
Abstract
Background:
Pregnant and lactating women were not included in the initial large vaccine clinical trials for SARS-CoV-2 (COVID) infection. Delineating the antibody titers in serum and breast milk of lactating women is important to determine the safety and benefits of vaccination in this special population.
Objective:
To investigate COVID vaccinations in breastfeeding dyads and effects on lactation, the Antibody Detection of Vaccine-Induced Secretory Effects trial (ADVISE) prospectively evaluated anti-COVID antibodies in serum and breast milk after initial paired and booster vaccines.
Methods:
This is a prospective longitudinal surveillance cohort study of lactating women. Eligibility criteria included ≥18 years of age, currently lactating, and at enrollment either received COVID vaccination within the past 60 days or planning vaccination within 60 days.
Results:
Among 63 lactating mothers, COVID vaccination led to breast milk secretory IgA (sIgA) and IgG antibodies with consistent viral neutralizing activity. Milk sIgA titers increased further after second vaccination and were prolonged after a third booster dose, including women with extended breastfeeding beyond 12 months. Milk IgG antibody titers were higher and more sustained than sIgA. Antibody titers were not associated with individual dyad characteristics or vaccine manufacturer. Vaccine-induced antibodies from milk were not detected in infant circulation.
Conclusions and Relevance:
Maternal COVID vaccination during lactation is well tolerated and generates sustained and boosted antibody responses in breast milk. COVID-specific sIgA and IgG antibodies with neutralizing activity are found in breast milk, including boosted mothers who continue breastfeeding beyond 12 months. These data support universal COVID vaccinations for all lactating mothers, including booster immunizations during extended breastfeeding (NCT04895475).
Introduction
Breastfeeding is recommended as the normative standard of nutrition for all infants by the American Academy of Pediatrics (AAP) and other major health care institutions. Breastfeeding is associated with a reduced risk for a myriad of short- and long-term health conditions for both mother and child.1,2 Key to improved health outcomes is the immune protection conferred through human milk, related to many bioactive factors including immunoglobulins, oligosaccharides, lactoferrin, cytokines, and other bioactive substances. 3
As the global and pandemic spread of the novel coronavirus (SARS-CoV-2) began in 2020, there were early knowledge gaps regarding the epidemiology and transmission of infection, the immunological responses after viral exposure, and the immunological protection through vaccine administration. Cincinnati, Ohio, had its first confirmed case of COVID-19 on March 14, 2020, and despite extensive shelter-in-place and social distancing efforts, community spread continued with several distinct infection surges. 4
The SARS-CoV-2 pandemic has now affected all ages of the global population. Pregnant and lactating mothers are susceptible to the virus, and early concerns about infant feeding and separation of mother and baby created multiple challenging and changing recommendations due to early unknown effects on the infants.5,6 Perinatal COVID-19 registry data on more than 7,524 cases of mothers positive for COVID-19 from 14 days before delivery and up to 10 days after delivery found 2.2% of infants tested positive. 7 However, a recent systematic review concluded that vertical acquisition of SARS-CoV-2 is likely to be rare and related to the severity of maternal infection. 8 Current guidance suggests that the risk of COVID acquisition in the birth hospital is low, and with proper hygiene precautions, mothers and babies should stay together (room-in) and breastfeed directly. 9
Concerns about maternal COVID infection or vaccination for the breastfeeding infant appear to be unfounded. Recent evidence from both clinical and laboratory studies documents that natural SARS-CoV-2 infection is unlikely to be transmitted through human milk, as detected viral particles in breast milk have not been found to be infectious. 10 After natural maternal infection, human milk has been found to have specific antibodies to SARS-CoV-2.11–13 Moreover, maternal vaccination with two doses of mRNA vaccine has been associated with a reduced risk for hospitalization for COVID-19 for infants younger than 6 months of age. 14
When COVID-19 vaccines were first authorized for use under Emergency Use Authorization in late 2020, no pregnant or lactating individuals were included in the early clinical trials; however, many lactating women were included in categories prioritized to receive the vaccine, such as health care workers. The Academy of Breastfeeding Medicine had early recommendations that breastfeeding need not discontinue in lactating mothers who received the vaccine and outlined the unlikelihood of harm from the vaccine, and more likely the plausible benefits. 15 Similarly, the American College of Obstetrics and Gynecology and the Society for Maternal and Fetal Medicine made early recommendations that lactating mothers could receive the COVID-19 vaccine.16,17
As COVID-19 vaccines became available, we recognized the opportunity to understand the immunological response to vaccination and to contrast them to the effects of natural infection. Of particular interest was the immunological response of lactating women to SARS-CoV-2 vaccination, particularly their production of viral-specific, breast milk secretory IgA (sIgA) antibodies that potentially confer protection to the breastfeeding infants. Several studies have detected sIgA in breast milk after COVID vaccination,18–21 and both the Centers for Disease Control and Prevention and AAP now recommend that lactating persons receive the vaccine.22,23 A recent study documented persistence of specific antibody up to 6 months after vaccination. 24 Many questions remain, however, including the long-term sustainability of antibody titers in breast milk, especially among mothers who continue breastfeeding beyond 1 year, and whether an additional booster is effective for increasing breast milk antibody titers.
To advise mothers asking these questions about vaccine efficacy and safety, we devised a prospective longitudinal surveillance research study, enrolling actively lactating women who received the SARS-CoV-2 vaccine, and followed their clinical and laboratory parameters for up to 24 months. Our overall goal was to investigate the characteristics of breast milk and serum antibody formation in lactating women receiving COVID vaccination, documenting the antibody isotypes, titers, duration, and transfer into milk over time, including durability of humoral immune responses. An optional component was a periodic blood testing of the breastfeeding child to determine the possibility of generating even small amounts of specific antibody-based immunity. Our primary objective was to document the prevalence and cumulative incidence of secretory antibody responses in breast milk to SARS-CoV-2 vaccines, especially among women with extended breastfeeding, and to gain insights into the protective immunological effects of elective vaccine administration.
Materials and Methods
Study design
Antibody Detection of Vaccine-Induced Secretory Effects (ADVISE, NCT04895475) was a prospective longitudinal surveillance cohort study to evaluate breast milk antibodies among lactating women who received COVID vaccination. The study was approved by the Cincinnati Children's Hospital Medical Center Institutional Review Board.
Recruitment and retention
Enrollment criteria included mothers at least 18 years of age, currently lactating, with either COVID vaccination in the past 60 days or planned in the next 60 days. Mothers were recruited primarily from the Cincinnati area, by word of mouth or recruitment flyer, beginning in February 2021. They were followed before COVID vaccine in most cases, and all were followed until the time of weaning, withdrawal from the study, or study closure.
COVID vaccination
The initial paired vaccinations against SARS-CoV-2, as well as subsequent booster immunizations, were administered in local health care settings and were not given as part of this study. At the time and location of this study design, the main choices were Moderna and Pfizer vaccines.
COVID-related special considerations
Because of the restrictions of the COVID pandemic in early 2021, and the fact that lactating mothers and young babies could not easily attend in-person research visits, we devised a fully electronic consent and data collection system for demographic information and vaccine-related data, which were entered into a Research Electronic Data Capture (REDCap) database. 25 We received breast milk samples from before and after vaccination at specific time intervals and developed an innovative “drive-by” research visit for mothers to drop off their frozen milk samples. Blood samples were obtained using a microsampler device, on the mothers while in their cars, and optionally blood samples were taken from infants while in their car seats.
Data and sample collection
After enrollment, maternal and infant demographics, plus breastfeeding characteristics including exclusivity, vaccination type, and side effects were recorded in REDCap. Mothers were classified as either breastfeeding exclusively, offering complementary food, or providing supplemental formula. Milk samples before vaccination, and weekly after Vaccine Dose 1 and Dose 2, were delivered using our convenient drop-off system. For women who obtained a third booster vaccine while lactating, milk was collected monthly. Maternal blood samples at monthly intervals, along with optional infant samples using a finger-stick Mitra® 10 μL microsampler device (Neoteryx, Torrance, CA), were also collected. Exposures included whether mothers had previously been infected with SARS-CoV-2 and whether they had received a COVID vaccination during pregnancy. Additionally, the type of vaccine was noted as an exposure variable.
Laboratory testing
The primary laboratory outcomes were IgG, IgA, IgM, and secretory component specific to the SARS-CoV-2 Spike protein, using internally prepared recombinant proteins and standard quantitative enzyme-linked immunosorbent assay (ELISA) techniques. 4 All milk samples and maternal serum samples were tested for antibodies against the Spike protein and the SARS-CoV-2 Receptor Binding Domain (RBD) protein by ELISA assay. Selected milk samples with high IgA and IgG titers were further tested for viral neutralizing antibodies. Most mothers “opted in” for infant serum collection, so these sera were also tested for the same antibodies.
Breast milk samples were collected and frozen at −80°C until processing, which involved initial centrifugation at 2,000 g for 10 minutes at 4°C to generate a fat-free supernatant between the bottom cell pellet and the top cream layer. 26 The supernatant milk was then aliquoted and tested by ELISA for reactivity against the SARS-CoV-2 proteins at both 1:4 and 1:10 dilutions, which were shown in preliminary experiments to give reproducible results without high background. Serum samples were stored at −80°C until analysis at 1:200 and 1:400 dilutions. Pre-vaccine samples were used as negative controls, and an absolute value of 0.4 optical density was considered positive, representing three standard deviations above the average negative value.
Selected milk samples were also tested for viral neutralizing antibodies using a pseudovirus blocking assay that measures the ability of the antibodies to block binding between the viral Spike protein and its membrane-bound receptor, using modifications of a published protocol. 27
Results
Enrollment
Study recruitment occurred using advertisements, referrals from breastfeeding medicine providers, and personal communication from study participants to their own acquaintances. A total of 66 women consented with enrollment, quickly exceeding the predicted pace (Fig. 1). Three mothers withdrew before sample collection, due to plans to wean before scheduling their first vaccination. Among the 63 mothers who provided breast milk samples, all provided blood on themselves and 52 allowed blood collection from their breastfeeding infants (Fig. 2). Between February 2021 and May 2022, a total of 1,009 breast milk samples were collected for analysis, including 209 from women with extended breastfeeding beyond 12 months of age. Similarly, a total of 464 blood samples from mothers and infants were collected for analysis.

Projected and enrollment in the ADVISE trial. Actual enrollment was much more rapid than anticipated. Withdrawal from the trial was due to natural or scheduled weaning of lactation, as well as three mothers who withdrew electively without providing any samples for analysis. ADVISE, Antibody Detection of Vaccine-Induced Secretory Effects.

CONSORT diagram of study participants in ADVISE. A total of 66 women enrolled, and most received an initial two-vaccine immunization series. Breast milk and blood samples were collected serially for up to 9 months. A total of 22 women were still breastfeeding when they received a third booster vaccine and had up to 6 months of sample collection thereafter. CONSORT, Consolidated Standards of Reporting Trials.
Demographics
Table 1 provides a summary of the enrollment demographics. The median age of our participants was 35 years, with a range of 23–43 years, and most mothers self-identified as White. Almost half of the mothers (29, 46%) were exclusively breastfeeding, while 26 (41%) were offering complementary foods and only 8 women (13%) were providing supplemental formula. The median infant age at enrollment was 7 months with a range of 0–42 months, including four infants older than 12 months of age. A small number of babies were born prematurely or post-dates.
Maternal, Infant, and Vaccine Characteristics in ADVISE
Only 5 mothers had a history of COVID infection at enrollment, but 10 had antibodies detected in serum and milk at enrollment, consistent with 5 undocumented infections.
Refers to age (months) of infants whose mothers were immunized after delivery.
The vaccine manufacturer for the initial paired two-part immunization schedule was 57% Moderna and 43% Pfizer (Table 1). Mothers were predominantly vaccinated during lactation (87%), although eight (13%) were vaccinated while pregnant. There were five mothers who reported having documented COVID before study enrollment (three while pregnant, two while lactating), but still received vaccination.
Effects of vaccination on breastfeeding
The majority of lactating mothers reported no adverse effects of vaccination on their breast milk or breastfeeding. Only two mothers reported a temporary decrease in milk supply, and one reported transient “blue milk” discoloration.
Antibody responses
The measured antibody responses in the breast milk are illustrated in Figure 3. For the entire cohort of 63 women who contributed breast milk samples, sIgA against the Spike protein was found in 90% of mothers ∼14 days after Vaccine Dose 1, which decreased to 65% by day 28 after first immunization. This decline was reversed 14 days after Vaccine Dose 2, as breast milk sIgA titers increased and were detected in 84% of mothers. The sIgA titers against Spike protein then decreased 2 months after the initial two vaccinations but were still detected up to 9 months later in over half of the mothers (Fig. 3, upper left panel), documenting sustained sIgA levels in many mothers with extended breastfeeding. At the last 9-month breast milk measurement, these infants were a median of 12 months of age, range 7 to 47 months.
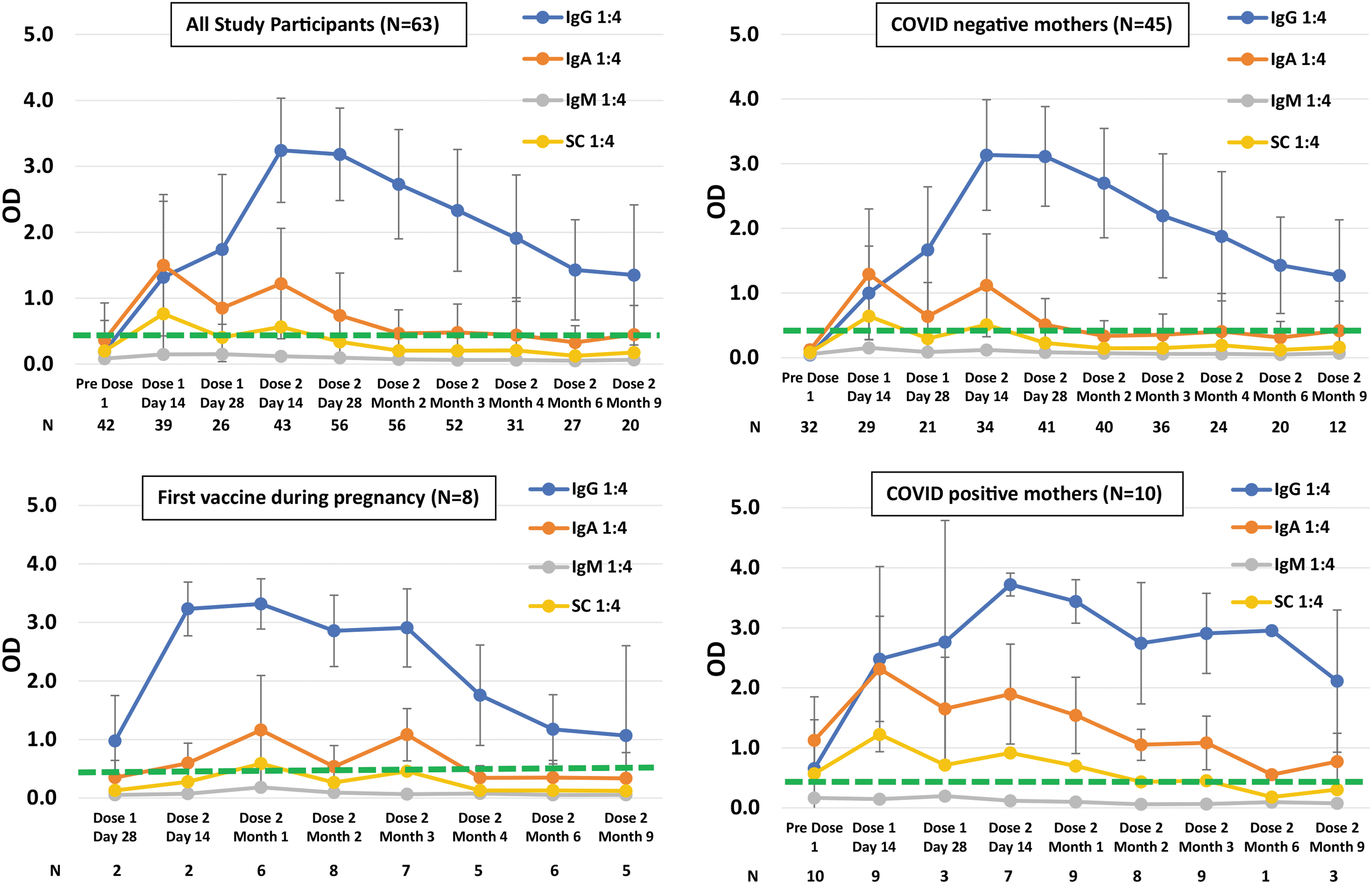
Breast milk antibody responses after the initial COVID paired two-dose vaccine series in the ADVISE trial. OD refers to optical density, the quantitative measure of antibody titers, with 0.4 (
Additional analyses were then explored within this cohort, based on prior exposure to COVID vaccine or natural infection. Figure 3 (upper right panel) illustrates the results for 45 COVID-naive mothers (negative IgG serum titers at study entry), with a similar pattern of initial breast milk sIgA titers that increased after the second dose, but with inconsistently detectable IgA titers in the milk 2 months after the second vaccine dose. Figure 3 (lower left panel) illustrates the results for eight mothers who received their first COVID vaccine during pregnancy, with measurable IgA titers in breast milk at 3 months after the second vaccine dose. Figure 3 (lower right panel) illustrates the results for 10 COVID-positive mothers (positive IgG serum titers at study entry without vaccination), which was expected in the five mothers with documented COVID during pregnancy or lactation, but unexpected in five others who did not have a documented infection. These mothers had much higher IgG and IgA levels in milk with sustained titers out to 9 months from the second paired vaccine dose. Breast milk antibodies also reacted with the RBD of the Spike protein (data not shown).
Maximum sIgA titers in breast milk were not associated with maternal age, race, or vaccine manufacturer (Moderna or Pfizer mRNA vaccines). Many breast milk samples contained viral neutralizing antibodies, which were sustained over time (data not shown). Infant serum had SARS-CoV-2 antibodies detected only in mothers with COVID infection during pregnancy or vaccination during pregnancy.
Boosted antibody responses
A total of 22 lactating mothers later received a third (booster) SARS-CoV-2 vaccine dose while still breastfeeding (median infant age = 13 months, range = 7–47 months). The majority of milk samples for this cohort (49/66, 74%) were collected from women with extended breastfeeding beyond 12 months, and significant antibody responses were observed in both IgG and sIgA antibody titers measured after the booster dose (Fig. 4). Specifically, sIgA titers were increased in all lactating women who received a third booster vaccine and were detectable even 6 months after the third vaccine dose.
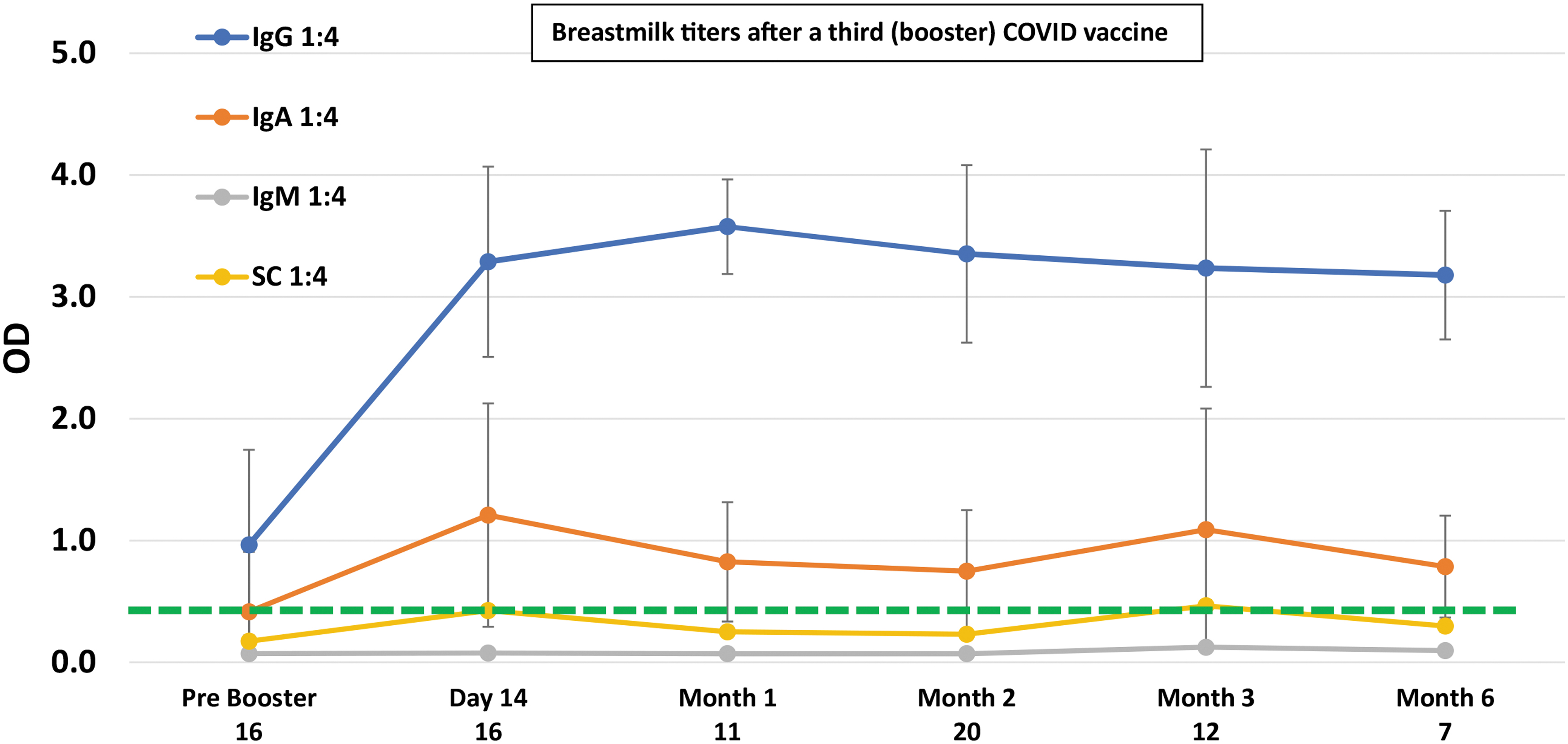
Antibody responses after a third COVID booster vaccination. A total of 22 women had a third vaccine administered while breastfeeding, which led to increased breast milk antibody titers of sIgA and IgG still measured 6 months later. After the booster, 49 of 66 tested milk samples (74%) were from mothers with extended breastfeeding beyond 12 months. OD refers to optical density, the quantitative measure of antibody titers, with 0.4 representing the threshold for a positive value at three times the standard deviation of negative control samples.
Discussion
Since its first known appearance in the human population in late 2019, the SARS-CoV-2 virus has spread widely and rapidly worldwide, sparing no age group. The rapid development of a vaccine helped to stem the tide of escalating infection, but only as much as families have been willing to be vaccinated. Vaccine hesitancy for the COVID-19 vaccine has been unfortunate and pervasive. 28 Predictably, pregnant and lactating women were extremely concerned about the vaccine, as there was no existing framework for their inclusion in early clinical trials. Yet these very groups were uniquely poised to protect their newborns long before a manmade vaccine could be developed for the young infant through their production of breast milk antibodies.
Due to a lack of research among pregnant and lactating women, there was slow and incomplete early official guidance recommending vaccination to this special and vulnerable population, leading to uncertainty about vaccination against COVID. The Task Force on Research specific to Pregnant Women and Lactating Women (PRGLAC) recommends studying pregnant and lactating women in research, rather than excluding them, to help counteract this exact scenario. 29
As time progressed, studies have shown lack of ill effects from the COVID vaccine for lactating women and their infants30,31 beyond the typical side effects noted for the general population, and more and more pregnant and breastfeeding women have received vaccinations. A recent systematic review of maternal and neonatal outcomes found no major side effects in 5,098 lactating women. 32 Predictably, several studies showed early antibody responses with IgA and IgG in breast milk, and even T cells with viral-specific neutralizing functionality after vaccination.33–35 Our results mirror these studies, as well as a recent meta-analysis and systematic review that found 64% positive for IgA after the first dose, and 30% positive for IgG, but higher titers (70% positive for IgA and 91% positive for IgG) after the second dose. 36 These antibodies will likely play a role in infant immunity to COVID-19, along with other abundant and potent immune factors found in human milk. 37
We confirmed that sIgA antibodies are formed in breast milk after initial paired vaccinations (Fig. 3), which play a significant role in infant health, especially in the critical early-life window. The importance of identifying sIgA antibodies against the Spike protein and the specific RBD, along with neutralizing capability, is highly significant for vaccinated mothers. sIgA protects the infant at the mucosal level of the gastrointestinal and respiratory tracts and helps to develop a healthy microbiome and influence immune system development. 38
By design, the ADVISE protocol prospectively followed lactating mothers for an extended period of time after the initial paired vaccination. We found sIgA in the milk of ∼50% of mothers 6 months after the initial paired vaccination series, similar to previously reported, 24 but in ADVISE, we detected antibodies even longer, with some having positive breast milk titers out to 9 months post-vaccination (Fig. 3, upper left panel). Mothers who received their first vaccine dose during pregnancy had higher sIgA titers 3 months following the paired vaccine series (Fig. 3, lower left panel), whereas COVID-positive mothers had even higher breast milk sIgA and IgG antibody titers (Fig. 3, lower right panel).
We also identified breast milk sIgA antibodies in mothers with older babies and in those taking solid foods. Importantly, antibodies were found in breast milk even with extended breastfeeding beyond 12 months of age, and a third booster immunization was effective for increasing the breast milk antibody titers even further. These mothers had positive sIgA titers measured up to 6 months after the booster vaccine (Fig. 4). Taken together, these observations suggest extended breastfeeding in vaccinated women continues to provide targeted immunity to SARS CoV-2, which aligns with the new AAP Policy statement that recommends continued breastfeeding for at least 2 years and beyond. 1
As expected, we observed that only mothers with previous COVID-19 infection or SARS-CoV-2 vaccination during pregnancy transferred IgG antibodies into the infant serum. 39 Although we did not find viral-specific IgG in infant serum samples collected from most study participants, IgG in maternal milk may still activate opsonization of antibody-coated viral particles by infant immune cells and promote the infant's own adaptive immunological responses. 40 This finding may help to encourage women to get vaccinated during pregnancy, so that their infants may receive this added immunological bonus. Women who received an initial vaccine dose during pregnancy had slightly higher titers than those who waited until after birth (Fig. 3) and were the only ones who transferred antibodies into their infant's circulation.
In summary, the initial two-dose paired COVID vaccination series is well tolerated in lactating mothers with very few side effects related to breastfeeding. Both Moderna and Pfizer mRNA vaccines generated strong immune responses with sIgA extending for up to 6–9 months, especially in women with prior COVID infection. Infants also received the sustained benefit of maternal vaccination through extended breastfeeding beyond 12 months. sIgA antibodies were routinely detected in the breast milk of COVID-vaccinated mothers, some with strong viral neutralizing activity. Breast milk sIgA titers persist for several months after initial vaccination and then were increased substantially and further prolonged after the third booster vaccine dose. These data support COVID vaccination for all lactating mothers, including booster immunizations for mothers with extended breastfeeding.
Footnotes
Acknowledgments
The authors appreciate the efforts of Adriane Hausfeld, Nick Jakubowski, and Amanda Pfeiffer in the organization and collection of samples. We also thank Dr. Andrew Herr and Dr. Michael B. Jordan for their early work to develop recombinant SARS-CoV-2 proteins used in the ELISA assays. Breast milk–neutralizing antibody assays were completed by Mr. Michael Jordan, and laboratory supervision was provided by Thad Howard.
Authors' Contributions
J.W.: Conceptualization, methodology, writing—original draft, writing—review and editing, and visualization. K.M.: Investigation, data curation, and writing—review and editing. T.L.: Software, formal analysis, data curation, and writing—review and editing. A.L.: Software, and formal analysis. K.D.-S.: Investigation. D.H.: Methodology, resources, writing—review and editing, and supervision. P.S.: Methodology, resources, and supervision. R.E.W.: Conceptualization, methodology, writing—original draft, writing—review and editing, supervision, project administration, and funding acquisition.
Disclosure Statement
The authors have no financial relationships relevant to this article to disclose.
Funding Information
Funding provided by the CARES Act and the Cincinnati Children's Research Foundation.