
Abstract
Background:
Human milk (HM) is a proven optimal food for preterm infants. However, there is uncertainty regarding the effects of different proportions of HM of the total enteral intake on health outcomes in preterm infants. Therefore, we conducted a systematic review of studies examining the effects of different proportions of HM of the total enteral intake on health outcomes in preterm infants.
Methods:
We conducted a literature search in the Web of Science, PubMed, and Scopus databases. The methodological quality of the included articles and the certainty of evidence were assessed according to the Newcastle-Ottawa Scale and the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) tool, respectively.
Results:
Twelve studies were included in the review. Among the clinical findings, the effect of different proportions of HM of the total enteral feeding on health outcomes in preterm infants was divided into six primary outcomes: physical growth, length of stay, morbidity of any disease, all-cause mortality, feeding-related outcomes, and other health outcomes. The studies presented a high risk of bias for most of the domains. The certainty of the evidence was considered low or very low.
Conclusions:
The findings reiterated that greater proportions of HM positively affect the health outcomes of preterm infants. Overall, when the HM accounts for at least 20% of the total enteral intake, it has an effect on health outcomes in preterm infants. If the proportion of HM reaches 50%, the incidence and severity of necrotizing enterocolitis, as well as the time to reach enteral feeds, will be reduced. Increasing the proportion of HM in enteral feeding should be considered a priority in the feeding strategy for preterm infants in clinical practice.
Background
Human milk (HM) is the optimal food for infants, especially preterm infants or very-low-birth-weight (VLBW) infants. 1 The types of HM feeding used for preterm infants include the mother's own milk (MOM) and pasteurized donor milk. MOM contains various important nutrients and bioactive substances, including immunoglobulins, cytokines, growth factors, and prebiotic oligosaccharides. 2 However, VLBW infants cannot meet their nutritional needs with HM alone because their needs for protein, energy, fatty acids, minerals, and micronutrients exceed those of healthy term infants. Therefore, infants who are fed only HM can be supplemented with HM fortifier (HMF) to meet their growth and development needs.
Current studies have shown that HM plays an important role in reducing preterm birth-related complications and diseases, such as late-onset sepsis (LOS), retinopathy of prematurity (ROP), bronchopulmonary dysplasia, and necrotizing enterocolitis (NEC).3–5 NEC is the most common gastrointestinal disease seen primarily in preterm infants and is one of the most devastating intestinal diseases seen in neonatal intensive care units (NICU). 6 Studies have shown that the majority of NEC (>90%) occurs in preterm infants, and NEC has a mortality rate as high as 20–45%. 7 Neonatal nutrition, especially HM feeding, has been shown to play an important role in preventing NEC in preterm infants.7,8
However, although HM is beneficial for preterm infants, it is difficult for many preterm infants to achieve their actual feeding needs due to various subjective and objective factors, such as mother-infant separation, the mother's willingness to breastfeed, and maternal-related complications. According to the World Health Organization, there has been an increase in the incidence of preterm birth and a low percentage of exclusively breastfed infants (available assessment on December 5, 2022). Therefore, the proportion of HM in enteral feeding and its association with health outcomes of preterm infants are worth exploring and will be of great significance for the clinical nursing of preterm infants.
The HM proportion was categorized as percentage of total enteral feeding during hospitalization. 9 Meinzen-Derr et al. 8 concluded that there is a dose–response association of HM feeding with a reduction in the morbidity and mortality of NEC after the first 14 days of life in preterm infants. Sisk et al. 10 found that enteral feeding receiving at least 50% HM in the first 2 weeks of life was associated with a six-fold decrease in the odds of NEC. Corpeleijn et al. 2 reported that preterm infants who received >50% HM experienced a decreased composite risk of infection, NEC, and death. Previous studies indicated that HM plays a significant role in the health outcomes of preterm infants; moreover, there is a strong dose–response relationship. However, the effect of different proportions of HM on the health outcomes of preterm infants remains unclear.
In this systematic review, we aimed to summarize the available evidence and comprehensively describe the effect of different proportions of HM of total enteral feeding on the health outcomes of preterm infants during hospitalization.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) statement 11 (Supplementary Table S1).
Eligibility criteria
The inclusion criteria applied in this systematic review were proposed according to the PICOs framework, which is based on describing the population (P), interventions (I), comparison (C), outcomes (O), and study types (s) (Table 1).
Inclusion Criteria Based on PICOs Framework
GW, gestational week, HM, human milk.
The exclusion criteria identified for this systematic review were (i) studied in which the participants were not preterm infants; (ii) in vitro or animal studies; (iii) reviews, letters, protocols, comments, case reports, and expert opinions; (iv) interventions that did not meet the inclusion criteria; (v) studies published before 2010; and (vi) articles not published in English.
Search strategy
The search was performed using PubMed, Web of Science, and Scopus. Articles published until December 2022 were retrieved. We used population and intervention terms to develop a search strategy: (infants, preterm OR premature infant OR preterm infant OR preterm infants OR premature infants OR neonatal prematurity OR prematurity, neonatal) AND (breast milk OR breastmilk OR human milk OR maternal milk OR mother milk OR breast-fed OR breastfed OR breast fed OR breastfeeding OR breast feeding OR milk sharing OR sharing milk OR human milk OR exclusive breast feeding OR exclusive breastfeeding).
Data extraction
For each eligible study, two reviewers independently extracted some information regarding the characteristics of included studies and participant characteristics. The following characteristics of each study were extracted: author, country, study design, participants, study duration, intervention, and health outcome. The following characteristics of the participants were extracted: birth weight, gestational week, sex, and baseline information.
Evidence assessment
Two reviewers assessed the methodological quality of each study according to the Newcastle-Ottawa Scales (NOSs). 12 Eight items are used to evaluate study quality. The NOS is divided into three dimensions: selection, comparability, and outcomes: for case–control studies, selection (scale from 0 to 4), comparability (scale from 0 to 2), and exposure (scale from 0 to 3), and for cohort studies, selection (scale from 0 to 4), comparability (scale from 0 to 2), and outcome (scale from 0 to 3). The score was categorized into three groups: 0–3, 4–6, and 7–9 NOS points which represented very high, high, and low quality. A higher NOS score indicates better study quality. Any assessment discrepancies were resolved through discussion or by a third reviewer.
Two reviewers evaluated the quality of evidence, which was of statistical significance according to the guidelines of the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE). 13 The GRADE tool assesses the level of bias according to the following factors: (i) risk of bias, (ii) inconsistency, (iii) indirectness, (iv) imprecision, and (v) publication bias. The quality of evidence was rated as very low, low, moderate, or high. Any disagreements were resolved by discussion or consultation with a third reviewer.
Results
Study selection
Articles retrieved according to the search strategy and published from 2010 until December 2022 were retrieved. Initially, 12,697 records were retrieved through the databases. After removal of duplicates, 7,802 records remained. Through screening titles and abstracts, 80 records were retained for full-text reading. Sixty-eight studies were excluded for the following reasons: (i) grouping exposure did not involve quantification of the HM; (ii) feeding intake data were collected during hospitalization; (iii) only study characteristics, not the full study, were included; (iv) health outcomes were not measured during the neonatal period (within 1 month); (v) study was published in a language other than English; and (vi) other reasons. Finally, we were able to include 12 articles in this systematic review that met the inclusion criteria. The search and selection processes are described in Figure 1.
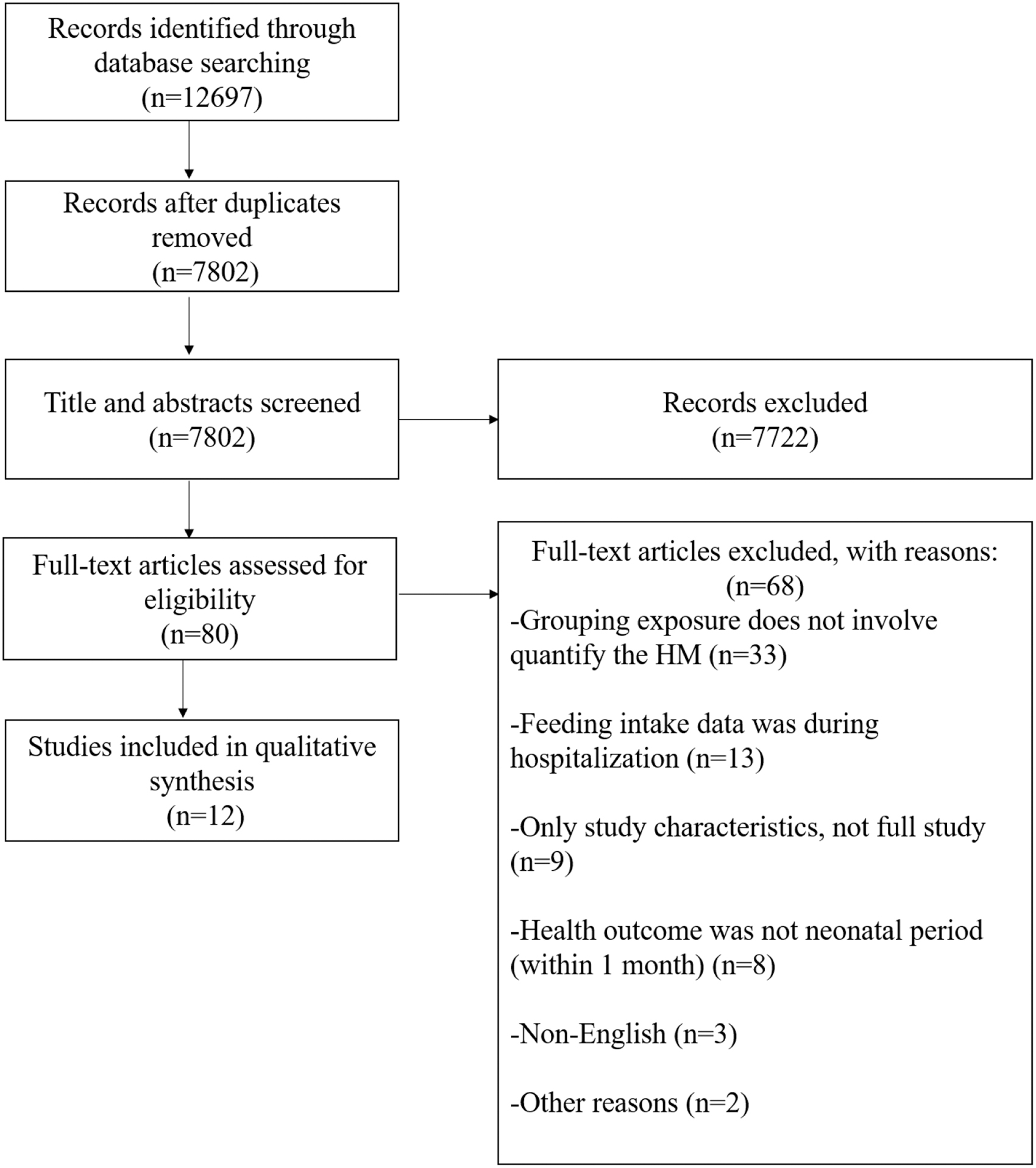
The flow diagram of study selection.
Characteristics of included studies
Twelve unique studies were identified for this systematic review and included 11 cohorts and a case–control study. In total, 3,328 preterm infants were enrolled in the systematic review. The proportion of HM to total enteral feeding was the intervention, and its effect on health outcomes was assessed. The primary outcomes were physical growth, length of stay (days), morbidity of any disease, all-cause mortality, outcome related to feeding, and other health outcomes. The characteristics of the included studies are summarized in Table 2.
characteristics of Included Studies
A: Physical growth; B: Length of stay; C: Morbidity of any disease; D: All-cause mortality; E: feeding-related outcomes; F: Other.
BW, birth weight; GW, gestational week; HM, human milk; MM, maternal milk; NOS, Newcastle-Ottawa Scale; PF, preterm formula; PDHM, pasteurized donor human milk.
Quality assessment of the included studies
The results of the quality assessment according to the NOS tool are shown in Table 2. The NOS scores of the included studies ranged from 7 to 9. According to the above criteria, all the studies were of high methodological quality.
The quality of statistically significant evidence according to the GRADE guideline is shown in Table 3. The quality of evidence was rated as “high,” “moderate,” “low,” or “very low.” The RCTs were first considered as high quality, but could be decreased according to the following aspects: (i) risk of bias, (ii) inconsistency, (iii) indirectness, (iv) imprecision, and (v) publication bias. The results showed that the proportion of HM exposure was associated with low or very low quality for related health outcomes.
Evidence Quality Assessment According to the GRADE Guidelines
↓ Decrease, ↑ increase.
NEC is defined as Bell's stage ≥II. 6
SAEs are defined as excluded events during initial hospitalization that might be expected in the natural course of the preterm infant (except death).
Intervention: the proportion of HM (%).
Comparsion: comparison for this systematic review.
Downgraded (−1) for risk of bias in the allocation concealment and blinding of outcome assessor.
Downgraded (−1) for imprecision due to wide 95% confidence interval consistent with “no effect.”
Downgraded (−1) for indirectness due to lack of a consistent definition between included studies.
Downgraded (−1) inconsistency of findings assessed the health outcome as a secondary outcome.
Downgraded (−1) for risk of bias as confidence in the findings of the reviews which contributed to this outcome was judged to be low.
Downgraded (−1) for imprecision and inconsistency of findings, due to a number of methodological weakness (high risk of bias in randomization sequence generation, allocation concealment, and blinding) and use of different outcome measures.
Downgraded (−1) for imprecision due to small sample size.
Gp, group; GRADE, Grading of Recommendations, Assessment, Development, and Evaluation; HC, head circumference; HM, human milk; IVH, intraventricular hemorrhage; LOS, late-onset sepsis; NEC, necrotizing enterocolitis; PF, preterm formula; PDHM, pasteurized donor human milk; SAEs, serious adverse events; SDS, standard deviation scores.
Analysis of health outcomes
The protective effects of the intervention on preterm health outcomes of included studies are presented in Table 4. Overall, 12 studies reported related health outcomes in preterm infants. We divided the health outcomes improved by the different proportions of HM of the total enteral intake exposure into six aspects: physical growth, length of stay, morbidity of any disease, all-cause mortality, feeding-related outcomes, and other health outcomes.
Studies on the Association of Human Milk Proportion with Health Outcomes
Statistical significance.
↓ Decrease, ↑ increase.
NEC: NEC is defined as Bell's stage ≥II. 6
Days to reach full enteral feeding was defined as ≥140 mL/kg/day of milk feeds actually administered for more than 24 hours. 23
Feed intolerance is defined as the need to cease enteral feeds for more than 4 hours. 24
EOS, early onset sepsis; HC, head circumference; IVH, Intraventricular hemorrhage; LOS, late-onset sepsis; NEC, necrotizing enterocolitis; NR, not report; NSD, no statistical significance; PF, preterm formula; PIVH, periintraventricular hemorrhage; RDS, respiratory distress syndrome; ROP, retinopathy of prematurity; SAEs, serious adverse events; SDS, standard deviation scores; SGA, small for gestational age infant.
Physical growth
Growth parameters such as weight, length, and head circumference (HC) are used in nutritional evaluation. The most commonly reported growth parameters are the z-score for weight gain (g/kg/day) during hospitalization. z-Score for weight, length, and HC is measured during hospitalization (at hospital discharge or birth). 14 The change in z-score has potential utility as an outcome measure for monitoring clinical quality improvement. Ten studies9,10,14–21 investigated the association between the proportions of HM of the total enteral intake and physical growth. All included studies were deemed of high quality.
Four studies9,14,16,18 identified a negative association between the proportions of HM of the total enteral intake and growth. Chowning et al. 14 reported that preterm infants who received ≥90% HM had a more significant decline in weight z-scores and lower HC growth rates than those who received 0% HM. Colaizy et al. 9 concluded that preterm infants fed with >75% HM experienced a significant decrease in weight z-score from hospitalization compared to preterm infants fed with <75% HM. O'Connor et al. 16 found that preterm infants fed with <20% HM had significantly greater mean weight, length, and HC than those preterm infants fed either >80% HM or ≥50% HM. Maas et al. 18 concluded that the standard deviation score for weight during hospitalization decreased by more in preterm infants fed with >75% HM than in those fed with <25% HM. Maas et al. 18 also reported a trend toward preterm infants with >75% HM having poorer weight gain than those fed with <25% HM at discharge.
Meanwhile, two studies15,17 identified a positive association between the proportion of HM of the total enteral intake and growth. Martins-Celini et al. 17 found that length (z-score) was slightly impaired at discharge in the mixed feeding (1–99% HM) group compared to the 100% HM group. Montjaux-Régis et al. 15 reported that weight gain was more pronounced and faster in preterm infants receiving at least 80% HM than in those receiving <20% HM.
Three studies10,19–21 did not find an association between different proportions of HM of the total enteral intake and physical growth from birth until discharge.
Length of stay
Length of stay (days) is measured as the number of days to discharge. 22 The length of hospital stay is associated with disease progression and prognosis, as well as the quality of life of a preterm infant. 23 Seven studies9,10,14–16,21,24 investigated the association between the proportion of HM of the total enteral intake and the length of hospital stay. All included studies were deemed of high quality.
Of all included studies, two studies10,14 demonstrated an association between the proportions of HM of the total enteral intake and length of stay. Chowning et al. and Sisk et al.10,14 concluded that the length of stay for preterm infants who received <50% HM was significantly shorter compared with those with ≥50% HM feeding.
Five studies9,15,16,21,24 concluded that different HM proportions of the total enteral intake had no definite influence on the length of hospital stay.
Morbidity of any disease
The most common complications among preterm infants are mainly due to inappropriate feeding. These complications include NEC, ROP, LOS, intraventricular hemorrhage (IVH), serious adverse events (SAEs), infection, chronic lung disease, meningitis, and intravascular catheter. NEC is defined as Bell's stage ≥II. 6 Twelve of the included studies9,10,14–21,24,25 investigated the association between the proportion of HM of the total enteral intake and morbidity of any disease. All included studies were deemed of high quality.
Six studies9,10,14,16,19,24 concluded that the proportions of HM of the total enteral intake impacted disease morbidity. Chowning et al. 14 found that preterm infants who received ≥90% of their intake as HM had lower rates of NEC than those who received 0% HM, and the lower NEC rates also remained apparent in the ≥50% HM cohort. Colaizy et al. 9 showed that preterm infants receiving <50% HM had lower rates of LOS than those receiving ≥50% HM. Colaizy et al. 9 also reported that preterm infants receiving <75% had lower rates of IVH than those receiving >75% HM. O'Connor et al. 16 revealed that preterm infants fed >80% HM or >50% HM had fewer SAEs than those fed <20% HM.
Sisk et al. 10 reported that preterm infants who received <50% HM had a higher incidence of NEC than preterm infants receiving ≥50% HM. Sisk et al. 24 showed that ≥50% HM was associated with a lower incidence of NEC in preterm infants compared with fed ≥50% preterm formula (PF). Hylander et al. 19 reported a lower incidence of LOS/meningitis among preterm infants fed 100% HM compared with those fed 0% HM. Hylander et al. 19 also reported that ≥20% HM was associated with a lower rate of infection in preterm infants compared with those fed <20% HM, although there was no dose–response effect between the proportion of HM provided and the incidence of infections.
Six studies15,17,18,20,21,25 showed no significant association between the proportion of HM of the total enteral exposure and morbidity of any diseases.
All-cause mortality
We assessed the effect of the proportions of HM of the total enteral intake on all-cause mortality based on four high-quality studies.10,14,21,24 Chowning et al. 14 concluded that preterm infants who received ≥90% of their intake as HM had lower mortality rates than those who received 0% HM, and the lower mortality rates also remained apparent in the ≥50% HM cohort.
Three studies10,21,24 concluded that the proportions of HM of the total enteral intake had no significant effect on all-cause mortality, but the mortality related to NEC was reported to be significantly reduced.
Feeding-related outcomes
Ten of the all included studies9,10,14–16,18–21,24 investigated the proportions of HM of the total enteral intake and feeding-related outcomes. The main feeding-related outcomes were as follows: days of HM, first time to reach full enteral feeding, feeding intolerance, feeding supplementation (protein supplement), and first PF exposure. The first time to reach full enteral feeding was defined as ≥140 mL/kg/day of milk feeds administered for more than 24 hours. 26 Feeding intolerance is defined as the need to cease enteral feeds for more than 4 hours. 27 Ten of the all included studies9,10,14–16,18–21,24 investigated the association between the proportions of HM of the total enteral intake and health outcomes related to feeding. All included studies were deemed of high quality.
Six studies9,14,16,18,21,24 concluded the association of different proportions of HM of the total enteral intake with health outcomes related to feeding in preterm infants. Chowning et al. 14 reported that the days of HM in those receiving ≥90% HM were significantly higher than that in those receiving no HM feeding and that lower days of HM also remained apparent in the ≥50% HM cohort. Colaizy et al. 9 revealed that infants receiving larger proportions of HM were more likely to receive protein supplementation than those receiving lower proportions of HM. O'Connor et al. 16 considered that the number of days to reach full enteral feeding in preterm infants fed <20% HM was less than that in those fed with >80% HM.
Sisk et al. 24 demonstrated that the timing of first PF exposure differs between groups with ≥50% pasteurized donor human milk receiving PF significantly later than the ≥50% HM group or ≥50% PF group. Sisk et al. 24 also concluded that the ≥50% HM group received protein supplements for significantly longer than the ≥50% PF group, and the ≥50% PF group did not receive any protein supplements. Maas et al. 18 explored a slightly lower cumulative protein intake in preterm infants receiving >75% HM compared with those receiving <25% HM. Sisk et al. 21 concluded that preterm infants fed at least 50% HM needed fewer days to reach full enteral feeding than those fed <50% HM.
Four studies10,15,19,20 found no significant association between the proportions of HM of the total enteral intake and feeding-related outcomes.
Other health outcomes
Four of the included studies14,19,20,25 investigated the association between the proportions of HM of the total enteral intake and other health outcomes (hospital readmissions, hospital cost, and microbial community). All included studies were deemed of high quality.
Three studies16,20,25 investigated the association between the different HM proportions of the total enteral intake and other health outcomes. O'Connor et al. 16 concluded that preterm infants fed with >80% or ≥50% HM had significantly fewer hospital readmissions than those fed <50% or <20% HM. Parker et al. 20 concluded that providing at least 50% HM feeding was associated with higher hospitalization costs than formula feeding in the preterm term in the NICU. Zanella et al. 25 showed a difference in the microbial community from those fed with different proportions of HM: the greatest microbial richness was found in those who received 100% HM in comparison with those that received different proportions of formula.
Hylander et al. 19 reported that a greater proportion of HM of the total enteral intake had no significant effect on the length of NICU stay, but the number of days showed a downward trend.
Discussion
Several studies have identified that a greater HM proportion of the total enteral intake plays a protective role in health outcomes in preterm infants. However, there are no definitive conclusions summarizing the effect of the precise HM proportion of the total enteral intake on health outcomes in preterm infants. To address this problem, we evaluated 12 studies of different HM proportions of the total enteral intake in preterm infants to summarize its effects on health outcomes.
Our systematic review of 12 studies of 3,328 preterm or VLBW infants found that the proportion of HM of the total enteral intake is positively associated with the health outcomes of preterm infants on the whole. We evaluated and summarized the effect of different HM proportions of the total enteral intake on health outcomes of preterm infants based on physical growth, length of stay, the morbidity of any disease, all-cause mortality, feeding-related outcomes, and other health outcomes. Although the quality of evidence was of low or very low certainty, the methodological quality was high.
Based on 2,039 preterm infants from 4 studies, this review found a negative relationship between in-hospital growth and the proportion of HM of the total enteral consumed. We concluded that at least 20% of total enteral feeding of HM has an effect on the physical health of preterm infants. Meanwhile, we also found that 50% of total enteral feeding was HM, which may have a negative association with growth of preterm infants. There are three possible explanations for this result. First, preterm infants fed primarily with HM cannot meet their nutritional needs, because their energy, fatty acid, and micronutrient requirements are much higher than those of term infants. Second, recent studies revealed that the growth of preterm infants is linearly related to their protein intake. 9 A possible explanation for the slower growth rates among infants fed predominantly HM is the lower protein intake and the fact that the participants were VLBW infants. Finally, pasteurized HM has a lower macronutrient content than MOM.
Based on 55 preterm infants from one study, these findings are inconsistent with those of Régis et al., 15 who demonstrated that ≥80% HM intake promoted weight gain during hospitalization of preterm infants compared to those fed <20% HM. There are several mechanisms to explain the difference between those findings and the results of this review. First, pasteurization of HM is not performed in their NICU. Second, standardized enrichment of HM was implemented. MOM produced by mothers who deliver preterm is higher in protein, total lipids, long-chain polyunsaturated fatty acids, growth factors, and hormones. 28 Finally, preterm infants receive more MOM and are properly fed HMF to meet their nutritional needs.
Different HM intakes may be an influential factor on the incidence and development of NEC. Based on 3 studies involving 1,303 preterm infants, at least 50% of HM is associated with lower rates of NEC.10,14,24 Chowning et al., Sisk et al., and Sisk et al.10,14,24 reviewed the proportion of HM on NEC and concluded, in line with our results, that preterm infants receiving ≥50% HM had a more significant reduction in the risk of NEC than those on diets of <50% HM. This finding is in line with the primary health outcomes. Although the remaining eight studies9,15–20,25 reported that a higher proportion of HM did not significantly decrease the incidence and severity of NEC in preterm infants, there was still an overall positive trend. Therefore, we believe that feeding ≥50% HM could effectively reduce the incidence of NEC in preterm infants.
The findings from the included studies also support the notion that a great proportion of HM promotes feeding-related health outcomes in preterm infants, for example, by decreasing the time required to reach full enteral feeding. Establishing full enteral feeding is an important goal for preterm infants in the NICU. We found an effect that at least 20% of the total milk intake is HM on the time to reach full enteral feeding in preterm infants, and receipt of ≥50% of the total enteral feeding as HM during hospitalization was associated with a shorter time to full enteral feeding. Our results are also consistent with the earlier finding by Sisk and Conor et al.16,21 that an increase in the proportion of HM intake reduced the time to achieve full enteral feeding. Although three studies15,18,19 showed that a higher proportion of HM of the total enteral intake did not have a statistically significant effect on reaching full enteral feeding in preterm infants, there was still a decreasing trend in the number of days. Therefore, we believe that the proportion of HM of 50% could effectively reduce the time needed to reach full enteral feeding in preterm infants.
Therefore, it may be preferable for preterm infants to receive greater rather than lower proportions of HM during their hospitalization. Certain limitations of our study should be noted. First, despite a systematic search, relevant articles may have been missed. Second, the results should be interpreted with caution, because the included studies were either case–control studies or cohort studies for which the quality of evidence on outcomes was limited. Finally, due to the heterogeneity in the methodology and the approach used to present results among the included studies, a meta-analysis could not be performed.
Conclusions
In this systematic review, we have integrated the current evidence and found that the effects of different proportions of HM of the total enteral intake on health outcomes are mainly reflected in the following six aspects: physical growth, length of stay, morbidity of any disease, all-cause mortality, feeding-related outcomes, and other health outcomes. We found that at least 20% of the total enteral intake as HM has an effect on health outcomes in preterm infants, and the protective effect on health outcomes was mainly observed in preterm infants fed with a greater proportion of HM. Therefore, efforts to increase the proportion of HM of the total enteral intake could be considered an important clinical strategy to improve the health outcomes of preterm infants. However, owing to the low certainty of most of the evidence, future clinical observation and research are still needed to focus on the effect of different HM proportions of the total enteral intake on short and long-term health outcomes in preterm infants to provide an optimal clinical feeding strategy.
Footnotes
Authors' Contributions
Y.S. contributed to the design of review protocol, define the research theme, screen the eligible studies, conduct data extraction, and revise the article. K.L. contributed to screen the eligible studies, conduct data extraction, analyze data, make the tables, and write the article. J.G. and J.Y. contributed to interpret the results and give expert advice on the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (81601330—Yanwei Su ), Natural Science Foundation of Hubei Province (2022CFB178—Yanwei Su), and the Fundamental Research Funds for the Central Universities (HUST: YCJJ202201053—Keqin Liu). The funding contributed to defining the research theme, and there was full accountability in ensuring the integrity and accuracy of the work, analyzing the data, and interpreting the results.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.