
Abstract
Background and Objective
: Donor human milk (DHM) from the human milk bank (HMB) is the next best alterative in circumstances when mother's own milk is not available. There was a steep decline in the volume of DHM collected during the coronavirus disease-19 (COVID-19) pandemic due to various factors, while DHM demand increased. Hence, a quality improvement (QI) study was conducted to increase the volume of milk donation to HMB from postpandemic baseline of 300–400 to 1,000 mL/day over 8 weeks.
Materials and Methods:
Fish bone analysis was used to identify the potential barriers, and four Plan-Do-Study-Act (PDSA) cycles were conducted from January 2021 to March 2021 to address the key barriers. In the first PDSA cycle, training of health care providers was done. Sessions for educating mothers in the second PDSA cycle and individualized one-to-one counseling of mothers by a mother support group were done in the third PDSA cycle. The availability of breast pump was increased in the fourth PDSA cycle. Sustainability of the interventions was studied for 6 months and data were analyzed.
Results:
The average DHM collected per day at the end of each PDSA cycle was 900, 1,500, 1,000, and 1,100 mL. Although the sustenance phase was affected by the second COVID-19 wave, prompt identification of the issues and timely interventions prevented the donated volume from dropping to preintervention levels.
Conclusion:
QI initiatives customized for local settings can result in significant improvement in voluntary milk donation in HMB, which can result in more availability of DHM to premature babies.
Introduction
Human milk is species specific and the most beneficial nutrition for term as well as preterm infants. Unfortunately, many factors such as delayed lactogenesis, insufficient milk volume in the first few days after delivery, maternal separation due to extramural birth, local breast problems, maternal morbidities, and difficulties in milk expression due to stress or inadequate support may affect adversely or prevent an infant from receiving his or her mother's own milk (MOM) after birth. Under such circumstances when MOM is not available, the next best option is pasteurized donor human milk (PDHM) from the human milk bank (HMB), which provides sufficient nutrients and reduces rates of feed intolerance and necrotizing enterocolitis in very low birth weight infants. 1 Furthermore, the use of PDHM was associated with increased use of MOM, suggesting that the use of donor milk serves as a bridge to promote the use of MOM. 2
The world of human milk banking has been heavily affected by the coronavirus disease-19 (COVID-19) pandemic. Globally, milk donations have decreased and the volume of milk collected at HMBs during this period was remarkably low. 3 Various factors during the pandemic that could have contributed included fewer health care professionals available to maintain the milk bank, various policies adopted by the health care system to decrease the spread of infection such as initial separation of mother–neonate dyad until the screening of mother, early discharge of neonates, and most importantly, lack of information regarding the spread of the virus via human milk. Subsequently, a study by Walker et al. proved that severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) was effectively inactivated by Holder pasteurization, suggesting that PDHM still be a better and safer choice than infant formula whenever available. 4 Furthermore, an observational study by Fox et al. has shown that 95% of milk samples from COVID-19-positive mothers contained anti-SARS-CoV-2 soluble immunoglobulin-A antibodies, which provide protection to the infants. 5
We are a tertiary care hospital in western India with an HMB established in 2005. Similar to the global situation, donations at our HMB decreased during the pandemic from an average of 1,000–1,500 mL/day in the prepandemic era to an average of 300–400 mL/day during the pandemic. In contrast, initial separation of mother and neonate dyad due to COVID-19 restrictions resulted in delayed lactogenesis and therefore an increased demand for PDHM, leading to an increased demand-supply gap. Hence, we planned this quality improvement (QI) study to narrow this gap.
Aim
To increase the donation of human milk to the HMB from a baseline of average 300–400 to 1,000 mL/day over a period of 8 weeks.
Materials and Methods
Setting
The study was conducted in a level III B Neonatal Intensive Care Unit (NICU) of a tertiary referral hospital that caters to more than 2,500 low birth weight infants and 1,600 NICU admissions annually. The volume of DHM collection during the prepandemic was at par with the national median volume of 498 L annually. 6 As there was a substantial decrease in the donation of human milk during the COVID-19 pandemic, we planned this QI study to address the issue.
Study design
This QI is based on the Point of Care Quality Improvement (POCQI) guideline; accordingly, a multidisciplinary QI team was formed consisting of three neonatologists (one team leader and two supervisors), two neonatology fellows, two lactation consultants, and two neonatal nurses for implementing changes.
As per our unit policy, we included healthy lactating mothers whose babies were admitted in our NICU and were willing to donate the surplus expressed breast milk after the feeding requirement of their own babies were met, provided they were HIV, HBsAg, and VDRL negative. We followed HMB guidelines published in 2014 by Indian Academy of Pediatrics. Mothers were excluded if they were on medications that were deemed to be contraindicated for milk donation, including smokers and alcoholics. 7 As our HMB is not for-profit, all the milk obtained from the voluntary donation from mothers was processed and dispensed to the needy infants in the NICU at no cost to the patient. The mothers were not paid for donating the milk.
Three phases were planned for the QI study. The phases were baseline phase, intervention phase, and sustenance phase. The outcome measure was the amount of milk donated to a milk bank over a 24-hour interval.
Baseline phase
During this phase, data on the process were collected from an HMB register retrospectively. Assessment of the baseline data showed that an average of 300–400 mL of donor milk per day was donated over 3 months before the initiation of our study (October–December, 2020). The team conducted a group discussion to analyze the problem and conducted process mapping of the steps involved in milk expression and donation.
Further the team carried out a root-cause analysis using the fish-bone approach (Fig. 1) and identified the various barriers for the donation of human milk.
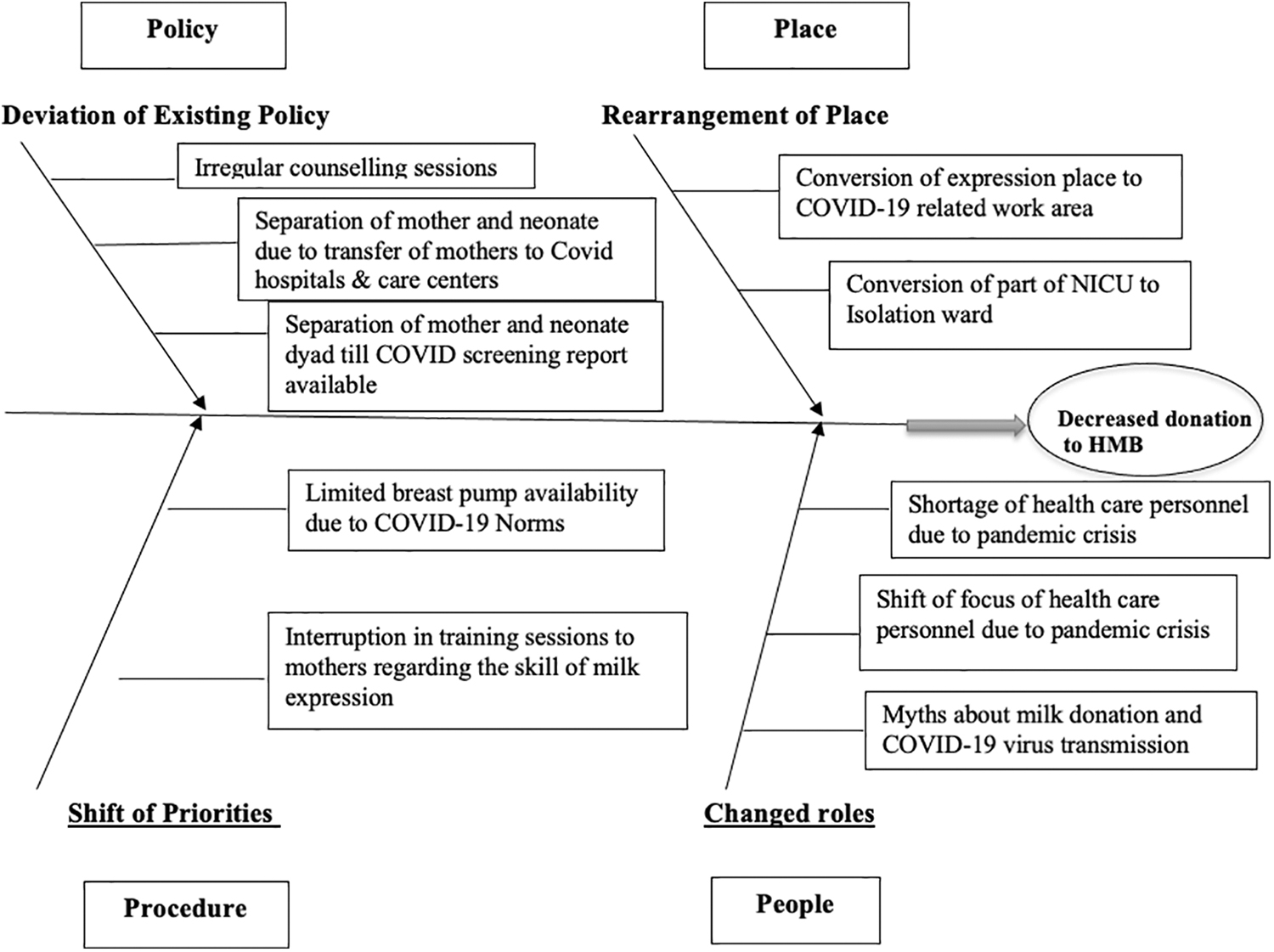
Root cause analysis of low human milk donation.
After extensive brainstorming and multiple focused group discussions with team members, the key barriers contributing to the decrease in milk donation were identified and possible change ideas to overcome them were planned using four Plan-Do-Study-Act (PDSA) cycles. Change ideas were adopted, adapted, or abandoned after the PDSA cycles. The sustainability of the interventions was studied for 6 months after the implementation phase.
Intervention phase
Based on the key barriers identified, four PDSA cycles of 2 weeks each were planned and implemented.
PDSA cycle 1: Training of health care providers
During the COVID-19 pandemic, there was an acute shortage of doctors and nurses in the NICU due to various reasons such as personal isolation for COVID-19 infection, quarantine due to infection exposure, and transfer of NICU doctors and nurses to COVID-19 wards/hospitals across the city. Hence, creating awareness among health care providers (HCPs) about the importance and method of milk donation inadvertently received less priority. In light of the above, education sessions were organized in small batches based on duty timings on the importance and safety of milk donation using seminars and PowerPoint presentations.
PDSA cycle 2: Educating mothers
The COVID-19 pandemic had a negative impact on regular counseling and motivation sessions for milk donation due to the strict need for social distancing, avoidance of large gatherings, and shortage of trained HCPs. In addition to lack of knowledge, several mothers had fear and doubts about milk donation, including transmission of the infection through breast milk. Structured group counseling and interactive sessions of 30 minutes each for 6 days per week were planned. COVID-appropriate behavior was maintained throughout the training sessions. Counseling was done in the form of lectures covering the importance of milk donation, method and frequency of expression, hygienic precautions required during milk expression and collection, and safety of milk donation in local language, and also by demonstration of the method of expressing milk using posters, cards, and a breast model.
PDSA cycle 3: Individualized counseling of mothers by mother support group
Before the COVID-19 pandemic, mothers with difficulty in milk expression or those with poor motivation for milk expression and donation were addressed using daily one-to-one counseling sessions. However, during the pandemic, mainly due to a shortage of HCPs, these sessions were interrupted. Therefore, the team planned to form a support group for mothers, which included lactation consultants who visited thrice a week. The focus was on educating and supporting high-risk mothers, and assisting them individually in the technique of milk expression.
PDSA cycle 4: Increase availability of breast pumps
Even after counseling and demonstration, some mothers continued to have difficulty in expression of milk by hand. A randomized trial has shown that use of a hospital-grade electric breast pump results in greater milk output compared with hand expression. 8 Hence, breast pumps are being used in our HMB for donor milk collection as a routine practice. During the pandemic, there was limitation in space due to reorganization of the NICU to accommodate a COVID-19 NICU. As a result, the area allotted for milk expression with the breast pump facility was no longer available. Hence, the breast pumps were made available in the NICU throughout the day and night.
Sustenance phase
Data on the amount of PDHM donated were recorded for 6 months after the last PDSA cycle to look for the sustenance of the interventions.
Outcome measure
The amount of milk donated to a milk bank over a 24-hour interval.
Data analysis
Data were collected in Microsoft Excel on a daily basis throughout the study and analyzed using run charts. Feedback of the results was given to the team on a weekly basis.
Results
During the first PDSA cycle over 2 weeks, we conducted 6 training sessions to train the team of 12 resident doctors and 25 nurses. The donated milk volume increased to 800–900 mL/day (Fig. 2). As the cycle showed improvement, we continued regular counseling and motivation of HCPs in the NICU.
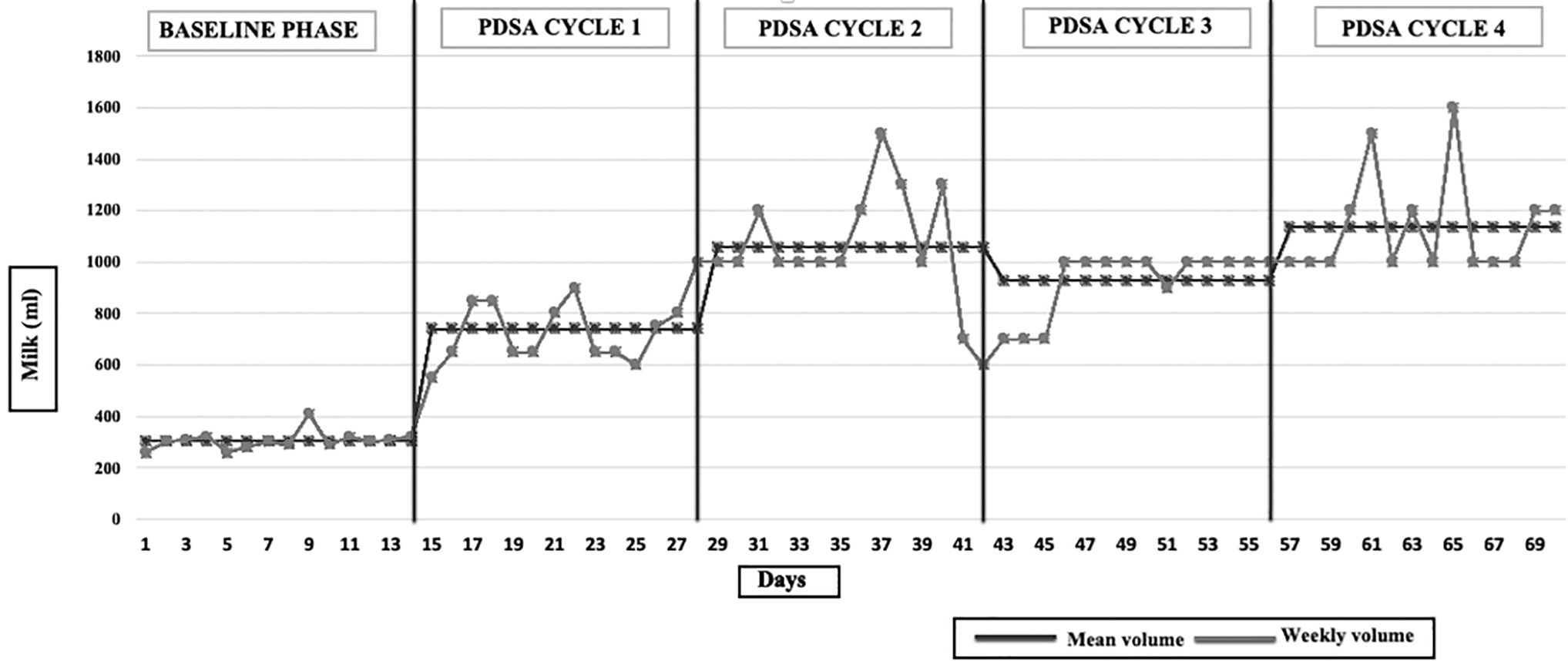
Run chart depicting daily collection of donor milk (in milliliters) during different Plan-Do-Study-Act cycles.
In the second PDSA cycle, we conducted daily counseling sessions in groups of six to eight mothers ensuring COVID-appropriate behavior. Over a 2-week duration, the milk volume increased to an average volume of 1,050 mL/day (Fig. 2). Feedback from the mothers was positive as they found the sessions helped them in improving their knowledge and skills of milk expression, and in alleviating their fear regarding milk donation., In view of the positive outcome, the group counseling sessions were continued and included as part of routine counseling of NICU mothers.
After the second PDSA cycle, there was an unexplained decrease in the number of admissions to NICU, from an average of 20–25 to 12–15 per week over the next 2 weeks. As a result, the total number of mothers available for milk donation declined and we were unable to initiate a new intervention. Although the previous two adopted interventions were continued during the extended PDSA 2 (PDSA 2E) cycle, there were fluctuations in volume collected.
With a subsequent normalization in the NICU admission rate, the third PDSA cycle was initiated. During this 2-week cycle, one-to-one counseling was done and the milk expression technique was demonstrated. Individual attention was given to the mothers by the support group leaders, particularly to those mothers who were poorly motivated and had difficulties in milk expression. During this cycle, we successfully achieved a sustained target of 1,000 mL/day over the 2 weeks (Fig. 2), and therefore, the intervention of this PDSA was adopted as a routine NICU practice.
During the PDSA cycle four, we increased the availability of two breast pumps at a dedicated place within the NICU and allowed mothers to use them 24 hours a day. There was an improvement in the amount of milk collected with an average volume of 1,100 mL/day during these 2 weeks (Fig. 2). The implementation of these four interventions led to the successful achievement of our aim and the interventions were incorporated into our unit policy.
During the sustenance period, we continued regular training and motivation sessions to NICU residents and nursing staff, along with daily group counseling of mothers, individual one-to-one counseling of mothers by support group leaders thrice weekly, and ensured availability of breast pumps throughout the day and night. We were able to sustain our donor milk volume to around 1,000 mL/day over the first 2 months of the sustenance period.
Unfortunately, during the third month of the sustenance period, the city encountered the second wave of the COVID-19 pandemic, which again led to a decrease in the number of health care personnel available, thereby affecting the training of HCWs and counseling of mothers. The team members discussed the challenges faced and decided to restrengthen and regularize the successful interventions of the same PDSA cycles over 2 weeks. On achieving this, we were able to reach our target of daily collection once again (Fig. 3).

Run chart depicting daily collection of donor milk (in milliliters) during sustenance phase.
Although the sustenance phase was affected by the second COVID-19 wave, prompt identification of the issues and timely interventions prevented the donated volume from dropping to preintervention levels. Currently, after showing positive results, we have adopted these successful interventions into our unit policy and continue to practice them as a routine.
Discussion
The COVID-19 pandemic presented unique challenges to health systems across the globe in maintaining established standards and ensuring compliance with best practice models. Overwhelming health care needs, diversion of resources and personnel, and logistic barriers had led to a negative impact on many patient-centered activities in the NICU such as lactation counseling, kangaroo mother care, and human milk donation. In our study, we documented the impact of a QI project to increase milk donation to the HMB post-COVID-19 pandemic. Various problems identified included irregular training and motivation of HCPs, disruption of counseling sessions, lack of regular lactation rounds, and limitation of breast pump availability. Key interventions such as regular training and motivation sessions to HCPs, reinitiating of counseling and support to mothers, initiation of regular lactation rounds, and increasing availability of breast pump, which were planned and implemented through various PDSA cycles, were found to be successful.
Counseling can enable a person to develop positive feelings, experiences, and behaviors that would facilitate positive behavior modification. Garegrat et al. evaluated the impact of counseling of mothers on the improvement of milk donation and found that counseling mothers increased the volume of breast milk donation from 0 mL baseline to a weekly maximum of 7,070 mL after the ninth week of the initiative. 9 A similar study by Sivanandan et al. used interventions such as promotion of exclusive breastfeeding and donation counseling by lactational counselors, and showed a significant increase in the mean monthly donated volumes from 28.2 to 34.1 L. 10 Similar to the above studies, the key interventions in our study also focused on counseling of the mothers in groups by HCPs, as well as individually by lactational counselors, which resulted in an increase in the donated volume.
Hospital-grade electric breast pump was found to be useful in providing assistance in milk expression, especially for mothers who had preterm delivery, stress, medical morbidities, and cesarean delivery. 10 In a randomized trial by Lussier et al., the use of a hospital-grade electric breast pump resulted in a greater milk output in comparison with hand expression. 8 Similarly, in our study, the intervention of increasing the availability of breast pumps to 24 hours a day for mothers within the NICU resulted in a larger volume of milk expression and a subsequent increase in the donated milk volume.
Sustainability of a QI study is possible only when the successful changes become a part of the system and are incorporated in the NICU standard operating procedure. Therefore, to continue improvement, the regular counseling sessions and support for mother by lactation counselors are streamlined, strengthened, and reestablished as in the prepandemic era.
This study also highlights the fragility of the milk bank services globally with a new infection having a severe impact on its functioning due to lack of knowledge on the viral presence in breast milk and the transmission of the disease through breast milk feeding. A similar experience was noted in the late 1980s when, following the discovery of the human immunodeficiency virus, several debates were raked up about the measures essential to ensure safe milk banking.11,12 As milk banks provide a vital contribution to the support, promotion, and protection of maternal lactation and breastfeeding, in addition to the prevention of necrotizing enterocolitis in preterm and low birth weight infants, prompt measures to address these issues of infection transmission require appropriate prioritization to protect staffing and functionality.
To our knowledge, there is no similar published QI study addressing and overcoming the milk bank crisis due to the pandemic. This quality initiative study was completed with available human resources in a busy NICU, with no additional personnel for increasing the quality or ensuring long-term sustainability. For effective close-loop communication among team members, technology such as WhatsApp software was found to be useful. Regular and real-time auditing and feedback played an important role in our QI study.
Conclusions
QI initiatives customized for local settings can result in significant improvement in voluntary milk donation in HMBs, thereby making more PDHM available to premature neonates. Regular training and motivation of HCPs, counseling and support to mothers, regular lactation rounds, and availability of breast pump were key interventions identified in improving milk donation. The COVID-19 pandemic generated a growing interest in, and need for, evidence-based tools to facilitate the implementation of disrupted patient management practices, and QI framework is a useful tool to achieve changes in the same.
Footnotes
Acknowledgment
The authors wish to thank Dr. Sangeeta Ravat, Dean, Seth G.S Medical College and KEM Hospital, Mumbai, for granting permission for publication.
Authors' Contributions
R.N., N.M., D.M., and V.K.V.: conception and design of the study; V.K.V. and K.S.B.: collection of data; V.K.V., D.M., and N.M.: interpretation of data. All authors contributed to the critical review of data analysis, article writing, drafting/revising the article, approving the final version, and accept accountability for all aspects of the work.
Ethical Approval
IRB: As this is a QI study, only clearance from department review board (DRB) is required, which was taken.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.