
Abstract
Background:
Cow's milk protein allergy (CMPA) is well described in term infants, as opposed to preterm infants. In preterm infants, CMPA shares many gastrointestinal symptoms with necrotizing enterocolitis (NEC).
Objectives:
To evaluate the presentation of CMPA in preterm infants and to investigate the different diagnostic and therapeutic options.
Materials and Methods:
We searched for the relevant literature using the medical databases PubMed, Web of Science, and the Cochrane Library. We performed a post hoc analysis on the 25 case reports included in this study.
Results:
Literature was scarce and heterogeneous. The majority of preterm infants with CMPA were exposed to bovine-based milk proteins before the development of symptoms. The most common clinical manifestations were bloody stools, vomiting, and abdominal distension. Of the 25 cases, only 7 (28%) retained human milk in their diet after diagnosis. In the larger studies, no study has human milk as primary feeding choice after diagnosis.
Conclusions:
Preterm infants exposed to a type of cow's milk-based formula in their first days of life have a higher risk of developing CMPA. Most of the preterm infants are no longer fed with human milk after the diagnosis of CMPA is made, which is in contrast with current nutrition guidelines in preterm infants. We strongly advocate that human milk with mothers on a cow's milk-free diet is the first choice of feed after the diagnosis of CMPA. Prospective studies are necessary to obtain more information regarding clinical presentation, diagnostic tools, and therapeutic approaches.
Introduction
Human milk provides the optimal nourishment for the preterm infant and is therefore the recommended feeding for preterm infants.1,2 In addition, it needs to be considered as part of the therapeutic strategies to decrease preterm infants' mortality and morbidities. After all, the use of mother's own milk results in a significant lower incidence of necrotizing enterocolitis (NEC), sepsis, bronchopulmonary dysplasia (BPD), and retinopathy in prematurity. 3 Human milk supports the development of the host defense of the preterm infant. Furthermore, clinical feeding tolerance is improved, and full enteral nutrition is obtained more quickly when fed with human milk. Finally, the neurodevelopmental outcomes are better when the preterm infant is on a predominantly human milk diet. 1
Due to the high protein need for fetal growth and to prevent extrauterine growth restriction, the use of human milk fortifier (HMF) that supplements human milk is essential in preterm infants. The most commonly used form of fortification is bovine-based milk fortifier. Human milk-derived fortification is now also available, although it is preliminary and expensive.4,5
Nonetheless, providing human milk for a preterm infant can be a challenge sometimes. 1 When mother's own milk is unavailable or there is an insufficient supply of mother's own milk, then donor human milk or preterm formulas can be used as alternative options. A Cochrane review compared the use of donor human milk versus preterm formula for feeding preterm infants. It demonstrated that preterm formula was associated with higher rates of weight gain and growth. However, it also showed that preterm formula is associated with a higher risk of severe NEC. 6 Therefore, several guidelines stress the importance of mother's own milk being superior to formula for preterm infants.7,8
Cow's milk protein allergy (CMPA) is an immunological reaction against proteins found in cow's milk. Cow's milk contains multiple proteins such as casein and whey. 9 CMPA is the most common food allergy in infancy, and can be IgE mediated or non-IgE mediated.10,11 IgE-mediated CMPA gives an immediate allergic reaction, while the non-IgE pathway leads to a postponed response with mainly gastrointestinal symptoms. 12 CMPA and allergic proctocolitis at this age are predominantly non-IgE mediated. 13 There are some diagnostic criteria for CMPA. First, elimination of cow's milk protein should provide resolution of symptoms. In addition, symptoms may recur if cow's milk protein is reintroduced into the diet. Finally, other causes for the symptoms must be ruled out. 10
As opposed to term infants, the prevalence of CMPA in preterm infants is uncertain due to various reasons. First, CMPA has a wide range of symptoms, such as gastrointestinal (rectal blood loss, abdominal distension, vomiting, and feeding intolerance), dermatological, and respiratory (wheezing and respiratory distress).10,14 The gastrointestinal symptoms of CMPA overlap with those of NEC. Therefore, it can be a challenge to distinguish CMPA from NEC. NEC is a life-threatening neonatal condition that causes inflammation of intestinal tissue. 15
This inflammatory bowel disease is one of the most common gastrointestinal emergencies among preterm infants with significant morbidity and mortality. 16 As a result of this, it is often the first working hypothesis for a neonatologist when a preterm infant presents with rectal bleeding, abdominal distension, or feeding intolerance.17–19 Second, there are no significant diagnostic tools for CMPA in preterm infants. The diagnosis of CMPA is generally based on the response to elimination diets and the recurrence of the symptoms when cow's milk protein is reintroduced into the diet.10,18,19
Another issue we encounter is that there are no extensively hydrolyzed milk formulae that are nutritionally adequate for preterm infants. 17
The aim of this study is primarily to investigate the presentation of CMPA in preterm infants, and second to compare the different diagnostic and therapeutic options. In addition, a comparison will be made between CMPA in prematurity and CMPA in term infants.
Materials and Methods
Search method
We searched for the relevant literature using the medical databases PubMed, Web of Science, and the Cochrane Library. Articles published before the date of April 2021 were included. Our initial search terms were “cow's milk protein allergy,” “cow's milk allergy,” “preterm infants,” “premature infants,” “allergic proctocolitis,” “allergic enterocolitis,” “rectal bleeding,” “food protein-induced enterocolitis,” “breastfeeding,” and “preterm formula.” Based on titles and abstracts, we selected the relevant literature, and excluded articles that were irrelevant to the research question. Reference lists of the selected articles were checked to identify additional articles.
An overview of our search strategy is shown in Figure 1. Because of the sparse literature, no additional exclusion criteria were applied, and we expanded our research question to compare CMPA between preterm and term infants.
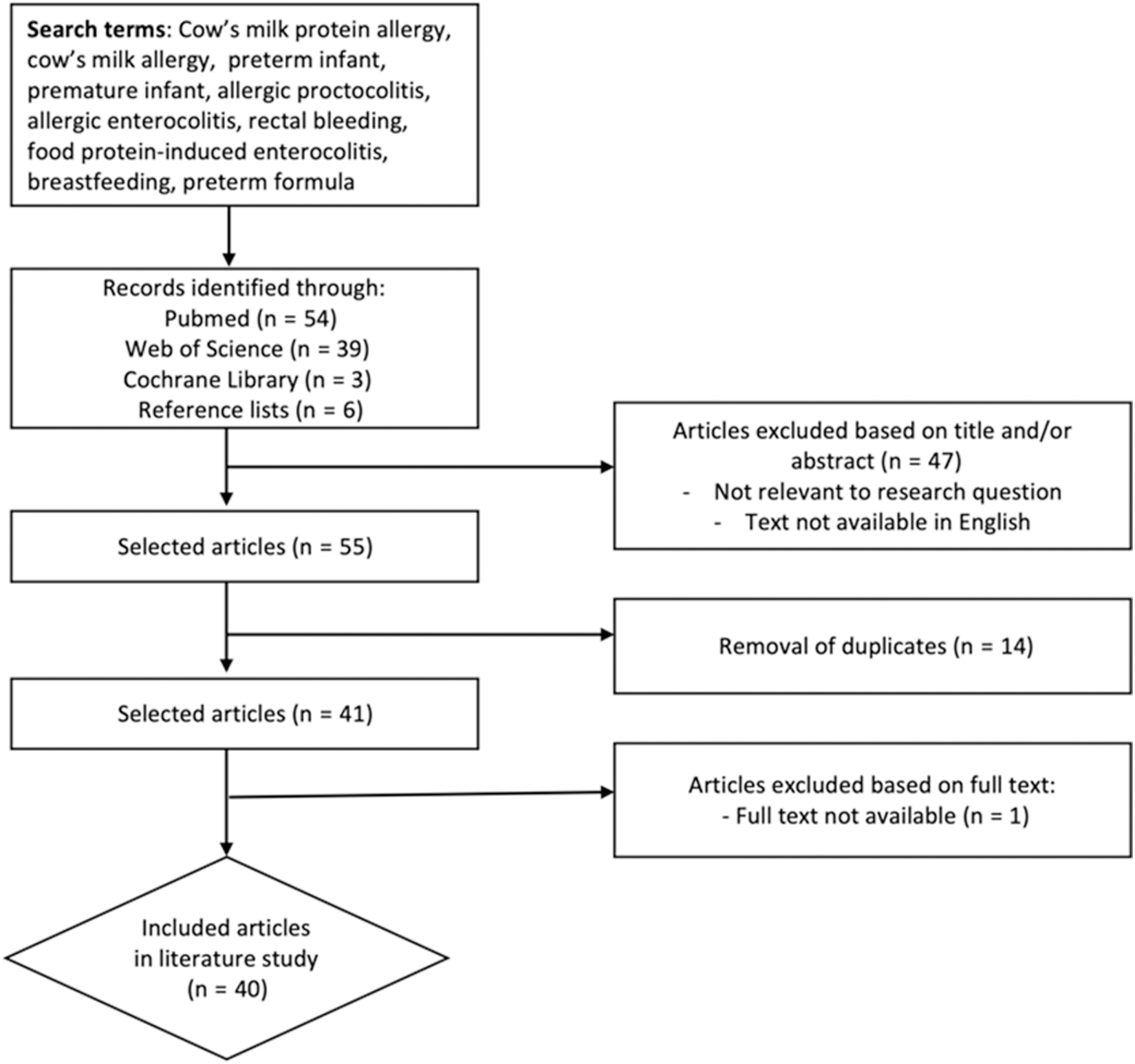
Overview of search strategy.
Post hoc analysis
We performed a post hoc analysis on the 25 case reports included in this study. We obtained a summary of the clinical manifestations, diagnostic tools, and management strategies of CMPA in preterm infants. Certain demographics were excluded in our post hoc analysis because too few case reports provided information regarding these demographics.
Results
Table 1 gives an overview of the studies on CMPA in preterm infants. Table 2 summarizes the case reports. Table 3 provides a post hoc analysis of the case reports.
Overview of Studies on Cow Milk Protein Allergy in Preterm Infants
Overview of Case Reports
DOL, day of life; HMF, human milk fortifier.
Post Hoc Analysis of Case Reports
Although we aimed to search for guidelines about CMPA in preterm infants, the literature was heterogeneous, scarce, and mainly based on retrospective studies and case reports. Overall, the majority of preterm infants who developed CMPA were exposed to bovine-based milk proteins before the development of the symptoms (cow milk protein-based preterm formula or bovine milk-based fortifier). In the studies, the percentage receiving a form of preterm formula based on cow's milk protein ranged from 75 to 100. In the post hoc analysis of the case reports, this percentage was 92.
The most common clinical manifestations of CMPA in preterm infants were bloody stools, vomiting, and abdominal distension (Tables 1 and 3). However, in some cases, respiratory symptoms such as apnea episodes were more prominent than gastrointestinal symptoms.14,17,19–21 Tekgündüz et al. published a case report of a preterm infant with BPD. The patient initially presented with respiratory symptoms, but at day of life (DOL) 80 there were also bloody stools. CMPA was suspected and confirmed with an oral food challenge (OFC): gastrointestinal and respiratory symptoms reoccurred. Thus, it was doubtful if the respiratory symptoms were a result of the BPD and the CMPA diagnosis. 14
Several studies published a case of CMPA that presented as NEC and was treated as (recurrent) NEC.17,19,22–24 Some of these mimicked NEC both clinically and on X-rays.17,18,20 CMPA and NEC have a lot of symptoms in common such as grossly bloody stools, therefore differentiating them can be difficult.17,22 It is not uncommon that CMPA engages in NEC mimicking and is therefore initially treated as NEC, which includes stopping all enteral feeding. Consequently, the symptoms disappear with this approach. However, when restarting enteral nutrition, all symptoms reoccur. 17
In the larger studies on CMPA in preterm infants, not one single study had human milk as the choice of feed after diagnosis (Table 1). Of the 25 cases, only 7 (28%) retained human milk in their diet after diagnosis (Table 3).
Discussion
In this literature study, we aimed to evaluate the presentation of CMPA in preterm infants, and to investigate the different diagnostic and therapeutic options. Although our goal was to search for guidelines about CMPA in preterm infants, we found that there were no good qualitative studies on CMPA in preterm neonates, which is the reason we were obligated to work mainly with case reports in this study.
Nevertheless, it is noteworthy that the majority of the preterm infants who developed CMPA were exposed to bovine-based milk proteins before the development of the symptoms (cow milk protein-based preterm formula or bovine milk-based fortifier). These findings are in line with a clinical trial where term newborn infants at risk of atopy were randomized to receive either exclusive human milk or human milk and cow's milk-based preterm formula in the first three days of life. Infants who exclusively received human milk had a significant decreased risk of developing CMPA, suggesting that sensitization to cow's milk and food allergy, including CMPA and anaphylaxis, is primarily preventable by avoiding cow milk supplementation for at least the first 3 days of life. 25
In addition to the already cited benefits of human milk, this is yet another argument for attempting to feed a preterm infant exclusively with human milk. If mother's own milk does not meet the caloric and nutritional needs of the preterm infant, one may consider using exclusive HMF instead of bovine-derived fortifier. Ananthan et al. compared the use of HMF with bovine milk-derived fortifier (BMF) in a meta-analysis. They concluded that HMF was associated with a lower risk of NEC, but also with poorer weight gain. 26
The incidence of CMPA in preterm neonates remains uncertain due to the lack of large prospective studies and the fact that CMPA is still often unrecognized in preterm infants. 19 Morita et al. cited an incidence of CMPA of 1.1% in their neonatal ward. 27 This percentage is higher than the 0.21% reported in a retrospective multicenter survey of Miyazawa et al. 28 In addition, we found that there is a wide variety in the time to first onset of symptoms (DOL 0–165).
According to Vlieghe et al. and Tekgündüz et al., several factors contribute to the sensitization to cow's milk protein allergens.14,29 An immature immune system and various harmful factors to the intestinal epithelium (free radicals, antibiotics, food restrictions, intestinal ischemia) lead to an increased intestinal permeability. Due to this elevated permeability, there is a sensitization to potential allergic allergens, such as cow's milk protein allergen.14,18,29,30 Various cow milk proteins, such as casein, β-lactoglobulin, lactoferrin, and bovine immunoglobin, can lead to this sensitization. 9 The fact that possible allergic antigens can move across the placenta and reach the amniotic fluid, and that some premature babies with CMPA were exclusively breastfed, suggests that the initial sensitization can already develop in utero.9,31,32
Apart from the fact that NEC and CMPA have several symptoms in common, NEC could play a sensitizing role in the pathogenesis of CMPA. During the healing phase of NEC, proinflammatory β-lactoglobulin, casein-specific interferon-γ, and interleukin-4 increase. Once fully recovered from NEC, there is a considerable decrease of the aforementioned values and an increase of transforming growth factor-β1 (TGF-β1) cells. According to Cordova et al., it is possible that the shift from a proinflammatory phase to an increase in TGF-β1 cells is significant for the tolerance of various food antigens. Hence, the failure of this particular switch could contribute to the pathophysiology of the development of CMPA. 30
Nonetheless, several studies offer a different view on the hypothesis of the pathophysiology. Morita et al. analyzed the differences in manifestations of CMPA between term and preterm infants. In their retrospective study, all preterm infants only established CMPA later than the age of 32 weeks, corrected for gestational age. Hence, their interpretation is that the immune system before 32 weeks is still too immature to establish an autoimmune response such as CMPA and that a certain immunological maturation is necessary to develop CMPA. 27 This is an interesting hypothesis, although we must remember that these observations were made in a small group.
In accordance with the guidelines, the diagnosis of CMPA is solely based on the OFC.9,15,16 Nevertheless, we note that an OFC is only performed in the minority of cases. This is due to the fact that it poses a potential risk of deteriorating the condition of the preterm infant, especially if they had already suffered from another medical condition. Therefore, the diagnosis of CMPA in preterm infants is mainly based on the elimination of cow's milk protein from their diet, rather than by applying the OFC.18,27,28
Twelve percent of the cases reported a positive OFC, 24% a negative OFC, and the remaining 64% did not perform a challenge. However, these percentages of a positive and negative OFC should be interpreted with necessary nuances. The positive challenges were performed 1–2 weeks after eliminating cow's milk protein in their diet, whereas the challenges with a negative result were only performed at the age of 6–18 months.
In various studies, other different diagnostic tools are used to support the diagnosis of CMPA in preterm neonates. Peripheral eosinophilia is occasionally found in preterm infants with CMPA, and is therefore often determined in various cases.13,15,33,34 Manuyakorn et al. describe three cases of preterm infants with CMPA and persistent peripheral eosinophilia, with a normalization or considerable decrease of the eosinophil level in the blood after elimination of cow's milk protein. 19 However, several studies indicate that eosinophilia is a common and nonspecific finding during the first months of life of preterm infants.32,35 It is also linked to infection, NEC, and transfusion of packed cells.19,23,29,36
This does not signify that we cannot incorporate this finding into our decision tree when we consider CMPA and observe eosinophilia, especially when we notice a decrease or normalization of the eosinophilic count after eliminating cow milk protein from the diet.
Dupont et al. performed a retrospective study to investigate the potential of a ready-to-use atopy patch test (APT) as a diagnostic instrument in the diagnosis of CMPA, particularly in the non-IgE–mediated responses. The ready-to-use CM-APT contains a small chamber with powdered defatted milk. Once applied, the powder will dissolve on the skin. The control-APT and CM-APT remain 48 hours on the back of the preterm infant, and the interpretation is done 24 hours later. Fourteen preterm infants were suspected with CMPA, and were therefore switched to an amino acid-based formula.
Four of the preterm infants showed no improvement after this change in formula and were put back on CMP-based formula. Of the remaining 10 preterm neonates, 7 infants had a positive APT. Hence, this study argues that APT can be a noninvasive tool in the diagnosis of CMPA. 13 To conclude, CMPA in preterm infants remains a difficult and main clinical diagnosis. Diagnostic tools to support the diagnosis are scarce and studied to a limited extent. Hence, it is important to consider CMPA especially in case of a preterm with suggestive symptoms not causing critical illness, or in case of a preterm infant with recurrent NEC symptoms after the reintroduction of enteral nutrition.
Preterm infants have higher nutritional and caloric needs than term infants. It is often challenging to meet these needs. With CMPA, there are a lot of additional challenges since the bovine-based milk fortifier cannot be used. 24 As mentioned before, human milk is the best choice of nutrition for premature babies. Therefore, it is striking that human milk almost completely disappears from the nutritional options after CMPA is diagnosed in preterm infants. As mentioned in the results, there is not one study that chooses human milk after the diagnosis. Of the 25 cases, only 7 (28%) retained human milk in their diet after diagnosis (Table 3). This is contradictory to the current guidelines regarding the most nutritionally adequate feed for preterm infants.10,18,19
With the disappearance of human milk in the feed after diagnosis, all the advantages of human milk for the preterm infant automatically disappear as well. We therefore strongly advocate that human milk with mothers on a cow's milk protein-free diet is the first choice of feed after the diagnosis of CMPA, and that further research is moving in that direction. Moreover, it remains doubtful whether extensively hydrolyzed formula (EHF) is nutritionally competent for preterm infants.
A Cochrane systematic review concluded that it requires larger and more pragmatic studies to determine whether EHF is effectively nutritionally (in)adequate as a feed for preterm infants. 2 Zuppa et al. investigated the nutritional efficacy of EHF in preterm infants through a randomized controlled trial. The preterm infants nourished with EHF showed a slower weight evolution than those fed with standard preterm formula. 37 The influence of marketing of commercial milk formula on health professionals and science should also not be underestimated in this light, as recently reported in The Lancet Breastfeeding series. 38
It was noticed that there were three pairs of monozygotic twins who all had CMPA (Table 2). It is known that food allergies have genetic and environmental risk factors. 32 These findings support the fact that CMPA has a genetic constitution.
Morita et al. compared CMPA in term and preterm infants. Their findings were that term and preterm infants have similar types of symptoms. However, there was a significant difference in median age of onset; preterm infants develop these symptoms much later than term infants (23 versus 3.5 days). Based on these findings, their hypothesis of immunological maturation to develop CMPA was substantiated. 27
We are aware that this study has several limitations: we were obligated to work with small heterogeneous studies, which were mostly case reports, and therefore we could only perform a post hoc analysis that automatically inherits bias. Therefore, it is crucial to interpret the analysis with the necessary caution. This made it challenging to compare results and get an overview. However, we believe it is important that this study was conducted: relevant literature on this particular subject was obtained, and diagnostic and therapeutic choices were compared with the known guidelines. The remaining questions and problems were presented, so that directions for further research are clarified.
Therefore, it would be interesting to set up a study that examines the effect of an elimination diet (preferably mother's own milk with mothers on a cow's milk protein-free diet) and evaluate the response. In case of a clinical response, an OFC should be performed after a period of 6 months to get a certain diagnosis.
Conclusions
It is important to be aware that CMPA in preterm infants can occur, and consider the diagnosis of CMPA in preterm infants with gastrointestinal or respiratory symptoms. Because of the aforementioned benefits of human milk, we emphasize the importance of mother's own milk in nutritional policies in preterm infants, even after the diagnosis of CMPA. Prospective and larger homogeneous studies are necessary to investigate the different aspects of CMPA in preterm infants.
Footnotes
Authors' Contributions
A.E. developed the concept of the article and conducted revisions. M.F. conducted the literature review and wrote the article. M.F. and A.E. discussed about the content of the article. All authors read and approved the final article.
Ethical Approval and Consent to Participate
No human or animal applicants were used in this article. This article review does not require an ethical approval.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.