
Abstract
Background:
African American women continue to experience low rates of breastfeeding initiation as well as low rates of exclusive breastfeeding for 6 months. Research has indicated that there are several social determinants that impact breastfeeding rates, but there is a dearth of literature that allows African American women to give voice to their experiences. In addition, research has shown women, infant, and children (WIC) participants to have lower breastfeeding rates than non-WIC eligible women.
Research Aim/Question:
The aim of this systematic review was to examine the relationship between WIC program participation and breastfeeding initiation and duration among non-Hispanic African American/Black women.
Methods:
The approach for this review used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Four online databases, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Library, MEDLINE, and SCOPUS, were used to search for peer-reviewed articles and grey literature.
Results:
Two hundred eighteen articles were retrieved through the database search and underwent initial screening, yielding 59 potential eligible articles. Full-text articles were further reviewed and 11 met the inclusion criteria and were included in this systematic review.
Conclusions:
Included studies show mixed results regarding the association between WIC participation and breastfeeding initiation, but there is a general negative association between WIC participation and breastfeeding duration, especially among Black women.
Introduction
The women, infant, and children (WIC) Supplement Nutrition program was established to ensure nutritional adequacy based on the United States Department of Agriculture guidelines. Since its inception, WIC has always provided supplemental foods, nutrition education, and counseling related to healthy food choices and nursing options and has even provided support for breastfeeding. Historically, WIC has served to provide food access for birthing people and children up to age 5, and counseling related to healthy food choices and nursing options and has even provided support for breastfeeding. However, the promotion of breastfeeding has been obscured by many WIC facilities having infant formula readily available. In recent years, there has been a cultural shift within WIC, and this has prompted greater advocacy and support for breastfeeding via peer breastfeeding support groups and the availability of lactation consultants in WIC clinics.
Background
Breastfeeding is an optimal source of nutrition for infant development and growth, and it provides all the energy and nutrient requirements for the first 6 months of an infant's life. 1 Numerous research studies have demonstrated the ability of human milk to confer health benefits. These conferred benefits are inclusive of women and infants and have implications for chronic diseases and mental health. 2 Breastfeeding is associated with reduced risk for certain health conditions, such as SIDS, types 1 and 2 diabetes, and respiratory tract infection for infants, and increase lactational amenorrhea, reduce risk of breast and ovarian cancers for their women, leading to reduced overall health care costs. 3
Due to the positive health impact on the life course of mother and child, the Centers for Disease Control and Prevention (CDC) recommends that women breastfeed their infants exclusively the first 6 months and continue to breastfeed for at least 12 months in combination with complementary foods or for longer as mutually desired by the birthing person and infant. 3
Healthy People 2020 (HP 2020) was launched in 2010 with established goals to improve the nation's health. Healthy People 2030 (HP 2030) launched in 2020 with changes to prioritize the most pressing public health issues. Five breastfeeding objectives in HP 2020 included breastfeeding initiation, breastfeeding duration at 6 months and 1 year, and exclusive breastfeeding through 3 and 6 months. HP 2030 prioritized to only two objectives related to breastfeeding: exclusive breastfeeding at 6 months and breastfeeding duration at 1 year. The target for these objectives was increased in HP 2030, further expanding the breastfeeding disparity among Black birthing people and emphasizing the need to promote breastfeeding among this population.
Despite known benefits of breastfeeding, there is low prevalence in breastfeeding in the United States. Only one in four infants meet the recommendation of 6 months of exclusive breastfeeding. 4 In addition, national breastfeeding rates data have shown that African American/Black infants have the lowest breastfeeding rates compared to other races in the United States. African American/Black birthing people have the lowest rates of breastfeeding initiation and breastfeeding at 6 months. WIC participants also have the lowest breastfeeding rates compared to eligible and ineligible nonparticipants. Low prevalence in breastfeeding can be due to various barriers to breastfeeding. 5
Disparities in breastfeeding rates are associated with a multitude of factors. Lack of ongoing support for breastfeeding and confusion surrounding breastfeeding can become barriers that limit individuals from providing breast milk for their infants. Variation in hospital routines regarding infant formula distribution, practices that discourage exclusive breastfeeding, and lack of breastfeeding support after discharge 3 are also some of the barriers. African American/Black birthing people have reported that some of the barriers to breastfeeding include lack of knowledge about benefits of breastfeeding and lack of family support. 6 In North Carolina, WIC clinics serving areas with higher African American populations are less likely to offer breastfeeding support services. 7
However, WIC's budget has a disproportionately larger allocation toward infant formula than peer counseling and breastfeeding initiatives. 8 These findings contrast with WHO and UNICEF's International Code of Marketing of Breast-milk Substitutes, which states that health workers should encourage breastfeeding and to only use marketing and distribution of breast milk substitutes when necessary to avoid incentivizing women to choose infant formula over breastfeeding.
With the emergence of studies demonstrating various benefits of breastfeeding, there have been many interventions developed to improve breastfeeding rates. Breastfeeding is a learned behavior, which requires active support to sustain breastfeeding practices. 9 Researchers have shown that peer counseling programs to provide breastfeeding support for WIC participants led to higher initiation and duration of breastfeeding. Segura-Pérez et al. reported that different breastfeeding-promoting policies impact U.S. minoritized populations differently. For example, Black birthing people were more likely to initiate breastfeeding in states where there were laws protecting breastfeeding in public and private locations, but are less likely to continue breastfeeding for 6 months in states with laws providing breaks from work and workplace pumping. 10
The WIC program has also implemented interventions to promote breastfeeding among participants. Overall, WIC has made some progress in their primary aim of safeguarding the health of recipients, despite having lower breastfeeding rates in comparison to nonrecipients. WIC aims to reduce the breastfeeding disparity by providing education, support, and incentives for eligible women to improve breastfeeding rates for infants of low socioeconomic status households. WIC implemented a food package revision in 2009 to promote breastfeeding by raising food benefits for individuals exclusively breastfeeding and reducing formula provisions for those partially breastfeeding. 11 The 2009 food package revision and the WIC breastfeeding peer counseling program have shown to improve participant breastfeeding rates.
Although the WIC program has increased breastfeeding rates among WIC participants over the years, the 2018 NIS showed that the increased rates were not enough to reach HP 2020 targets or to reduce the difference between breastfeeding rates of WIC participants and nonparticipants. According to the NIS data, from 2011 to 2018, both WIC participants and nonparticipants improved in breastfeeding outcomes, but only the gap in breastfeeding initiation reduced between WIC participants and eligible nonparticipants (11.6% difference reduced to 6.4% difference), the difference in breastfeeding duration and exclusivity slightly decreased (duration at 6 months and exclusivity at 3 months) or slightly increased (duration at 12 months and exclusivity at 6 months).5,12,13
In relationship to HP 2020, non-Hispanic Black is the only racial/ethnic group that did not reach the target for breastfeeding initiation. Across all breastfeeding goals of HP 2020, non-Hispanic Black infants consistently had the lowest rates compared to all other racial and ethnic groups. Non-Hispanic Black infants also did not reach any breastfeeding goal of HP 2020. One possible factor for this discrepancy is the infant formula rebates system available to WIC participants, providing a perceived low-cost formula package to WIC participants while driving up formula costs which would deter WIC nonparticipants from using formula, further increasing the breastfeeding disparities. 14 Although Murimi found that many of their WIC participants (88%) reported that the availability of free formula by WIC did not affect their breastfeeding decision, the participants reported that the additional breastfeeding food package also did not affect their decision to breastfeed (59%). 6
However, 41% of participants were not aware of the additional food package and 49% were not aware of the availability of breast pump assistance, which would have assisted with breast milk feeding, further highlighting the need for WIC to emphasize breastfeeding benefits, increase awareness of breastfeeding incentives, and potentially revise incentives to breastfeeding.
The aim of this systematic review was to assess the association between WIC program participation and breastfeeding initiation and duration among non-Hispanic African American/Black women. The secondary objectives of this review were to assess whether WIC-provided infant formula and WIC income eligibility or socioeconomic status influenced breastfeeding rates among these women.
Methods
Inclusion and exclusion criteria
The systematic review used Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) for systematic review protocol and the Institute of Medicine's published Finding What Works in Health Care: Standards for Systematic Reviews. All types of study designs and manners of publication were included for this review, including grey literature from references cited in the articles. The studies included are exclusively published full text in English and within the last 10 years (2010–2020) to coincide with the launch of HP 2020.
The participants of the studies included non-Hispanic African American/Black WIC-eligible women older than 18 years of age who have given birth. The intervention of interest was the target population's participation with WIC. The comparison group included the target population who are not WIC participants.
The primary outcome was the change of breastfeeding initiation and duration due to WIC participation. The secondary outcomes were the change of breastfeeding rates due to access to WIC-provided infant formula or income status related to WIC-eligibility.
Search approach
Four online databases, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Library, MEDLINE, and SCOPUS, were used to search for peer-reviewed articles and grey literature. An experienced Health Science Librarian created a search string and translated the string to fit the selected databases, then followed the PRISMA diagram for inclusion and exclusion of articles. Search terms included “breast feeding,” “infant formula,” “WIC participants,” “African Americans,” and “non-Hispanic Black.”
For retrieved eligible studies, their abstracts, titles, and index terms used to describe the articles were reviewed by two independent reviewers for relevance based on the inclusion criteria and research question. Articles not able to sufficiently address the research question were removed. The remaining articles were reviewed for inclusion in the systematic review by six individual reviewers. Consensus was achieved by discussion among reviewers for final inclusion of articles in the systematic review.
Data extraction
Data were extracted for the study details, including study design, sample size, evidence level, participant characteristics race/ethnicity, WIC participation, breastfeeding outcomes, socioeconomic status, and formula feeding if applicable.
Results
Search results
Figure 1 shows the PRISMA flow diagram that depicts the search and inclusion of studies. The search string identified 218 articles which underwent initial screening and 59 were potentially eligible based on the abstracts. These full-text articles were further reviewed and 11 met the inclusion criteria and were included in this systematic review (Table 1 shows the articles included in the systematic review). Two studies reported breastfeeding initiation outcomes, five studies reported breastfeeding duration outcomes, and four studies reported both outcomes. Two studies used human milk feeding at neonatal intensive care unit (NICU) discharge as the outcome, which is assumed to be equivalent to breastfeeding duration due to the average length of NICU stay (73.0 ± 35.0 days). Fleurant et al. and Riley et al. used samples from the same population with slight differences in exclusion criteria. Shim et al., Sparks, and Sparks obtained their samples from the same data set.16,22,23,25,26
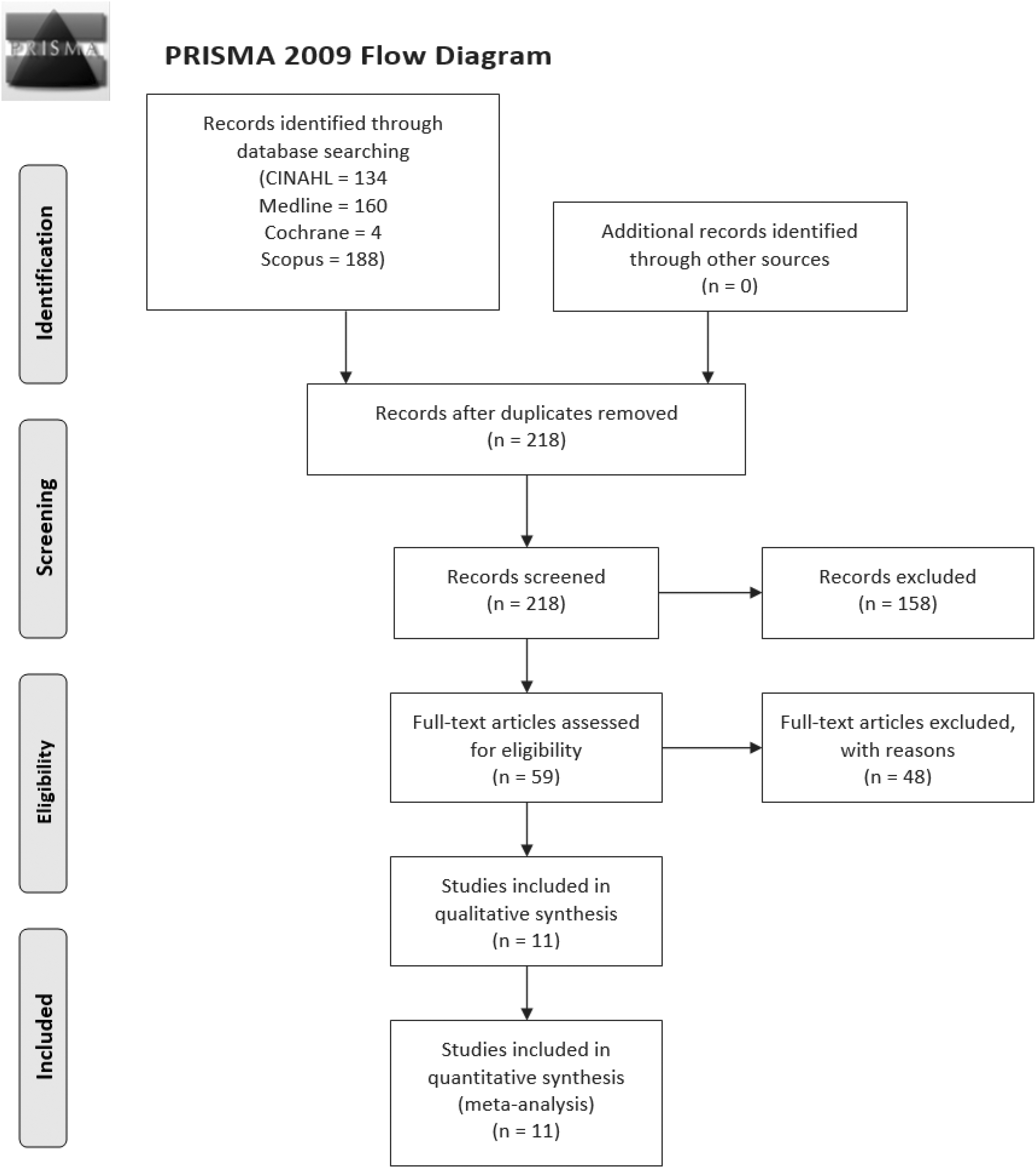
PRISMA 15 flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Articles Included in Systematic Review
BF, breastfeeding; HM, human milk; NICU, neonatal intensive care unit; WIC, women, infant, and children.
Breastfeeding initiation
Table 2 summarizes the articles which provided evidence for initiating breastfeeding. Six total studies reported breastfeeding initiation outcome(s). One study found that WIC participation is associated with higher breastfeeding initiation for Black women, but not White women, while three studies found that WIC participation is associated with lower breastfeeding initiation regardless of race or ethnicity.18,19,21,24 Marshall et al. found no significant association between WIC participation and breastfeeding initiation among Black women. 20 Black birthing people are shown to have the lowest rate of breastfeeding initiation in all the studies. One study measured formula feeding at the hospital and found higher rates of usage among Black women. 21
Summary of Evidence Regarding Breastfeeding Initiation Among Non-Hispanic African American/Black Women Stratified by Women, Infant, and Children Participation
CI, confidence interval; OR, odds ratio; NHB, Non-Hispanic Black; WIC, women, infant, and children.
Breastfeeding duration
Nine total studies reported breastfeeding duration outcome. Table 3 shows the summarized results of these studies. One study found that Black women make up a higher percentage of WIC participants who entered with low-intensity breastfeeding (breastfeeding <60% of total liquid feeds), which is the group with the shortest breastfeeding duration. 17 Five studies found that WIC participants have the shortest breastfeeding duration.16,18,22,23,26 Three studies found that WIC participation was not associated with breastfeeding duration among Black women.17,19,20 Six studies found that Black women have the shortest breastfeeding duration.16,18,19,21,22,26
Summary of Evidence Regarding Breastfeeding Duration Among Non-Hispanic African American/Black Women Stratified by Women, Infant, and Children Participation
BF, breastfeeding; CI, confidence interval; FPL, federal poverty level; HM, human milk; OR, odds ratio; NHB, Non-Hispanic Black; NICU, neonatal intensive care unit; SD, standard deviation; WIC, women, infant, and children.
WIC participation
Seven studies found higher WIC eligibility and participation among Black women, and one study found fewer Black women among nonparticipants compared to White women. One study 18 found that WIC participation had a negative influence on breastfeeding duration among all regions of the United States. One study 17 found that participants entering WIC while having high breastfeeding frequency were more like WIC nonparticipants than participants who entered WIC while having low breastfeeding frequency. Another study 20 found that WIC participation during pregnancy was not associated with breastfeeding initiation among Black women, but was negatively associated with breastfeeding initiation among White women.
Healthy People 2020
HP 2020 set goals for breastfeeding initiation and breastfeeding duration at 6 months, which correspond to the two breastfeeding outcomes assessed by this literature review. The target for ever breastfeeding is 81.9% and the target for breastfeeding duration at 6 months is 60.6%. The most recent data (2015) for non-Hispanic Black children were 69.4% ever breastfed and 44.7% breastfed at 6 months, both of which did not reach the target.
The HP 2020 target for ever breastfeeding is 81.9%. Out of the seven studies reporting breastfeeding initiation outcome data, all seven studies consistently showed that non-Hispanic Black women had the lowest breastfeeding initiation, regardless of WIC participation, compared to women of other race and ethnicities and consistently did not reach the HP 2020 target for breastfeeding.
The HP 2020 target for breastfeeding duration at 6 months is 60.6%. However, studies do not have consistent measurements for breastfeeding duration. Two studies measured continued human milk feeding at NICU discharge, some studies measured rate of short breastfeeding duration, one study reported rate of breastfeeding at 10 weeks, and others reported the mean duration of breastfeeding.16,20,22 Sparks reported rate of breastfeeding duration at 6 months and showed that breastfeeding duration among non-Hispanic Black women were the lowest, regardless of WIC participation, and did not reach the HP 2020 target (5.88% and 9.98%, respectively). 26 Out of the nine studies reporting breastfeeding duration outcome data, seven had data to show that breastfeeding duration was consistently the shortest among Black women compared to women of other race and ethnicities, and three studies showed that WIC participation is associated with lower breastfeeding duration.
Gregory et al. found that WIC entry when breastfeeding was already low and was associated with the lowest breastfeeding duration, but did not link this outcome to maternal race or ethnicity. 17 Marshall et al. showed the probability of breastfeeding at 10 weeks and found that Black women are less likely to breastfeed at 10 weeks compared to White women, but Black women's probability of continuing breastfeeding did not differ with WIC participation. 20
Discussion
Breastfeeding initiation
Jensen analyzed state data and regional data, dividing the country into seven regions (Northeast, Mid-Atlantic, Southeast, Midwest, Southwest, Mountain plains, Western). Jensen's results found that non-Hispanic Black women had the lowest breastfeeding initiation rate and are more likely to be WIC participants than eligible nonparticipants. 18 The study's adjusted model found that the odds of breastfeeding for WIC participants were significantly lower than that of eligible nonparticipants. Three of the seven regions across the United States analyzed by Jensen indicated a significant negative association between WIC participation and breastfeeding initiation, whereas the other four regions had negative associations and they were not statistically significant. However, Jensen's article used data from 2007, before the WIC food package revision in 2009 that have been demonstrated to decrease breastfeeding initiation disparities among WIC participants.
Marshall et al. found that Black women are more likely than White women to be WIC participants and are more likely to use Medicaid, even among nonparticipants. 20 Despite Black women having lower breastfeeding initiation overall compared to White women, their adjusted regression models found no significant decrease in breastfeeding initiation between Black WIC participants and Black nonparticipants. One potential reason for this finding is because Black women already have overall low breastfeeding rates coupled with high rates of WIC participation among Black women.
However, Marshall et al. only analyzed data in Mississippi from 2004 to 2008, before the WIC food package revision. Their finding related to Black women is supported by Jensen's adjusted model that found most states, including Mississippi, had no association between WIC participation and rates of breastfeeding initiation compared to nonparticipants. 18 However, Marshall et al. found that WIC participation is associated with lower breastfeeding initiation among White women, citing potential WIC contributions such as food package content, education and counseling, support, and formula supplementation. 20
Sparks' results found that non-Hispanic Black women not only had the lowest breastfeeding initiation rates compared to women of other races and ethnicities in both urban and rural settings, but they also had the highest rate of family living below the poverty threshold and the lowest rate of being married. 25 In their logistic regression model, living below the poverty threshold is consistently shown to have lower odds of breastfeeding initiation, and non-Hispanic Black women, especially those living in rural settings, had the lowest odds of breastfeeding initiation compared to women of other races and ethnicities. On the contrary, rural women of other races and ethnicities have higher odds of breastfeeding initiation. The model also showed that non-Hispanic Black women participating in WIC had slightly higher odds of initiating breastfeeding (odds ratio = 1.13), but this effect is not statistically significant and is lower than most women of other races and ethnicities.
Sparks discussed that rural non-Hispanic Black women had significantly lower odds of initiating breastfeeding than urban non-Hispanic Black women and noted the differences between the groups. The majority of rural non-Hispanic Black women used WIC, lived in poverty, and were least likely to be married. In addition, both rural and urban non-Hispanic Black women were more likely to work during pregnancy. Sparks concluded that factors such as lack of marital partner support, poor economic circumstances, WIC formula, and employment barriers may explain lower breastfeeding initiation rates among rural non-Hispanic Black women. However, WIC usage is only assessed by Sparks based on whether the mother or infant received benefits from WIC without specification about formula usage. WIC participation can impact breastfeeding outcomes due to lack of breastfeeding support or education, not just from infant formula access. In addition, the data used were from 2001, before the WIC food package revision.
Sonchak found that Black WIC participant women were more likely to breastfeed (41%) compared to Black nonparticipant women (39%). 24 However, Sonchak stated that the Black WIC women were less likely to be high school dropouts (28% versus 31%) and more likely to have some college education (32% versus 29%) compared to the Black nonparticipant women. This is in contrast with Marshall et al.'s 20 sample in which Black WIC women are more likely to be high school dropouts (31.5% versus 20.6%) and less likely to have some college education (33.5% versus 53.0%) compared to Black nonparticipant women. The other included studies show that WIC participants are more likely to have less education than nonparticipants, but the data were not stratified by both WIC participation and Black women, so there may be different patterns of education based on different maternal races and ethnicities.
While Sonchak controlled for socioeconomic status by including only Medicaid insurance users, they also only focused on women with multiple births, so their findings may not be generalizable to women with a singular birth. Regardless, Sonchak's sample size is the largest of the 11 included articles and includes the most recent data in 2013, likely having more data after the WIC food package revision that may explain the different results.
Ma et al.'s 19 results found that not only are Black women more likely to be WIC participants, but also WIC participants who still had significantly lower breastfeeding initiation rates (55.5%) despite more participants receiving breastfeeding information through WIC (91.6%) compared to both eligible and ineligible nonparticipants. In the adjusted regression models, both ineligible and eligible nonparticipants had significantly higher odds of breastfeeding compared to WIC participants, and women of other races and ethnicities have significantly higher odds of breastfeeding compared to non-Hispanic Black women. Ma et al. discussed that providing breastfeeding information is a good approach to encourage breastfeeding among WIC participants, but breastfeeding education was already on a desirable level (overall 84.9%). The regression model showed that women receiving breastfeeding information had an insignificantly lower odds of breastfeeding. Ma et al.'s sample were taken from 2009 to 2010, which would include women receiving the revised WIC food package.
However, the study found that breastfeeding initiation disparity remained large between WIC participants and nonparticipants. In addition, receiving breastfeeding information did not significantly improve breastfeeding outcomes. There may be other factors that still function as barriers to breastfeeding among WIC participants independent of breastfeeding education, so future WIC interventions should be addressing other barriers to promote breastfeeding.
McKinney et al. results found that breastfeeding initiation was lowest among Black women and analyzed various mediators that may contribute to disparities between racial and ethnic groups. 21 In relationship to the breastfeeding initiation disparities between Black and White women, Black women had higher rates of poverty and lower rates of having a college degree or being married, all of which fully mediated the difference in breastfeeding initiation. Second, in relationship to the breastfeeding initiation disparities between non-Hispanic Black and Spanish-speaking Hispanic women as well as English-speaking Hispanic women, Black women were less likely to have been breastfed, which would have predicted greater breastfeeding initiation in the next generation. Breastfeeding practices and perceptions are often culturally mediated, and differences have been shown between not only Hispanic and non-Hispanic Black women but between non-U.S. born Black women.
Overall, the study showed that Black women had higher rates of poverty, lower levels of education and marriage, which predicted lower breastfeeding initiation. McKinney et al. indicated that all these characteristics contribute to the social environment and self-efficacy, which are key factors for improving breastfeeding. 21 These may be factors that breastfeeding promotion interventions should target to mitigate disparities experienced by Black women.
Three of the articles evaluating breastfeeding initiation using data before 2009 had mixed results regarding the association between WIC participation and breastfeeding initiation.18,20,25 Three articles that included data after 2009 still showed mixed results regarding the association between WIC participation and breastfeeding initiation.19,21,24 The WIC 2009 food package revision did not appear to reduce the disparities in breastfeeding initiation, especially among Black women. The mixed results between the articles relates to differences in research methodologies, but also point to an unstudied variable within the models.
Breastfeeding duration
Fleurant et al. concluded that WIC eligibility negatively predicting human milk feeding at NICU discharge (average 73 days length of NICU stay) may reflect economic status rather than lack of WIC lactation support. 16 Their finding is due to the article only determining whether participants are WIC eligible or ineligible, not whether they participated in WIC or not, as nonparticipants may either be eligible or ineligible due to income.
In addition, the article found that neither breastfeeding support nor lack thereof from friends, family, and peers were correlated with human milk feeding at discharge. This contrasts with other studies that show support from friends, family, and community can facilitate breastfeeding and lack of support can become a barrier to breastfeeding. For example, Gyamfi et al. described the cultural dimension that influences breastfeeding experiences of African American women in the United States, stating that breastfeeding support or lack thereof from family, peers, and the community significantly impacts breastfeeding outcomes. 27 The difference in correlation may be due to different settings inside the hospital versus community setting or home setting.
Jensen found that the difference in breastfeeding duration is seen based on regions of the United States, with WIC participants in western regions having a smaller decrease in breastfeeding duration compared to nonparticipants, and WIC participants in eastern regions having a larger decrease in breastfeeding duration compared to nonparticipants. 18 Factors may differ based on regional differences, so WIC may improve breastfeeding disparities by addressing region-specific factors that contribute to breastfeeding differences.
Marshall et al. was one of the three articles that found no association between WIC participation and breastfeeding duration among Black women. 20 However, this article did not stratify the data among nonparticipants based on eligibility criteria. Furthermore, the breastfeeding duration outcome measured only whether women breastfed at 10 weeks or not, which is much shorter than the mean breastfeeding duration of 6 months among Black women in Jensen's article, so the study would not be able to capture the potential differences in breastfeeding duration between WIC participants and nonparticipants.
McKinney et al. results showed that Black women had shorter breastfeeding duration than White women, and Black women are significantly more likely to experience in-hospital formula introduction, which was the biggest predictor of breastfeeding duration. 21 Studies have indicated that Black birthing people are more likely to be introduced to and provided formula than other racial groups. 28 Racial bias that has been cited has an explanation for this discrepancy in formula introduction while in the hospital. 28 On one hand, Black women's lower likelihood of having a college degree or being married predicted shorter breastfeeding duration, but on the other hand, Black women's higher rates of poverty was not a unique predictor of breastfeeding duration. Compared to Spanish-speaking Hispanic women, Black women were less likely to have a family history of breastfeeding and less likely to live with the infant's father, both of which partially predicted lower breastfeeding duration among Black women.
The sociocultural factors of marital status, family, structure, education, income, and neighborhood characteristics are complex interacting with race, which imposes social and historical barriers to breastfeeding for Black women. 29 DeVane-Johnson et al. discusses the legacy of slavery and Jim Crow and the deleterious impacts on breastfeeding practices of Black women. 30 McKinney et al.'s study highlights the factors independent of WIC-participation that may contribute to breastfeeding disparities experienced by Black women. Riley et al.'s findings may explain the mixed findings regarding the association between WIC participation and breastfeeding outcomes, especially in relationship to socioeconomic status that indicates eligibility for WIC. 22 The article found that both WIC eligibility and maternal race negatively predicted human milk feeding at discharge. The results demonstrate the need for further exploration into the impact of race and racisms impact on breastfeeding, particularly examine the intersection between these two variables.
In addition, socioeconomic status affected breastfeeding outcomes of all race and ethnic groups, but disproportionately affected Black women to a greater degree. The disparity in socioeconomic and racial status may partially explain why other studies have found no association with WIC participation on breastfeeding outcomes. However, Riley et al.'s article also only included WIC eligibility, not whether the women were WIC participants or not.
Shim et al. results showed that WIC participants are more likely to have short breastfeeding duration (<6 months) compared to nonparticipants. 23 The study categorized the data by childcare and found that infants receiving parental care were less likely to have short breastfeeding duration than infants who received nonparental (relative or center-based) care. Nonparental care is a proxy for work status, with parents relying on childcare being more likely to be employed outside of the home. Return to work and working conditions have been cited as a barrier to breastfeeding by Black women, particularly for women employed in nonmanagerial roles. 30 Therefore, both WIC participation and childcare are risk factors for breastfeeding duration, and future studies should include childcare setting in addition to maternity and breastfeeding policies in the workplace as variables when evaluating breastfeeding outcomes.
The effects were found after adjusting for confounding factors between WIC participants and nonparticipants, which includes higher proportion of White infants, married women, women having some college education, and women having incomes higher than 185% of the poverty threshold among nonparticipants. However, the sample used in this study was from 2001, more than two decades old. In addition, this study included women who did not initiate breastfeeding among those with short breastfeeding duration. Furthermore, the study did not specify WIC eligibility among nonparticipants. To evaluate whether breastfeeding duration may be due to WIC participation or socioeconomic status related to income requirements for WIC eligibility, it is beneficial for studies to discern nonparticipation of WIC between income-eligible and income-ineligible women.
Gregory et al. results support Fleurant et al. conclusion, as their results show that breastfeeding duration is higher (37 weeks) among women who entered WIC while frequently breastfeeding than eligible nonparticipant women (33 weeks), potentially indicating successful WIC lactation support for certain women participating in WIC. Meanwhile, women who entered WIC while infrequently breastfeeding had the shortest breastfeeding duration (8 weeks). 17 The finding highlights differences within WIC participants, and identifying factors contributing to these differences would be potential targets for future interventions to reduce breastfeeding disparities.
Ma et al. compared breastfeeding duration between WIC participants, eligible nonparticipants, and ineligible nonparticipants and found that the shortest breastfeeding duration was among participants (7 weeks) and the highest duration was among ineligible nonparticipants (11 weeks). 19 The unadjusted association between breastfeeding duration and WIC participation is significant, but became insignificant after adjusting for covariates, indicating that differences in breastfeeding duration may be due to other factors independent of WIC participation. One of the covariates was maternal race. However, this article determined WIC eligibility based on Medicaid use, which is shown in Marshall et al., results that even WIC participants may be using private insurance.
Sparks' study only included women who were WIC-eligible and found that non-Hispanic Black women were the least likely to breastfeed for 6 months compared to women of other races and ethnicities. 26 Black women had the highest rate of WIC participation and were most likely to be single, which highlight the potential lack of support from the infant's father and the importance for WIC program to address the breastfeeding disparity among their participants. Moreover, the study's analysis found that WIC participants were more likely to discontinue breastfeeding. However, this study was published one decade ago, using data from almost one decade before publication.
Of the included articles, none found a positive association between WIC participation and breastfeeding duration. Instead, three articles found no association and six articles found a negative association between WIC participation and breastfeeding duration. Among studies using data before 2009, two found no association and three found a negative association.16–18,20,21,23 Among studies including data after 2009, one found no association and three found a negative association.17,19,22,26 The WIC 2009 food package revision did not appear to reduce disparities in breastfeeding duration, which is supported by Li et al. study. 11
WIC provided infant formula
Although both Marshall et al. and Sparks discussed infant formula access through WIC may be factors that lower breastfeeding initiation among WIC participants, only McKinney et al. study evaluated formula use in their methods and that variable referred to in-hospital formula use, which is not specific to WIC-provided infant formula. There is a gap in knowledge in evaluating use of infant formula provided by WIC to participants.20,21,25
Socioeconomic status
Studies assessing socioeconomic status evaluated either type of health insurance or income relative to poverty threshold. Marshall et al. found that Black women are more likely to have Medicaid than private insurance compared to White women. 20 Riley et al. found that socioeconomic status disproportionately affected breastfeeding rates of Black women to a greater degree than White or Hispanic women. 22 Sparks found that Black women were more likely to work during their pregnancies and had the highest rate of living below the poverty threshold, which is a factor that lowers odds of breastfeeding initiation. 25 McKinney et al. found that Black women had higher rates of poverty, which mediated differences in breastfeeding initiation compared to White women, but did not predict short breastfeeding duration. 21 Overall, low socioeconomic status is associated with poorer breastfeeding outcomes, especially among Black women, which demonstrates the intersection of race and its influence on breastfeeding outcomes.
Education
Education has been evaluated by several studies and may be a contributing factor to differences between women. Sonchak and Marshall et al. found conflicting results regarding the likelihood of being high school dropouts or having some college education among Black WIC participant women.20,24 McKinney et al. found that Black women were less likely to have a college degree, which is a variable that predicted short breastfeeding duration and mediated the difference in breastfeeding initiation rates compared to White women. 21 Riley et al. found that Black women were more likely to graduate high school and have some college, but less likely to complete 4 years of college. 22 Jensen found that women with increasing educational levels had higher breastfeeding initiation and longer breastfeeding duration. 18 Overall, other studies that stratified data by WIC participation showed that education was generally lower among participants than nonparticipants.
Marriage status
Marriage status may indicate presence of breastfeeding support from the partner. Sparks found that Black women had the lowest rate of being married compared to other women, which may or may not contribute to differences in breastfeeding outcomes. 25 Marshall et al. found that while Black WIC participants had lower rates of being married than nonparticipants, overall, Black women had lower rates of being married compared to White women. 20 However, McKinney et al. found that Black women were less likely to be married, which predicted short breastfeeding duration and mediated differences in breastfeeding initiation compared to White women. 21 Gregory et al. found that women who entered WIC while breastfeeding less frequently had significantly lower rates of marriage than women who entered WIC while breastfeeding more frequently. 17
Studies that stratified data by WIC participation showed that marriage rates were generally lower among participants than nonparticipants. Jensen found that women who were married were more likely to initiate breastfeeding and continue breastfeeding for longer than women who were not married. 18
Limitations
One of the aims of this study was to assess available data regarding the use of WIC-provided infant formula among WIC participants and how that is associated with breastfeeding initiation and duration. However, none of the included studies evaluated the use of WIC-provided infant formula among WIC participants. Future research evaluating the association between WIC participation and breastfeeding outcomes should collect data regarding WIC-provided infant formula use, socioeconomic status, and breastfeeding education and support. In addition, studies do not disaggregate data for Black/African Americans or Hispanic populations, nor do studies discuss differences between U.S. born and non-U.S. born populations and exposure to breastfeeding practices which are normalized within the culture.
The number of articles available to address the research question was limited, as only 11 articles were included. Many of the eligible articles that were excluded were due to lack of WIC nonparticipant subjects and not addressing or stratifying data by WIC participation or race/ethnicity that includes non-Hispanic Black. The included studies had variations in measurement of breastfeeding outcomes. For example, some studies measured breastfeeding at discharge or short breastfeeding duration (<6 months) instead of breastfeeding initiation or breastfeeding duration. Some studies had relatively low sample size of Black women compared to the entire sample. Although one inclusion criteria for the articles search included studies being published within the past 10 years from 2020, most of the data used by the articles were up to two decades old and may not reflect current trends in breastfeeding outcomes.
Many of the studies used data collected before 2009, due to the availability of data, when WIC revised their food package to promote breastfeeding, so these data are not likely to reflect current breastfeeding outcomes.
Many studies stratified data based on WIC participation for the entire sample but did not stratify by both race or ethnicity and WIC participation. Of the studies that stratified the data by both race or ethnicity and WIC participation, they only specified the percentage of each race or ethnicity within the WIC participation category, and the breastfeeding outcome was an aggregate for the entire WIC participation category. Only two of the included studies stratified breastfeeding data by both race/ethnicity and WIC participation. However, some of the other studies adjusted for covariates which included WIC participation. Future research should stratify breastfeeding data by both variables to illustrate the association of both race/ethnicity and WIC participation on breastfeeding outcomes as well as distinguish between eligible and ineligible WIC nonparticipants.
Conclusions
Included studies show mixed results regarding the association between WIC participation and breastfeeding initiation, but there is a general negative association between WIC participation and breastfeeding duration, especially among Black women. Other noteworthy factors that may contribute to low breastfeeding outcomes among Black women include regional differences, socioeconomic status, marriage status, and educational level.
Footnotes
Authors' Contributions
F.A.K-K. made substantial contributions to the conception/design of the work; the acquisition, analysis, or interpretation of data for the work; drafted the work and revised it critically for important intellectual content; gave the final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
S.T. made substantial contributions to the conception/design of the work, the acquisition, analysis, or interpretation of data for the work; drafted the work and revised it critically for important intellectual content; gave the final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
D.O. made substantial contributions to the acquisition of data for the work and conception/design of the work; drafted the work and revised it critically for important intellectual content; gave the final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
L.W. contributed to the acquisition, analysis, or interpretation of data for the work; revised it critically for important intellectual content; gave the final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
N.M. contributed to the acquisition, analysis, or interpretation of data for the work; revised it critically for important intellectual content; gave the final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
M.S.-S. contributed to the acquisition, analysis, or interpretation of data for the work; revised it critically for important intellectual content; gave the final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
M.P. contributed to the acquisition, analysis, or interpretation of data for the work; revised it critically for important intellectual content; gave the final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work were appropriately investigated and resolved.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.