
Abstract
Objective:
The aim of this study is to examine in-hospital exclusive breastfeeding (EBF) and its association with sociodemographic factors, medical factors, breastfeeding intentions, and health care system breastfeeding support.
Materials and Methods:
We conducted a retrospective cross-sectional study using medical records from 2015 to 2019 of healthy term infants without breastfeeding contraindications at a public teaching hospital serving a racially and ethnically diverse patient population. Using multivariable regression analysis, we examined the associations between in-hospital EBF and sociodemographic factors, medical factors, breastfeeding intentions, and health care system breastfeeding support (in-hospital breastfeeding education and lactation support).
Results:
The prevalence of in-hospital EBF was 29.0%. The statistically significant findings from our fully adjusted regression analysis include that there was a higher prevalence of in-hospital EBF among adult mothers (prevalence ratio [PR]: range 1.78–1.96), married mothers (PR: 1.35, 95% confidence interval [CI]: 1.23–1.44), and mothers who were White (PR: 1.41, 95% CI: 1.20–1.66, compared with Black). Factors associated with a lower prevalence of in-hospital EBF were maternal diabetes (PR: 0.82, 95% CI: 0.70–0.95), pre-eclampsia/eclampsia (PR: 0.82, 95% CI: 0.71–0.95), cesarean delivery (PR: 0.84, 95% CI: 0.77–0.92), neonatal hypoglycemia (PR: 0.46, 95% CI: 0.36–0.59), and intention in the prenatal period to formula feed only (PR: 0.15, 95% CI: 0.10–0.22). In-hospital lactation support was associated with higher prevalence of in-hospital EBF (PR: 1.24, 95% CI: 1.16–1.33).
Conclusions:
Prioritizing lactation support for Black mothers, adolescent mothers, those intending in the prenatal period to formula feed only, and mother–infant dyads with certain medical factors could improve in-hospital EBF.
Introduction
An estimated 19.2% of breastfed infants were supplemented with infant formula within the first 2 days of life in 2019. 1 This is despite recommendations for exclusive breastfeeding (EBF) for the first 6 months of life from several global and national authorities based on evidence of its benefits.2–4 Breastfeeding reduces the risk of adverse health conditions across the life course for both the mother and child.5–7 This includes reduced risk of hypertension, type 2 diabetes, breast cancer, and ovarian cancer for the mother later in life.5,6
For the child, this includes reduced risk of sudden infant death syndrome and various infections and possible reductions in overweight and diabetes later in life.6,7 There is a dose–response relationship between breastfeeding (including both exclusivity and duration of breastfeeding) and reduction of health risks. 6 Early EBF is important for establishing a breast milk supply needed for longer durations of breastfeeding. 8
Furthermore, in 2019, 23.0% of breastfed non-Hispanic Black (Black) infants and 21.0% of Hispanic infants were supplemented with infant formula within the first 2 days of life, compared with 16.1% of non-Hispanic White (White) infants. 1 Yet, early EBF could reduce specific racial/ethnic health inequities. Improved EBF in Black and Hispanic women and children may result in decreased risks in these groups for diabetes and hypertension (for women) and overweight and obesity (for children).5,6
Medical factors and breastfeeding intentions are associated with breastfeeding outcomes. Cesarean deliveries, maternal diabetes, and maternal hypertension are associated with lower EBF.9–11 For example, a U.S. study using data from the Pregnancy Risk Assessment Monitoring System found that mothers with gestational diabetes were less likely to engage in EBF while in the hospital; however, the study was unable to control for breastfeeding intentions, a potential confounder, due to the unavailability of this information. 10 Infant medical conditions are also reported to be associated with EBF.
One study found that neonatal hyperbilirubinemia was negatively associated with EBF prevalence 1 month after birth 12 and another study did not find a statistically significant association at 1 week following birth. 13 However, these studies that examined the relationship between neonatal hyperbilirubinemia and EBF were conducted outside the U.S. and did not specifically examine in-hospital EBF. A study conducted among Latina mothers in North Carolina found that the decision in the prenatal period about the feeding method was a significant factor associated with in-hospital EBF. 14
Health care system breastfeeding support is a critical factor during the early postpartum period. 15 Before beginning the research presented here, we conducted a formative qualitative research study of facilitators of and barriers to in-hospital EBF at the Grady Memorial Hospital (GMH), a public teaching hospital serving a racially and ethnically diverse patient population. 16 GMH achieved the Baby-Friendly Hospital designation in 2015 (a designation that includes implementation of evidenced-based policies and practices that support breastfeeding). 15 GMH administrators sought to utilize the findings from our qualitative study to guide a quantitative examination of factors associated with in-hospital EBF. 16
There is evidence that sociodemographic factors, medical factors, breastfeeding intentions, and breastfeeding support are associated with breastfeeding outcomes. However, the few studies that examined the relationship with in-hospital EBF were conducted outside the U.S. or were conducted in U.S. populations with few people from racial/ethnic minority groups.9,11–13
We therefore aimed to address these gaps in the literature and examined in-hospital EBF and its association with sociodemographic factors, medical factors, breastfeeding intentions, and breastfeeding support in a racially and ethnically diverse patient population.
Materials and Methods
Study population
We conducted a retrospective cross-sectional study using medical records of live births at GMH between January 1, 2015, and December 31, 2019. Approval was obtained from Emory University's Institutional Review Board and GMH's Research Oversight Committee. We obtained the data from the Grady Obstetric and Gynecological Outcomes (GOGO) initiative. The GOGO initiative provided a data set that excluded births that fell under the exclusion criteria, which included medical contraindications for breastfeeding, as defined by the Academy of Breastfeeding Medicine. 17
Additional exclusion criteria were mothers with multiples; infants of less than 37 weeks' gestation; infants who were admitted to the neonatal intensive care unit or who were administered parenteral nutrition during the hospital stay following birth; length of stay exceeding 7 days following birth; and patients transferred to another hospital.
Outcome
In-hospital EBF from 2015 to 2019 was the outcome of interest. We utilized the Joint Commission's definition of perinatal care outcome, PC-05: Exclusive Breast Milk Feeding, to operationalize the outcome, which is defined as receiving only breast milk (including direct breastfeeding and expressed breast milk feeding) and no other fluids or foods except medications, vitamins, or minerals. 18
Independent variables
We utilized the results from our GMH qualitative study to guide the selection of independent variables. We analyzed five categories of independent variables: sociodemographic factors, maternal medical factors, infant medical factors, prenatal feeding intentions, and health care system breastfeeding support. Sociodemographic factors included maternal age, parity, race/ethnicity (non-Hispanic Asian, non-Hispanic Black or African American, non-Hispanic White, Hispanic, and other), language, marital status, employment, number of prenatal care visits, prenatal care clinic (no prenatal care, GMH clinic, or outlying clinic), birth hospitalization length of stay, and infant sex.
The prevalence of EBF among Black mothers was used as the reference standard to avoid the perception of normalizing breastfeeding in White mothers as the standard for comparison. Maternal medical factors examined were pre-existing or unspecified diabetes, gestational diabetes, pre-existing hypertension, gestational hypertension, pre-eclampsia/eclampsia, and cesarean delivery.
Infant medical factors included gestational age (early term or 37–38 weeks, full term or 39–40 weeks, late term or 41 weeks, and post-term or ≥42 weeks), low birth weight (<2,500 g), hypoglycemia, and jaundice. Prenatal feeding intentions included four levels: EBF, both breastfeeding and formula, formula only, and undecided. Health care system breastfeeding support included in-hospital breastfeeding education after birth and a completed lactation consult from a trained lactation consultant.
Covariates
Infant length of stay following birth (range = 1–7 days) and birth year were determined to be a priori covariates, and we adjusted all models for these two variables.
Analytic data set and statistical analyses
A total of 8,971 mother–infant dyads met the study criteria (Fig. 1). Mother–infant dyads were excluded from the analysis if data were missing, which included the following variables: parity (n = 28), race/ethnicity (n = 1), infant sex (n = 1), and low birth weight (n = 43). Three mother–infant dyads had implausible values for gestational age and were excluded.
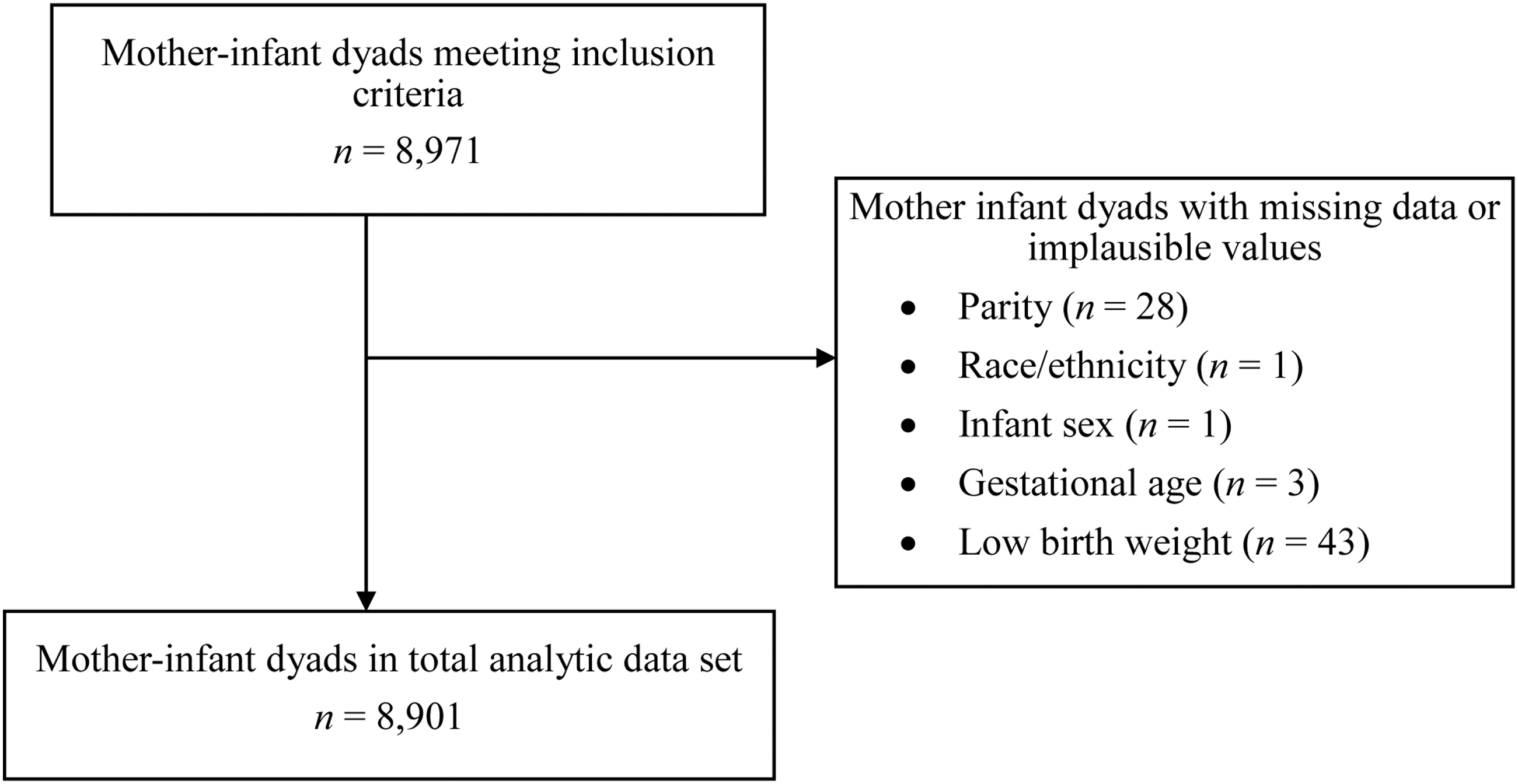
Flow diagram of the data set used in the analysis. Some mother–infant dyads had missing data on more than one variable.
Six mother–infant dyads had missing data on more than one variable, and a total of 70 dyads were excluded due to missing data, resulting in a final analytic data set of 8,901. The EBF prevalence for those with missing data was 31.9%, whereas the EBF prevalence for dyads without missing data was 29.0%; however, the difference in EBF prevalence was not statistically significant (chi-square p-value = 0.6; data not shown).
We conducted descriptive analyses to report the count and frequency of each factor. We also conducted descriptive analyses to report the total in-hospital EBF prevalence stratified by year and race/ethnicity. We conducted Poisson regression with robust variance estimates to determine prevalence ratios (PRs) of in-hospital EBF using two sets of models. The first model set included each individual factor, adjusted for infant length of stay following birth and birth year. The second model was the same as the first model, additionally adjusted for statistically significant factors found in the first model set.
We conducted a sensitivity analysis to examine if the PRs from the second model would differ if those who had prenatal intentions to formula feed only were excluded from the analysis. We examined effect measure modification terms for statistically significant demographic factors and breastfeeding intentions from the second model with breastfeeding support factors by including all the effect measure modification terms in the model and eliminating the term with the highest p-value in the subsequent models.
None of the effect measure modification terms were statistically significant, and none were included in further analyses. We found no evidence of multicollinearity in the models. We used SAS 9.4 (SAS Institute, Inc., Cary, NC) for all analyses. Statistical significance was set at p < 0.05.
Results
The sociodemographic factors, medical factors, breastfeeding intentions, and health care system breastfeeding support for mother–infant dyads in the study are reported in Table 1. Among the mothers in the study, 34.8% were 18–24 years old, 67.3% were multiparous, 67.9% were non-Hispanic Black or African American (Black), 76.8% were not married, and 41.7% were not employed. The in-hospital mean EBF prevalence for GMH for all years from 2015 to 2019 was 29% and ranged from 25% in 2016 to 33% in 2019 (Supplementary Fig. S1).
Sociodemographic Factors, Medical Factors, Prenatal Feeding Intentions, and Health Care System Breastfeeding Support Among Mother–Infant Dyads at Grady Memorial Hospital, 2015–2019
EBF, exclusive breastfeeding; GMH, Grady Memorial Hospital.
Of the exposure variables in the models adjusted for birth year and infant length of stay (model set 1), only parity, prenatal care visits, infant sex, gestational hypertension, jaundice, and in-hospital breastfeeding education were not significantly associated with in-hospital EBF (Table 2). In model set 1, non-Hispanic White (White), Hispanic, and non-Hispanic Asian (Asian) mothers were more likely to breastfeed than Black mothers (PR: 1.74, 95% confidence interval [CI]: 1.48–2.04; PR: 1.07, 95% CI: 1.00–1.15; and PR: 1.22, 95% CI: 1.01–1.47, respectively).
Sociodemographic Factors, Medical Factors, Prenatal Feeding Intentions, and Health Care System Breastfeeding Support Associated with In-Hospital Exclusive Breastfeeding Among Mother–Infant Dyads at Grady Memorial Hospital, 2015–2019
Statistically significant results for comparisons within variables are shown in bold.
Adjusted for infant length of stay and birth year.
Adjusted for infant length of stay, birth year, and all other statistically significant factors from model set 1.
Adjusted for birth year only.
CI, confidence interval; PR, prevalence ratio.
In model set 2, which was additionally adjusted for all other significant factors from model set 1, mothers over 18 years of age (PR range: 1.78–1.96) and mothers who were married (compared with unmarried, PR: 1.35, 95% CI: 1.25–1.45) were more likely to engage in EBF. White mothers were more likely to engage in EBF compared with Black mothers (PR: 1.41, 95% CI: 1.20–1.66).
Mothers with diabetes (PR: 0.82, 95% CI: 0.70–0.95), pre-existing hypertension (PR: 0.82, 95% CI: 0.70–0.96), and pre-eclampsia/eclampsia (PR: 0.82, 95% CI: 0.71–0.95) were less likely to engage in EBF compared with mothers without these medical factors. Mothers who delivered through cesarean were less likely to engage in EBF compared with mothers who delivered vaginally (PR: 0.84, 95% CI: 0.77–0.92). Infants with hypoglycemia were less likely to engage in EBF compared with infants without hypoglycemia (PR: 0.46, 95% CI: 0.36–0.59).
Mothers were less likely to engage in EBF if they indicated that they intended to both breastfeed and formula feed, only formula feed, or were undecided (PR: 0.55, 95% CI: 0.49–0.62; PR: 0.15, 95% CI: 0.10–0.22; and PR: 0.74, 95% CI: 0.70–0.79, respectively) compared with mothers who indicated that they intended to EBF. Mother–infant dyads who received a lactation consult completed by a trained lactation professional were more likely to engage in EBF compared with mother–infant dyads who did not receive a lactation consult (PR: 1.24, 95% CI: 1.16–1.33).
The sensitivity analysis that excluded those with prenatal intentions to formula feed only yielded similar results (Supplementary Table S1).
Discussion
In this study of factors associated with in-hospital EBF at a public teaching hospital serving a racially and ethnically diverse patient population, we found that the EBF prevalence was on average 29.0% from 2015 to 2019. The strongest associations with in-hospital EBF were maternal age, breastfeeding intentions, and neonatal hypoglycemia. In addition, breastfeeding support from a lactation consultant was positively and significantly associated with in-hospital EBF. These results are similar to previously conducted studies that examined factors associated with breastfeeding outcomes.9,11–13 Our study adds to this existing literature by examining the association between these factors and in-hospital EBF.
Other studies have similarly found that the maternal factors, diabetes, hypertension, and cesarean delivery, are significantly associated with lower prevalence of EBF.9–11 These maternal conditions are reported to interfere with lactogenesis II (copious breast milk production).19–21
However, we found in our qualitative study at GMH that obstetricians have limited time to provide prenatal breastfeeding education during prenatal visits to high-risk mothers with conditions such as diabetes and hypertension, which could affect infant feeding decisions for these mothers. 16 The key facilitators of in-hospital EBF at GMH reported by mothers were an individualized approach to breastfeeding counseling and a personable breastfeeding counselor. 16
Neonatal hypoglycemia was negatively associated with in-hospital EBF. Untreated neonatal hypoglycemia can result in further adverse health consequences such as brain damage or death. 22 Clinical recommendations for treating hypoglycemia often include practices that protect EBF, such as supporting breastfeeding and mother's milk expression to provide to infants requiring more frequent feedings.23,24
In addition, an increasing amount of evidence supports the use of glucose gels to treat low-glucose levels, which can prevent formula supplementation. 22 Neonatal hypoglycemia and hyperbilirubinemia are potential consequences of breastfeeding difficulties. Therefore, there is potentially reverse causality between these conditions and in-hospital EBF prevalence; however, we are not able to establish the direction of this relationship due to the cross-sectional study design.
In our study, over half of the mothers were undecided about their infant feeding plans during the prenatal period. A study conducted among Latina mothers in North Carolina after delivery reported that 60% chose to exclusively breastfeed, 37% chose both breastfeeding and formula feeding, and 3% reported to formula feed only. 14
Our study's finding of over half of the mothers being undecided is potentially due to the timing of data collection during the prenatal period, whereas the previously conducted study collected data on infant feeding decisions during the postpartum period. The previously conducted study also found that the decision about the feeding method before pregnancy was significantly associated with in-hospital EBF. 14 These findings suggest that efforts that aim to address breastfeeding decisions may be most effective if delivered early in the decision-making process. 14
Other studies have recently reported that lactation support from professionals trained to assess the breastfeeding relationship between the mother and infant and to provide support for effective latch, breast milk transfer, and concerns about breast milk supply is associated with breastfeeding duration and exclusivity as early as 3 months, including among high-risk patients with conditions such as gestational diabetes.25,26
Our study further adds to these findings, and we found that mother–infant dyads who received breastfeeding support from a lactation consultant while in the hospital following birth were more likely to engage in EBF compared with those who did not. Our qualitative study also found that practical support with breastfeeding was a key facilitator of in-hospital EBF; however, we also found that there was inadequate staffing to provide lactation management support. 16 Increased lactation support from trained professionals could potentially improve in-hospital EBF.16,25,26
Our study has three limitations. First, we analyzed data from a single public teaching hospital with ∼3,000 births per year, serving a high proportion of Black socioeconomically disadvantaged patients. The results may not be generalizable to hospitals that do not have similar characteristics. However, other hospitals could use our study as a framework to understand setting-specific factors associated with in-hospital EBF and thereby support their quality improvement efforts.
Second, we were unable to examine all factors that may influence in-hospital EBF. Some data were not in fields with predefined categories, but instead in notes, and the volume of births was too high to make it possible to extract these data efficiently.
These factors include prenatal breastfeeding education, skin-to-skin contact, early initiation of breastfeeding, rooming-in, and timing of the receipt of lactation consults (e.g., first day of life compared with the second day of life); birth country; social support; participation in the Special Supplemental Nutrition Program for Women, Infants, and Children; and maternal obesity.16,23 Researchers examining in-hospital EBF could prospectively collect the data from medical records to be able to efficiently extract this information.
Third, this is a cross-sectional retrospective study, and causation cannot be established with this study design.
Conclusions
In-hospital EBF during the hospital stay following birth was low in this urban hospital and varied by sociodemographic characteristics, health status of the infant and mother, prenatal breastfeeding intentions, and in-hospital breastfeeding support. This information can be used by the hospital to guide decisions about quality improvement efforts to enhance breastfeeding support.
Adolescent mothers, those intending in the prenatal period to formula feed only, and infants with neonatal hypoglycemia could be prioritized to improve in-hospital EBF. In-hospital breastfeeding support from trained lactation professionals following delivery may be key to improving in-hospital EBF among these priority populations.
Footnotes
Acknowledgments
The authors thank Dr. Sheree Boulet and Sallie Owens for their guidance with data collection through the GOGO initiative. The authors thank Dr. Franklyn Geary for his guidance.
Authors' Contributions
L.H.B. was involved in conceptualization, methodology, formal analysis, data curation, writing—original draft, writing—reviewing and editing, visualization, and project administration. E.H.A. was involved in conceptualization, methodology, and writing—reviewing and editing. D.J.J. was involved in conceptualization, methodology, resources, and writing—reviewing and editing. M.R.K., C.G.P., and U.R. were involved in conceptualization, methodology, writing—reviewing and editing, and funding acquisition. N.W. was involved in conceptualization, investigation, resources, and writing—reviewing and editing. M.F.Y. was involved in conceptualization, methodology, data curation, writing—reviewing and editing, supervision, project administration, and funding acquisition.
Disclaimer
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was financially supported by the National Association of County and City Health Officials to support the Reducing Disparities in Breastfeeding through Continuity of Care Project through funding from the Centers for Disease Control and Prevention, award number 18NU38OTOOO306. This study was also financially supported by the Emory Maternal and Child Health Center of Excellence, with support from the Health Resources and Services Administration Maternal and Child Health Bureau under award T76MC28446.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.