
Abstract
Introduction:
Although safety data demonstrated the efficacy and effectiveness of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccination for all individuals over 6 months of age, including pregnant and breastfeeding individuals, optimal treatment courses for symptomatic pregnant and lactating individuals infected with SARS-CoV-2 remain to be defined.
Case Description:
A coronavirus disease 2019 (COVID-19)-vaccinated breastfeeding woman received anti-SARS-CoV-2 monoclonal antibody treatment casirivimab–imdevimab 5 days after diagnosis of a symptomatic breakthrough SARS-CoV-2 infection.
Results and Conclusions:
The patient did not present with obvious defects in innate or adaptive cellular subsets, but compared with controls had minimal maternal antibody response to recommended pregnancy vaccinations including SARS-CoV-2 and tetanus, diphtheria, pertussis (TDaP). The outcome of the monoclonal antibody infusion treatment was favorable as it transiently increased SARS-CoV-2 antibody titers in plasma and human milk compartments.
Introduction
The severe acute respiratory syndrome coronavirus 2 (
As of 2023, there are now substantial safety data demonstrating the efficacy and effectiveness of SARS-CoV-2 vaccination for all individuals over 6 months of age, including individuals planning to conceive, pregnant, or breastfeeding.3–6 Unfortunately, a dearth of information remains for the optimal treatment course for symptomatic pregnant and lactating individuals infected with SARS-CoV-2, as well as the role of novel treatments including monoclonal antibodies.7–9
In this scientific report, we describe the case of a breastfeeding woman who received monoclonal antibody treatment casirivimab–imdevimab for a symptomatic breakthrough SARS-CoV-2 infection despite completing the recommended SARS-CoV-2 primary two-dose vaccination series. Compared with controls, we observed minimal maternal antibody response to recommended pregnancy vaccinations including SARS-CoV-2 and tetanus, diphtheria, pertussis (TDaP). The SARS-CoV-2 casirivimab–imdevimab monoclonal antibody (mAb) therapy transiently increased SARS-CoV-2 antibody titers in plasma and human milk.
Materials and Methods
Ethical statement and cohort information
This participant was part of a prospective cohort study approved by the institutional review boards of Oregon Health and Science University and the University of Kentucky. All participants provided written consent before enrollment that occurred from March 2021 to June 2022. Participants who had received SARS-CoV-2 vaccination while either pregnant or breastfeeding within the first postpartum year were identified and invited to participate in the study. In total, 121 SARS-CoV-2-vaccinated (Pfizer BN162b2 or Moderna mRNA-1273) pregnant or lactating participants were enrolled and underwent longitudinal maternal blood and human milk sample collection. Characteristics of the full cohort have been described previously. 10
Sample processing
Whole blood samples were collected and complete blood counts (CBCs) were determined before samples were separated into plasma and peripheral blood mononuclear cells (PBMCs) as described 11 and that were cryopreserved at −80°C and in liquid nitrogen, respectively. Human milk samples were diluted 1:1 in Hanks' Balanced Salt Solution before centrifugation to remove the fat layer before the supernatant was collected and stored at −80°C.
Antibody responses
An indirect ELISA was used to determine the IgG end-point titer (EPT) of antibodies against the receptor-binding domain (RBD) of the SARS-CoV-2 spike protein as previously described 11 or against the tetanus toxoid. Plates were coated with 0.5 μg/mL SARS-CoV-2 spike-protein RBD or 1 μg/mL of tetanus toxoid. Plasma samples were tested in duplicate in a threefold dilution series with an initial 1:30 dilution in blocking buffer. Human milk supernatant was assessed in duplicate at a 4:1 dilution in blocking buffer. Plasma EPT was calculated using log-log transformation of the linear portion of the curve, and 0.1 optical density (OD) units as cutoff. Antibody levels in milk are reported as OD values.
Cellular responses
PBMCs were surface stained with an innate or adaptive antibody panel (500,000 cells per condition) in fluorescence-activated cell sorting buffer (1 × PBS, 2% PBS, 1 mM EDTA). Innate cell populations were determined with CD3, CD20, CC14, HLA-DR, CD16, and CD56 antibodies. Adaptive cell populations were determined with CD4, CD8β, CCR7, CD45RA, and CD20 antibody staining. Samples were incubated for 30 minutes at 4°C for surface staining before being washed in FACS buffer and acquired on the Attune NxT Flow Cytometer.
To measure cellular responses to stimulation, 106 PBMCs were stimulated for 16 hours with a bacterial toll-like receptor (TLR) ligand cocktail containing 1 μg/mL lipopolysaccharide, 2 μg/mL Pam3CSK4, and 1 μg/mL FSL-1. After stimulation, cells were washed and surface stained with CD3, CD20, CD14, and HLA-DR. Cells were then fixed, permeabilized, and intracellularly stained with interleukin (IL)-6 and tumor necrosis factor-α (TNF-α) and were run on the Attune NxT flow cytometer.
Results
Our case participant was a 29-year-old primiparous vaccinated breastfeeding woman who experienced symptomatic SARS-CoV-2 infection 9 months postpartum at 216 days after her initial Pfizer BN162b2 vaccination. Her pregnancy course had been uncomplicated, including receiving TDaP at 31 weeks gestation and undergoing a normal spontaneous vaginal delivery at 39 weeks gestation. She was exclusively breastfeeding, and her infant remained healthy. Per study protocol, maternal blood and milk samples were collected at 60 days postfirst vaccination (DPV) and every 3 months for the first year postpartum (Fig. 1A).
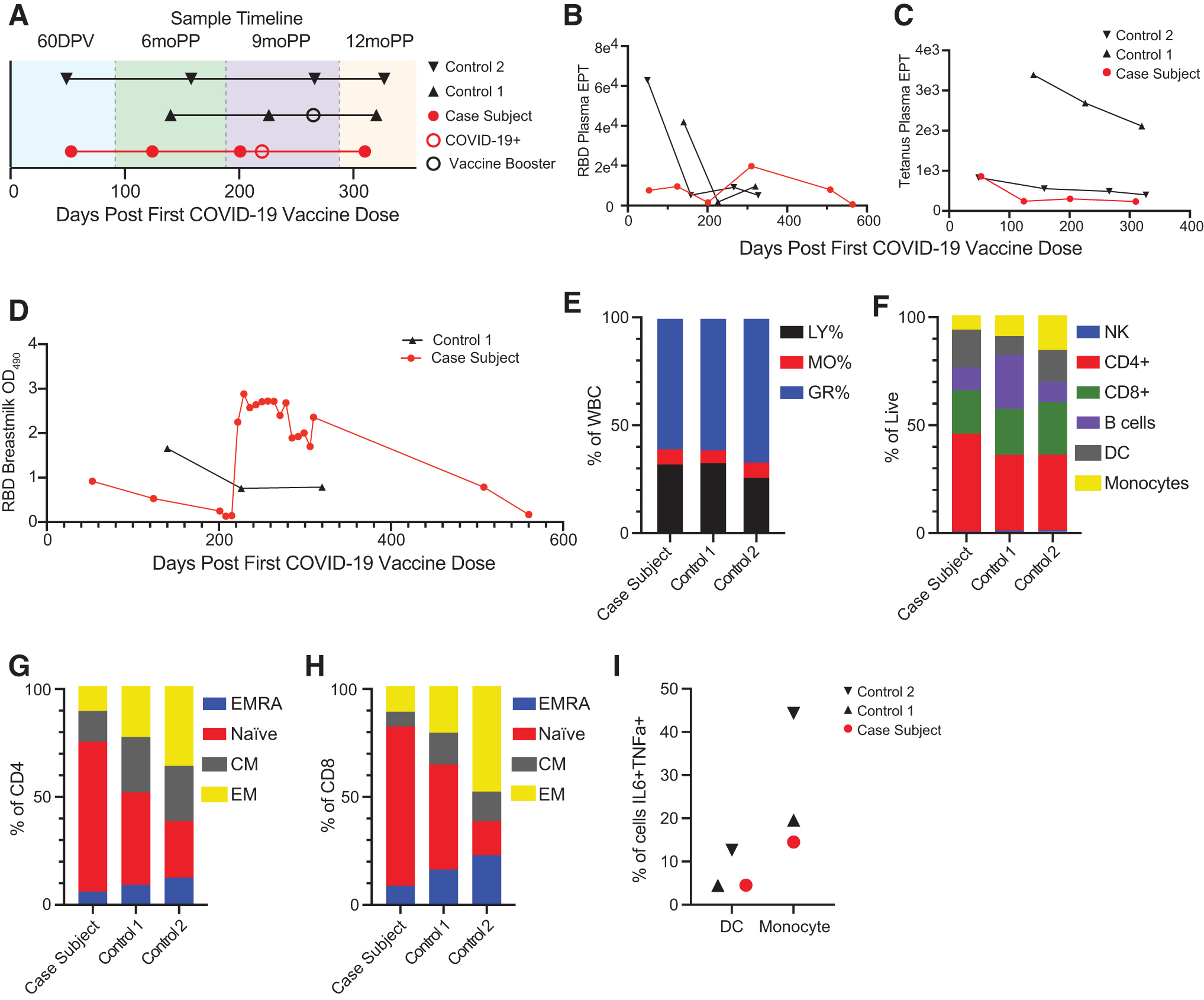
COVID-19 mAb therapy increases SARS-CoV-2 antibody titers in plasma and human milk of breastfeeding woman with breakthrough infection.
The case participant had presented for her routine 9-month study visit at 201 DPV, and tested positive for SARS-CoV-2 infection 15 days later on 216 DPV. She started treatment 5 days postdiagnosis on DPV 222 with casirivimab–imdevimab 600–600 mg/10 mL monoclonal antibody infusion. After infection, milk samples were collected on DPV 220 and 221, and weekly thereafter for 3 months. For the purpose of this report, two matched controls (1 and 2) were identified from the study cohort population.
Evolution of plasma antibody titers specific for SARS-CoV-2 RBD was followed longitudinally and revealed that the case participant had minimal EPTs from 60 DPV up until 2 weeks before SARS-CoV-2 infection, unlike the control participants who had higher initial RBD antibody titers after vaccination that subsequently waned over time (Fig. 1B). RBD EPTs increased significnalty after mAb therapy (310 DPV) compared with the initial vaccine series. However, two additional timepoints collected at 18 and 21 months postpartum showed a continuous decline in maternal RBD antibody levels.
To decipher whether the impaired response in the case participant was specific to the coronavirus disease 2019 (COVID-19) vaccine, we also measured tetanus-specific antibody titers elicited by the TDaP vaccine that is administered during the third trimester of pregnancies. Tetanus EPTs in maternal plasma of the case participant were low at the first evaluated timepoint (60 DPV that is 4 months postdelivery) and declined sharply thereafter. Although Control 2 had an initial EPT response similar to the case participant, the decline in titer overtime was less steep than that observed in the case participant. In contrast, Control 1 had a much higher initial tetanus antibody titer than the case participant and Control 2, and continuously declined overtime (Fig. 1C).
We next probed the evolution of RBD antibody titers in human milk. Although Control 1 had high RBD titers at 104 DPV that halved over the following 3 months and remained consistent thereafter, the case participant had low initial RBD titers that continuously waned from enrollment until 2 days after SARS-CoV-2 diagnosis on 216 DPV (Fig. 1D). After administration of monoclonal antibodies on 222 DPV, there was a steep and immediate increase in RBD antibody titers in human milk that first declined slowly over the next 3 months, followed by a steeper decrease leading to barely detectable titers 564 DPV or 10 months postmonoclonal antibody treatment.
To investigate whether the defect in antibody titers in the case participant was due to impairment of cell frequency or function, we first determined the composition of white blood cell populations by CBC analysis and observed no significant differences in lymphocytes, monocytes, or granulocytes (Fig. 1E) in the case participant versus control participants at 6 months postpartum. Notably, the case participant and Control 2, who both had low antibody titers, had low B cell frequencies (Fig. 1F) compared with Control 1 who had higher B cell frequency and antibody titer (Fig. 1C, F).
In addition, the case participant appeared to have more dendritic cells (DCs) and CD4 T cells, as well as fewer monocytes than the two controls (Fig. 1F). This prompted us to investigate more closely these cell compartments (Fig. 1G–I). This analysis revealed that the case participant had a greater percentage of naive CD4 and CD8 T cells and lower effector memory (EM), central memory, and terminally differentiated effector memory CD4 and CD8 T cells compared with control participants (Fig. 1G, H). Finally, there was no defect in the functionality of myeloid cells (DCs and monocytes) as determined by expression IL-6 and TNF-α cytokines after stimulation with a bacterial TLR ligand cocktail (Fig. 1I).
Discussion
In this case report, a breastfeeding woman experienced a breakthrough symptomatic SARS-CoV-2 infection at 9 months postpartum and was treated with a monoclonal antibody infusion of casirivimab–imdevimab 5 days postdiagnosis. She had minimal to absent SARS-CoV-2 RBD antibody levels in her plasma and human milk samples until she received mAb therapy, which led to a transient increase in antibody titers in both compartments. No obvious defects in the innate or adaptive immune cell populations were identified that could explain the lower levels of RBD-specific antibodies after vaccination in the case patient. She recovered fully, and continued exclusive breastfeeding of her healthy infant.
mAb therapies are commonly used to treat autoimmune conditions, including diseases such as inflammatory bowel disease and multiple sclerosis that occur in reproductive-age individuals.12–14 Although women historically were recommended to either forego breastfeeding or treatment until weaning, recent studies have reported low mAb transfer into human milk (antibody level of 1:100 to 1:200 compared with maternal plasma) 15 without evidence of developmental delay or serious infections in the offspring.16,17
This is due to the fact that many antibodies used in therapies are IgG1 molecules that do not have a high transfer efficacy between the plasma and human milk compartments. 18 Few studies have reported on the use of COVID-19 mAb therapies in pregnant and/or breastfeeding people. 7 One woman was also treated with an intravenous infusion of casirivimab–imdevimab at a lower dose of 300–300 mg 5 days before delivering vaginally a healthy newborn. Breastfeeding was initiated 3 days after disappearance of maternal symptoms and the infant remained healthy 1 month postbirth. 19 As our case study focused on the breastfeeding individual, the relative infant dose (RID) of casirivimab–imdevimab was not determined.
Of note, the RID of all the mAb therapies for COVID-19 is still unknown, but as these are human broadly neutralizing antibodies specific for SARS-CoV-2 spike protein, and since antibody transfer from maternal plasma to human milk is low, no toxicity to the infant is expected and a potential protective effect is anticipated.
Footnotes
Authors' Contributions
Design and conception of the study were contributed by N.E.M. and I.M. Investigation was taken care by M.B.B. and B.M.D. Visualization was done by B.M.D. Writing—original draft was done by D.C.M., N.E.M., and I.M. Writing—review and editing was carried out by N.E.M., M.B.B., B.M.D., D.C.M., M.R., and I.M. Supervision was done by N.E.M., M.R., and I.M. Funding acquisition was carried out by I.M. and N.E.M.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by grants from the National Institutes of Health R01AI145910 (I.M.) and R01AI142841 (I.M.). The funding source had no involvement in study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.