
Abstract
Background:
Lack of mother's own milk (MOM) at discharge from the neonatal intensive care unit (NICU) is a global problem and is often attributable to inadequate MOM volume. Evidence suggests that the origins of this problem are during the first 14 days postpartum, a time period that includes secretory activation (SA; lactogenesis II, milk coming in).
Objectives:
To describe and summarize evidence regarding use of MOM biomarkers (MBMs) as a measure of SA in pump-dependent mothers of preterm infants in the NICU and to identify knowledge gaps requiring further investigation.
Methods:
An integrative review was conducted using Whittemore and Knafl methodology incorporating the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) checklist. A search using electronic databases MEDLINE (through PubMed) and CINAHL (Cumulative Index to Nursing and Allied Health Literature) and reference lists of included articles was conducted.
Results:
Of the 40 articles retrieved, 6 met the criteria for inclusion. Results revealed the following five findings: (1) Achievement of SA defined by MBMs is delayed and/or impaired in mothers of preterm infants. (2) MBMs are associated with pumped MOM volume. (3) Achievement of SA defined by MBMs is associated with pumping frequency. (4) Delayed and/or impaired achievement of SA defined by MBMs may be exacerbated by maternal comorbidities. (5) There is a lack of consensus as to which MBM(s) and analysis techniques should be used in research and practice.
Conclusions:
MBMs hold tremendous potential to document and monitor achievement of SA in mothers of preterm infants, with multiple implications for research and clinical practice.
Introduction
Mothers of preterm infants hospitalized in the neonatal intensive care unit (NICU) initiate lactation and provide mothers' own milk (MOM) at rates that often approach or exceed those for mothers of healthy term infants.1–4 These rates reflect the knowledge among NICU staff that high-dose MOM feedings are effective in reducing the risks and associated costs of necrotizing enterocolitis, late-onset sepsis, bronchopulmonary dysplasia, retinopathy of prematurity, neurodevelopmental problems, and post-NICU acute care use and rehospitalization in preterm infants.5–7 These high initiation rates are also consistent with studies showing that mothers of preterm infants change the decision from formula feeding to MOM provision when they receive targeted educational messaging from NICU staff.5,8,9 However, high MOM provision rates do not continue through to NICU discharge, despite mothers' self-reported intentions.3,10,11
A primary reason for lack of MOM feedings through to NICU discharge is insufficient quantities of MOM to meet the infant's required feed volumes. The phenomenon of “running out of milk” is ubiquitous among breast pump-dependent mothers of preterm infants and has been attributed to modifiable (e.g., pumping behaviors) and nonmodifiable (e.g., breast pump dependency, maternal health conditions, household income) factors.12–16 Previous studies by this research team have demonstrated that in the preterm population, the first 14 days postpartum represent a critical lactation window for addressing modifiable factors that predict MOM receipt later during NICU hospitalization and at NICU discharge.17,18 This time period includes secretory activation (SA; lactogenesis II, milk coming in) and achievement of “coming to volume” (CTV; removing ≥500 mLs/day of pumped milk by day 14 postpartum).18,19 Achievement of CTV independently predicts receipt of MOM at NICU discharge in preterm very low birthweight (VLBW; <1,500 g) infants. 17
SA is triggered by the rapid decline in progesterone following delivery of the placenta and must be achieved for lactation to continue long term. 20 Several studies indicate that SA is delayed and/or impaired in breast pump-dependent mothers of preterm infants, despite the fact that SA is inconsistently and often unreliably measured in research and clinical practice. 21 In particular, maternal perceptions of milk coming in, the most commonly used indicator of SA, have not been validated concurrently with another objective measure of SA in mothers of preterm infants. 21
Increases in pumped MOM volume, including the threshold attainment of 20 mL of expressed MOM from two consecutive pumping sessions, have also been suggested as an indicator of SA.19,22 This measure is limited because pumped MOM volume involves both MOM production and removal, thus being dependent on the effectiveness of the breast pump and pumping behaviors in addition to actual MOM production.21,23 Clearly, there is a priority for evidence-based measures of SA in both research and practice to address the lack of MOM through to NICU discharge and beyond in this vulnerable population. 21
The use of serial MOM biomarkers (MBMs) of SA in mothers of preterm infants may provide an accurate, reliable, feasible, and potentially cost-effective approach to the identification and management of mothers at risk for delayed and/or impaired SA.18,19,21,24 These MBMs, which include sodium (Na), sodium:potassium ratio (Na:K ratio), lactose, citrate, and total protein, have been the gold standard for measuring SA in lactation research for over three decades.21,25 Serial increases or decreases in individual MBMs reflect biologic changes in the mammary gland that occur during the transition from secretory differentiation to SA. 21 Normal ranges for each MBM have been used to characterize SA in healthy term populations, and are shown in Box 1.
Mother's Own Milk Biomarker Reference Ranges
Adapted from Medina Poeliniz et al. 21
Values of ≤20 or ≤16 are study specific, and represent small sample sizes and differing days postpartum.
However, little is known about the extent to which these values are affected by preterm birth (interrupted secretory differentiation) and its associated lactation risk factors such as inflammatory maternal health complications (overweight and obesity, preeclampsia and eclampsia, diabetes and gestational diabetes, and associated medications to manage these conditions), maternal stress, and breast pump dependency, all of which are much more common in mothers of preterm infants.18,26,27
Leveraging MBMs as predictor and outcome variables in research as well as diagnostic clinical tools to personalize data-driven clinical lactation care for at-risk mothers holds promise. However, a thorough review of research on MBMs of SA in breast pump-dependent mothers of preterm infants admitted to the NICU is lacking. Thus, the aims of this integrative review are to describe and summarize evidence regarding the use of MBMs of SA in breast pump-dependent mothers of preterm infants in the NICU and to identify knowledge gaps requiring further investigation.
Methods
Observational studies and randomized control trials investigating MBMs of SA in mothers of preterm infants admitted to the NICU were included in this review. Nonhuman-based studies were excluded. An integrative review was conducted using Whittemore and Knafl 28 methodology incorporating the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. A search using electronic databases MEDLINE (through PubMed) and CINAHL (Cumulative Index to Nursing and Allied Health Literature) and reference lists of included articles was conducted.
Search strategy
To identify eligible studies, a search was conducted with electronic databases MEDLINE (through PubMed) and CINAHL (Cumulative Index to Nursing and Allied Health Literature). In addition, reference lists of included articles were examined. Our search was conducted in October 2022, was limited to studies in English, and used a combination of different groups of keywords (free text and MeSH [Medical Subject Headings] terms) that described the population and outcomes of interest (Supplementary Table S1 Search Strategy). All titles and abstracts identified by our search were screened for relevance by a single author (L.A.P.). The full texts of those considered relevant were retrieved and evaluated for inclusion relevancy by three authors (M.M.B., R.H., and L.A.P.) who independently performed data extraction and a single author (M.M.B.) collected the following information: first author's name, year of publication, study design, setting, and results (Table 1).
Summary of Included Studies
BMI, body mass index; CI, confidence interval; CTV, coming to volume; GA, gestational age; IQR, interquartile range; K, potassium; MBM, MOM biomarkers; MOM, mother's own milk; Na, sodium; OR, odds ratio; SA, secretory activation; SD, standard deviation; WNL, within normal limits.
Data analysis
We synthesized data obtained from the included studies and all discrepancies between reviewers regarding study selection process, data extraction, synthesis, and interpretation were discussed until a final agreement was reached.
Results
Forty articles were retrieved from databases and reference lists of identified articles. After removing duplicates, 36 articles were screened by title and abstract. Of these, 30 were unrelated to MBMs of SA in mothers of preterm infants in the NICU and excluded, leaving 6 potential articles. After reviewing full texts, all six met the inclusion criteria, of which five were observational studies and one was a secondary analysis of data (Fig. 1). Studies originated in the United States and Australia with sample sizes ranging from 16 to 69. Five of the six studies clarified that mothers were breast pump dependent. Table 1 summarizes included studies.
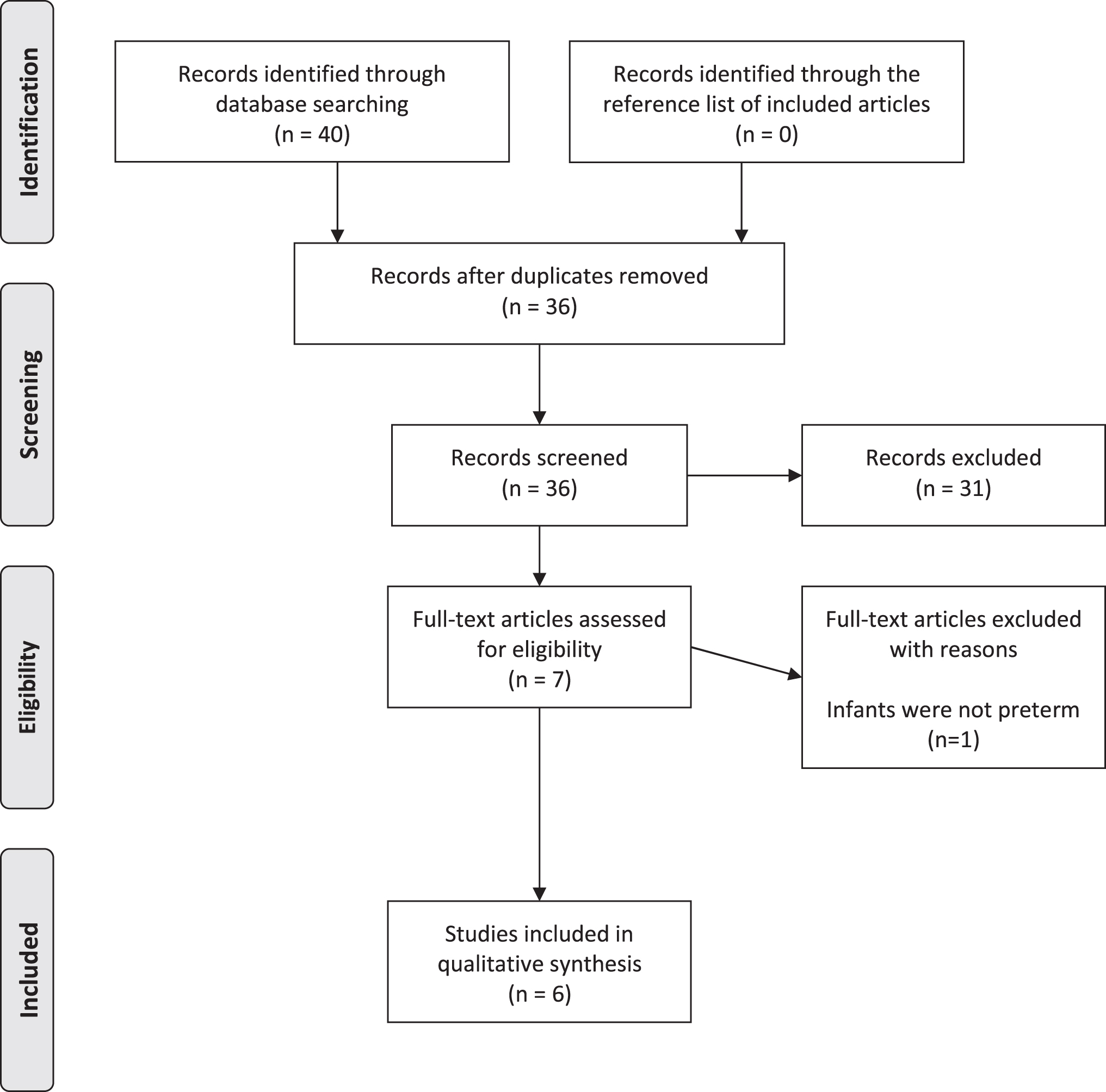
PRISMA flow diagram.
The results revealed the following five major findings (Box 2): (1) Achievement of SA defined by MBMs is delayed and/or impaired in breast pump-dependent mothers of preterm infants. (2) MBMs are associated with pumped MOM volume. (3) Achievement of SA defined by MBMs is associated with pumping frequency. (4) Delayed and/or impaired achievement of SA defined by MBMs may be exacerbated by maternal comorbidities. (5) There is a lack of consensus as to which MBM(s) and analysis techniques should be used in research and practice.
Five Major Findings
MBMs, MOM biomarkers; MOM, mother's own milk; SA, secretory activation.
Achievement of SA defined by MBMs is delayed and/or impaired in breast pump-dependent mothers of preterm infants
Five studies revealed either delayed (eventually occurred) and/or impaired (never occurred) SA in mothers who delivered preterm, regardless of which specific MBMs were measured and which analyses were performed.18,19,29–31 Historically, the first study to characterize delayed SA in mothers of preterm infants remains a classic work, despite its limitations of enrolling only 22 mothers of moderately preterm infants (31–35 weeks of gestational age [GA] at birth) and 16 mothers of healthy term infants (>38 weeks of GA), and measuring outcome variables (MBMs, MOM prolactin concentration, and 24-hour MOM volume) only on day 5 postpartum. 29 Cregan et al. 29 defined achievement of SA as having all four primary MBMs (Na, lactose, citrate, total protein) within normal limits (WNL; ±3 standard deviations from published normative values for mothers of healthy breastfeeding infants), and compared this dichotomous outcome (yes/no) for the two groups of mothers.
All 16 mothers of healthy term infants had achieved SA on day 5 postpartum compared with 18% of mothers of preterm infants. Cregan et al. 29 also reported the percentages of mothers of preterm infants with three (14%), two (32%), and one (36%) MBM WNL. This study was the first to show a biological basis for clinicians' reports of delayed SA in mothers of preterm infants while clarifying that MBM deviations were not a function of altered prolactin, which was statistically similar between the groups.
Hoban et al. 30 reported delayed SA in a 2018 pilot study of 16 breast pump-dependent mothers of very preterm infants (<33 weeks of GA), for whom the following data were collected during the first 14 days postpartum: twice-daily MBMs (Na and Na:K ratio, lactose, citrate, total protein), daily pumped MOM volume (weighed to the nearest 0.1 g), and frequency of breast pumping sessions as recorded by mothers. Using Cregan et al.'s 29 characterization of SA, Hoban et al. 30 reported that only 40% of mothers had all four primary MBMs WNL by day 5 postpartum. Of the 50% of mothers who achieved SA by day 14 postpartum, all had four MBMs WNL at 5.4 ± 3.5 days and reported significantly more cumulative pumping sessions between birth and day 5 postpartum.
This small pilot study was pivotal for two reasons: it was the first to establish a mean time postpartum for achievement of SA in mothers of very preterm infants using MBMs, and it demonstrated the research feasibility of daily sampling of MBMs and MOM pumped volumes during the first 14 days postpartum in this vulnerable population.
Hoban et al. 18 subsequently published on the entire cohort (n = 39) for the abovementioned study. Findings revealed that on day 5 postpartum, well past the normal 72-hour threshold when healthy mothers with term infants should experience SA, only 50% and 32.3% of mothers had achieved SA as defined by Na <16 mM or Na:K ≤0.8, respectively.32,33
In 2021, Parker et al. 19 studied 69 mothers of VLBW infants (≤32 weeks of GA) during the first 7 days postpartum. Timing of SA was compared using three separate indicators: maternal perceptions of milk coming in; removing ≥20 mL of MOM per pump session for two consecutive sessions; and WNL MBMs Na and lactose (collected when pumped MOM was ≥20 mL per pumping session for two consecutive sessions). Compared with normal values in healthy breastfeeding mothers, SA in this cohort was delayed. Maternal perception of milk coming in occurred at mean 130.6 ± 170.3 hours postpartum and achievement of ≥20 mL of pumped MOM volume for two consecutive pump sessions occurred at mean 123.4 ± 91.9 hours postpartum. Only 42% of mothers had WNL MBMs of Na and lactose at the ≥20 mL pumped MOM volume time point. These findings document both delayed SA in this population and the lack of association of MBMs with two commonly used clinical indicators of SA, maternal perception and pumped volume.
Henderson et al. 31 studied SA over the first 10 days postpartum in 50 mothers who had received antenatal betamethasone treatment and then delivered preterm infants (<34 weeks of GA). Daily data collection included the following: MBM lactose and citrate concentrations, participant-weighed daily MOM volume, and frequency and duration of pumping sessions. SA was defined as trends of increase in both 24-hour pumped MOM volume and in MOM lactose and citrate concentrations. For mothers delivering infants ≥28 weeks of GA (n = 37), significant increases (p = 0.017) in 24-hour pumped MOM volume were noted between days 1 and 3 postpartum. In contrast, for those delivering <28 weeks of GA (n = 13), pumped MOM volume did not increase significantly until day 4 postpartum.
Furthermore, mean lactose concentrations were higher in MOM of mothers of higher GA infants during the first 3 days postpartum (p < 0.001). These results indicate delayed SA in mothers who delivered <28 weeks of GA.
MBMs are associated with pumped MOM volume
Five publications reported an association between WNL status of MBMs and pumped MOM volume.18,19,29–31 Cregan et al. 29 reported a dose–response relationship between the number of MBMs WNL on day 5 postpartum and pumped MOM volume, with four WNL MBMs associated with the highest volume and no WNL MBMs with the lowest. Similarly, Hoban et al. 30 2018 demonstrated a dose–response relationship between number of WNL MBMs and pumped MOM volume on days 3 and 5 postpartum. In addition, all mothers who achieved CTV (≥500 mLs/day of pumped milk by day 14 postpartum) had all four MBMs WNL earlier (median 4 days postpartum) than those who did not achieve CTV (median 9 days, plus two mothers who never had four WNL MBMs).
A study of the full Hoban cohort 18 showed that the 33% of mothers who achieved CTV between days 6 and 14 postpartum had lower median Na (11.1 mM versus 17.8 mM, p < 0.01) on day 5 postpartum and were more likely to have day 5 postpartum Na <16 mM (77% versus 33%, p = 0.03), day 3 Na:K ratio ≤1 (75% versus 25%, p = 0.06), and day 5 Na:K ratio ≤0.8 (69% versus 10%, p < 0.01). Other collected MBMs (citrate, lactose, total protein) were not associated with CTV achievement.
Henderson et al. 31 (n = 42) also reported a significant positive association with daily lactose (p < 0.001) and citrate concentrations (p < 0.001) and pumped MOM volume over the first 10 days postpartum. 31 This positive association held true for different GAs, despite the statistically significant differences in mean daily pumped MOM volume for the two groups.
In Parker et al., 19 mothers of VLBW infants with WNL concentrations for both Na and lactose (n = 29/69, 42%) had greater daily pumped MOM volume during the first postpartum week as well as greater weekly volumes during the first 6 weeks postpartum than did mothers without WNL concentrations for both Na and lactose (n = 21). Mothers with only WNL Na (n = 38/69) had greater mean and median pumped MOM volume than those without WNL Na (n = 31) at all time points, but only reached statistical significance on day 28 postpartum (355 mL ±406 versus 189 mL ±216, p = 0.036).
A limitation of this study is that MBMs were collected only one time, based on the study-specific clinical definition of SA (achieving ≥20 mL of pumped MOM volume for two consecutive pumping sessions). Because MBMs vary over time in this early postpartum period, it is possible that achievement of SA based on WNL MBM status was not detected at one time point. Similarly, seven otherwise eligible mothers were excluded from study enrollment because they never removed 20 mL for two consecutive pump sessions, likely underrepresenting the relationship between MBMs and low pumped MOM volume. Despite these limitations, study findings support a relationship between WNL MBMs and pumped MOM volume.
Achievement of SA defined by MBMs is associated with pumping frequency
Hoban et al. 30 demonstrated statistically significant relationships between achievement of SA as measured with MBMs, and CTV and pumping frequency. First, dose–response relationships were noted between the number of WNL MBMs and pumped milk volume. Second, achievement of CTV (n = 8/16) was related to the number of cumulative pumping sessions in the first 5 days postpartum (p < 0.001), and to mean daily pumping frequency (≥5 × /daily, p = 0.03) for the first 14 days postpartum. Finally, Hoban et al. 30 demonstrated for the first time that SA was not necessarily permanent, a finding that was detectable only because of twice-daily serial sampling from birth to day 14 postpartum. Specifically, all mothers with one WNL sample for all primary MBMs (n = 14/16) provided at least one subsequent MOM sample without four WNL MBMs. The occurrence of SA impermanence correlated with decreased pumping frequency.
Similarly, Parker et al. 19 found that mothers with WNL Na and lactose (n = 29/69) pumped more frequently during days 2–5 postpartum than those without WNL MBM (n = 21/69). In addition, those with WNL lactose concentrations (n = 39/69) pumped more frequently during days 2–5 postpartum than those without WNL lactose concentrations (n = 30/69). Likewise, mothers with WNL (n = 38/69) versus not WNL (n = 31/69) Na concentrations pumped more frequently on days 1–5 postpartum. Henderson et al. 31 also reported significant direct associations between pumping ≥6 times daily and concentrations of citrate and lactose.
Delayed and/or impaired achievement of SA defined by MBMs may be exacerbated by maternal comorbidities
Breast pump-dependent mothers of preterm infants are at greater risk than the general population for inflammation-based comorbidities of pregnancy, including obesity, preeclampsia, and diabetes, which appear to negatively impact lactation outcomes in term populations and animal models.21,27,34–36 Only three studies have reported data on maternal comorbidities in the preterm population using MBMs.18,24,31
Henderson et al. 31 reported that mothers of more mature preterm infants (≥28 weeks of GA) who experienced a 3–9-day gap between prenatal betamethasone treatment and delivery had significantly less pumped MOM volume than mothers who experienced a gap of 0–2 days or >10 days, but this gap was not associated with either MBM lactose or citrate concentrations. These investigators also found no association with maternal diabetes (gestational diabetes and type 1 diabetes) and either daily pumped MOM volume or lactose and citrate concentrations. 31
In contrast, two studies from the same cohort of 39 mothers reported significant relationships between maternal prepregnancy BMI (body mass index; weight [kg]/height [m] 2 )18,24,37 and pumped MOM volume, Na concentration, and Na:K ratio. In a multivariate regression model, Hoban et al. 18 reported that decreased Na:K ratio and lower maternal prepregnancy BMI were associated with achievement of CTV, making this the first study using MBMs to suggest a role for maternal overweight and obesity as an additive lactation risk factor in mothers of preterm infants. In a secondary analysis of this Hoban et al.'s 18 data set, Medina Poeliniz et al. 24 compared daily rates of change for pumped MOM volume and MBMs (Na, Na:K ratio) between birth and day 14 postpartum for mothers with prepregnancy BMI <27 kg/m2 (n = 17; mean BMI = 22.1 kg/m2) and BMI ≥27 kg/m2 (n = 22; mean BMI = 36.3 kg/m2).
Using a dichotomous growth model and controlling for pumping frequency, during days 1–7 postpartum, mothers with BMI ≥27 kg/m2 had significantly lower mean rates of increase in pumped MOM volume than did mothers with BMI <27 kg/m2 (33.1 mL/day versus 65.8 mL/day), such that mean pumped MOM volume on day 7 postpartum was 195 mL versus 393 mL, respectively. Mean rates of change in MBMs demonstrated similar trends, with Na concentration and Na:K ratio decreasing significantly more slowly in mothers with BMI ≥27 kg/m2 versus BMI <27 kg/m2. In contrast, between days 8 and 14 postpartum, no within- or between-group changes were noted for either pumped MOM volume or MBMs, indicating that overweight/obese mothers did not “catch up” during the second postpartum week, suggesting impaired versus delayed SA.
There is a lack of consensus about which MBM(S) and analysis techniques should be used in research and practice
Two primary approaches have been used to define SA achievement using MBMs. The original work in this field dates back decades and measured all four primary MBMs, whereas recent studies have measured only Na and Na:K ratio. 21 These differences are noteworthy because decreasing trends in Na and total protein primarily measure closure of the paracellular pathway in the mammary gland, whereas increases in lactose, citrate, and K reflect upregulation of transcellular pathways.20,21 Some MBMs are affected by both upregulation of transcellular and closure of paracellular pathways. 21 This is especially true of lactose, which is secreted by transcellular pathway I, but readily crosses into maternal serum before SA achievement due to patent paracellular pathways. 21 Citrate, which reflects upregulation of transcellular pathway I, is the only MBM that is unaffected by paracellular pathway patency, and has historically been labeled the harbinger of lactogenesis because it typically is the first to be WNL.37,38
In the Hoban et al. 30 2018 pilot study, WNL concentrations for citrate preceded WNL concentrations for Na, similar to Cregan et al.'s 29 findings that citrate concentrations were more likely than either Na or lactose to be WNL on day 5 postpartum. Henderson et al. 31 collected citrate and lactose, but did not report times to achieve WNL. Parker et al. 19 found that WNL concentrations for both lactose and Na predicted pumped MOM volume on days 28 and 42 postpartum, whereas WNL for each MBM separately predicted pumped MOM volume for only one of those days postpartum. Given the separate but complementary biologic role of the individual MBMs, an argument can be made for a dichotomous definition of SA achievement (yes/no) based upon whether all four primary MBMs are WNL.
Recently, researchers have measured only Na and/or Na:K ratio, in part, because these MBMs can now be analyzed with point-of-care technology, which is accurate as inductively coupled plasma optical emission spectrometry, easier to use and less costly, does not involve specimen storage or laboratory analyses, and uses less MOM than analyzing all four primary MBMs.21,39–41 The potential for real-time, actionable data using these point-of-care analyzers is promising. In prediction models of pumped MOM volume and achievement of CTV in breast pump-dependent mothers of preterm infants, Hoban et al. 18 found that Na <16 mM and Na:K ratio <0.8 were significant predictors, whereas lactose, citrate, and total protein concentrations were not. Nonetheless, it remains unanswered as to whether lactose, citrate, and total protein are additive to explaining or predicting SA achievement, especially in vulnerable populations with inflammation-based comorbidities.
Discussion
A major finding of this review is that MBMs hold promise as an objective, accurate, and feasible measure of SA in mothers of preterm infants. Specifically, MBMs confirm previous clinical reports of delayed SA in this population, are associated with both pumped MOM volume and pumping frequency, and may be associated with maternal comorbidities that independently predict delayed and/or impaired SA.
However, our findings also revealed a paucity of studies challenged by small sample sizes, different definitions of SA using MBMs (from “trends of increase” in one biomarker to having all four primary biomarkers WNL), inconsistent sampling (from twice daily to a single time during the first 14 days postpartum), and lack of evidence regarding the incremental impact of common maternal comorbidities. Because MOM reduces the risk of potentially preventable, costly, and handicapping morbidities in this population,3,6,15 strategies to identify and monitor delayed and/or impaired SA using MBMs are a priority research and practice area.
Implications for Research
Addressing fundamental research gaps with a larger sample and state-of-the art methodological approaches
Several of the research gaps noted in this review require a larger sample than any of the single studies cited. It is important that such a study incorporates daily samples of all MBMs, pumped MOM volume (weighed to nearest gram), and pumping behaviors (frequency and duration) that are measured and recorded electronically using smart pump technology as described by Hoban et al. 42 and Medina Poeliniz et al. 43 These methodologies address limitations in previous studies that relied on maternal perceptions of SA and pumping logs based on maternal self-report, which are known sources of error. Similarly, detailed data about maternal risk factors and their management (antenatal bed rest, medications) should be collected.
Priorities within this work are as follows: (1) Elucidating which MBM(s) are important for use in research and practice and (2) determining which individual or combinations of maternal co-morbidities signal additional risk for delayed and/or lack of SA achievement and therefore decreased long-term MOM dose.
Elucidating MBMs for research and practice
In the absence of objective measures to document SA, researchers have most commonly turned to maternal perceptions of milk coming in, a measure that has not been validated concurrently with MBMs in preterm populations. 21 Published and unpublished data suggest that breast pump-dependent mothers of preterm infants, particularly those who are overweight or obese, may be particularly unable to articulate whether MOM has come in. Parker et al. 19 reported that maternal perceptions of milk coming in was not correlated with SA as defined by volume achievement (20 mL × 2 consecutive pump sessions) nor with MBM concentrations.
Similarly, Hoban et al. 18 in their MBM cohort queried mothers about their perceptions of milk coming in, but the mothers frequently asked the data collector to tell them if this had occurred because they did not know (R Hoban, unpublished data). The validation of maternal perceptions of SA, especially in high-risk populations, deserves rigorous study before its use as an accurate measure of SA in research.
Specific research questions elucidating which MBMs include: (1) Citrate: Since citrate reflects upregulation of the milk-making apparatus in the mammary gland and is the only MBM unaffected by paracellular pathway patency, 21 does it predict or identify SA problems in at-risk mothers such as those with multiple comorbidities in a different or more accurate way than other MBMs? (2) Na and Na:K ratio: Is the Na:K ratio clinically and statistically additive to the measurement of Na concentration alone? Point-of-care Na measures are simple to perform, whereas point-of-care Na:K ratio requires two separate measures and a calculation. Therefore, if Na concentration alone is sufficient to identify delayed and/or impaired SA, considerable savings in time and costs could be realized with less opportunity for error.
(3) Lactose: Is lactose measurement redundant if Na concentration is measured? Both Na and lactose concentrations in early lactation are affected primarily by paracellular pathway patency, but Na can be measured at point-of-care, whereas lactose cannot. (4) Impermanent paracellular pathway closure: Which happens first, reversal of SA achievement as measured by MBMs or by decreased pumped MOM volume? This information will be critical to directing timely interventions. (5) What are predictive “cut-off” values that can guide subsequent research and clinical guidelines for mothers of preterm infants? Likely more important than absolute values for Na and Na:K ratio are downward trends, or rates of decrease in these MBMs. Nonetheless, in predictive models, Na <16 mM and Na:K ratio <0.8 on postpartum day 5 predicted the achievement of CTV in mothers of preterm infants in the only study to have measured absolute values. 18 Thus, additional research to validate these values is indicated.
Determining which individual or combinations of maternal comorbidities signal additional risk for delayed and/or impaired achievement of SA and therefore decreased long-term MOM dose
Original clinical and animal studies have focused on suboptimal lactation outcomes in the presence of maternal overweight and obesity.24,27 However, more recent work has focused on a constellation of inflammation-based morbidities termed maternal metabolic risk that suggests a role for disturbed secretory differentiation during pregnancy that manifests as delayed and/or impaired SA.24,36 These morbidities, including overweight/obesity, preeclampsia, and diabetes, are commonplace in mothers of preterm infants and are further complicated by therapies that have been linked to lactation problems in clinical studies. 27
Key questions include the following: (1) Since many mothers of preterm infants have multiple metabolic comorbidities, can they be considered a single risk factor with respect to research and practice, or is this impact incremental or specific to a single primary morbidity? These data will be key to determining sample sizes in subsequent research focused on identification and management of maternal risk factors in this population. (2) Are all 4 primary MBM measurements necessary to identify and manage lactation risk in this population compared with mothers of preterm infants without these complications (e.g., are citrate and lactose additive to Na)? (3) Does infant GA (and therefore degree of maternal pregnancy-induced breast development) at delivery affect achievement of SA?
Although this review was limited to mothers of preterm infants, future studies should include breast pump-dependent mothers of other NICU infants, such as those born late preterm, who, although at lower risk of poor outcome, represent a much larger proportion of births and still reap the benefits of maximal doses of MOM.
Translational research to inform best practices for the clinical use of MBMs
A second research priority is designing and conducting studies that translate the science of MBMs into routine NICU clinical practice, similar to studies of other lactation research technologies that have become standard of care, including test-weights, creamatocrit measures, and breast pump technologies. 44
Not to be confused with quality improvement (QI) initiatives, these studies require rigorous original research and should target several key questions: (1) Are MBMs needed? Many will argue that maternal perception of SA is sufficiently robust and that MBMs are not needed. This is a legitimate question that can be easily answered in clinical studies using designs similar to those done with test-weights.45,46 (2) Can mothers perform MBM measurements on their own pumped MOM? Blinded studies using methodologies in Hurst et al. 47 (test-weights) and Griffin et al. 48 (creamatocrit) can answer this question. (3) What are mother's perceptions of performing and using such measures, balancing potential empowerment versus stress in a vulnerable population? A pilot study by Hoban et al. (CIHR trial ID: 202209PJM-490173) will enroll mothers of preterm infants to perform point-of-care MOM Na testing in the NICU to begin to answer this question.
(4) What is the cost and cost-effectiveness of integrating MBMs into routine clinical practice? Does this strategy increase available MOM and decrease costs of donor human milk acquisition, thus improving health outcomes and lowering NICU costs for recipient infants?
Implications for Clinical Practice
MBMs hold the potential to optimize personalized breast pump strategies for mothers of preterm infants during the early critical window postpartum when intervention strategies are likely to be most effective in achieving adequate long-term MOM provision. Current practice is often a “one-size-fits-all” approach with standardized recommendations, including the number of daily pump sessions and frequency of lactation consultations, and the use of pumped MOM volume as the indicator of “progress.” 15 This strategy is inconsistent with the data from this review as well as more recent findings from Hoban et al. 30 and Medina Poeliniz et al., 24 all of which show tremendous variability in the timing and permanence of SA achievement, and therefore, the need for personalized, data-driven breast pumping interventions.
Ideally, these interventions can be guided by real-time, point-of-care Na or Na:K ratios and shared with mothers so that they become involved and empowered, similar to the Griffin et al.'s 48 study in which mothers performed creamatocrits on their pumped MOM to customize calories for their infants. The predictive potential of MBMs to determine by days 3 or 5 postpartum whether an individual mother is likely to have challenges with SA, before it is clinically apparent by pumped MOM volumes, could have significant clinical implications for targeted lactation interventions.
MBMs also add a measure of objectivity to a myriad of QI initiatives in the NICU. Nearly all NICUs benchmark receipt of MOM at NICU discharge, and all evidence points to the critical nature of the first 14 days postpartum in achieving this outcome.17,24,49 Although the introduction of MBMs into the clinical setting may be worthy of its own QI project (e.g., acceptance by mothers and staff, resource allocation, added value), the primary value of MBMs may be as early outcome measures for QI projects that test optimal breast pumping behaviors and/or need-based lactation interventions.
Conclusion
This integrative review reveals tremendous research and practice potential for the use of MBMs to monitor and document achievement or lack of achievement of SA in breast pump-dependent mothers of preterm infants. Two overarching priorities for research are as follows: (1) conducting studies with adequate sample sizes to determine which specific MBMs should be measured and analyzed, and whether specific or additional MBMs are needed to monitor and document SA among mothers with multiple coexisting morbidities; and (2) implementation studies to tease out utility of MBMs, acceptance by NICU mothers, and whether the applications are cost-effective. For practice, MBMs are likely an additional tool to personalize lactation care in this vulnerable population, and should be included in NICU-based QI initiatives.
Footnotes
Acknowledgments
The authors thank the health care workers and mothers in our NICUs.
Authors' Contributions
Conceptualization/design: L.A.P., R.H., M.M.B., C.M.P., T.J., and P.P.M. Supervision: L.A.P., R.H., and P.P.M. Data curation: L.A.P., R.H., M.M.B., and P.P.M. Writing—original draft: LA.P., R.H., M.M.B., and P.P.M. Writing—review and editing: L.A.P., R.H., M.M.B., C.M.P., T.J., and P.P.M. All authors have read and agreed to the published version of the article.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure Statement
No competing financial interests exist.
Funding Information
Partially supported by the Canadian Institutes of Health Research (202209PJM to R.H.) and the National Institutes of Health (1K23NR020537-01A1 to M.M.B.).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.