and better nipple trauma healing than the breast milk group in 60 Egyptian breastfeeding mothers. Our study yielded different findings partly because we included fewer participants and shorter observations (within 3 days of delivery), which may have affected the results. Although this study found no significant difference between the olive oil and breast milk groups in reducing nipple pain and soreness, the descriptive data indicated that nipple pain and soreness scores were lower at 24, 48, and 72 hours after delivery in the olive oil group than in the breast milk group.
Moreover, participants in this study gave positive feedback on using olive oil during the initial stages of breastfeeding. Olive oil could reduce nipple pain and redness, leading to the feeling that the breasts have enough moisture, and offer an extra layer of protection. This is consistent with Gungor et al.'s 15 study, which indicated that more women chose olive oil over lanolin cream in the first week of breastfeeding and recommended using olive oil to protect nipples from cracking during suckling, especially in early lactation.
In the past, breastfeeding mothers suffering from nipple pain and soreness were instructed to apply lanolin cream or breast milk in Taiwan. To our knowledge, this is the first study that evaluates the effects of olive oil on relieving nipple pain and soreness in breastfeeding mothers in the Chinese context. Olive oil is a natural product with moisturizing and antibacterial properties, and it is an easy-to-obtain and inexpensive product that does not cause skin irritation or adverse side effects. It is beneficial for skin moisturizing, wound healing, and pain relief. 13
Our results demonstrated that olive oil has the same effect as breast milk. The results suggest that health care professionals in clinical practice should offer nursing mothers olive oil care instructions in addition to breast milk in the early breastfeeding period. In addition, the most common cause of nipple pain and soreness is incorrect breastfeeding posture and baby's inappropriate latch-on. 24 Thus, health care professionals are advised to provide breastfeeding-related knowledge and skills, and necessary assistance during the breastfeeding period to help mothers continue breastfeeding.
Limitations
A small sample size, unblinded participants, potential contact between participants, and a single hospital setting may have contributed to selection or performance bias of this study. Therefore, further research trials should take into consideration a larger sample size, a randomized setting, and design that prevents participants from communicating, and a longer follow-up to gain further insights into applying olive oil as a pain-relief method for breastfeeding mothers. Alternatively, researchers may consider implementing different measures on the left and right breasts of the same subject in their study design to increase reliability.
Conclusions
Nipple pain and soreness are concerning for breastfeeding mothers, making it difficult for them to continue with breastfeeding. Health care professionals should provide breastfeeding mothers with effective measures for prevention and treatment of nipple problems during the early postpartum period. Olive oil is a plant-based product with moisturizing and antibacterial properties, easy to obtain, and inexpensive, which can be used to treat nipple pain and soreness among lactating mothers.
Footnotes
Acknowledgments
We are grateful to the participants who gave their time for this study.
Authors' Contributions
C-X.L. conceptualized the topic, conducted research and formal data analyses, and wrote the article's first draft. Y-Y.L. assisted with the conceptualization and critically revised drafts of the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.