
Abstract
Background:
Avoidance of early formula feeding (EFF) and advancement of mother's own milk (MOM) in very low birth weight (VLBW) infants are important health influencers to decrease serious morbidities.
Objective:
To present the challenges and feeding strategy successes implemented to counteract a decline in MOM at discharge after initiation of donor milk (DM) to avoid EFF in racially and ethnically diverse VLBW infants.
Patients and Methods:
Retrospective review of prospectively tracked inborn surviving VLBW infants and their mothers admitted to neonatal intensive care unit from 2010 to 2020 during three feeding strategy implementations baby friendly (BF), DM program, and MOM bundle. Analysis included type of feeding (MOM, DM, or formula) and maternal with descriptive and comparative statistical analysis as indicated.
Results:
Analysis included 616 VLBW infants. Initiation of BF program resulted in 58.5% of infants discharged on MOM with 41.5% exposed to EFF. Initiation of the DM program resulted in a decline in EFF to 5% and decline in MOM at discharge to 26%. MOM bundle strategy resulted in an increase in MOM at discharge to 41% with sustained EFF exposure 0%. MOM at discharge varied among maternal racial and ethnic backgrounds in all epochs. Early DM use was not different among mothers by race or ethnicity with DM by African American (AA) mothers 89% > White mothers 83% > Other/Hispanic mothers 75%. MOM at discharge was lowest for AA mothers 33% < Hispanic mothers 40% < White mothers 55% < Asian/Other mothers at 60%.
Conclusion:
Changes in VLBW feeding strategies to avoid EFF utilizing DM can be successful among diverse maternal racial and ethnic populations. Nursing and maternal education coupled with early lactation support and attention to maternal individual long-term feeding plans were critical to improve MOM at discharge among mothers of all racial—ethnic backgrounds for successful attainment of MOM utilization in term corrected VLBW infants at discharge.
Introduction
Human milk is the preferred nutrition for the very low birth weight (VLBW) infant at risk for morbidities related to prematurity.1–5 In cases where mothers are unable to provide their own breast milk, pasteurized donor human milk (DM) can serve as an alternative and/or bridge during the critical early period in the neonatal intensive care unit (NICU) to avoid early formula exposure.6,7 DM use similarly influences the development of a healthy gut microbiome, as well as reduces the risk of feeding intolerance, necrotizing enterocolitis, infection, and sepsis, compared with infants fed preterm infant formula.
The Children's Hospital of Richmond (CHoR) at Virginia Commonwealth University (VCU) NICU is a level IV NICU with a large population of VLBW infants. The CHoR NICU was designated a baby-friendly (BF) hospital in 2015 with goals to encourage breast milk utilization for all infants using the broad-scale implementation of the 10 Steps to Successful Breastfeeding and the International Code of Marketing of breast milk substitutes. 8 The BF hospital designation aligned well with further goals to limit early formula exposure, increase human milk utilization, as well as advance mother's own milk (MOM) at discharge for the VLBW infant, and facilitated the institution of the NICU pasteurized human donor milk (DM) program in 2017. We hypothesized that early initiation of DM would be a successful bridge to advancing MOM at discharge.
This observational study details successes and limitations encountered in the pathway to advance human milk exposure and MOM utilization at discharge for VLBW infants. In particular, we identify challenges encountered with the initiation of the 2017 DM program and the influence on diverse maternal racial and ethnic cultural response variabilities to DM, as well as successful MOM strategies implemented, which were required to combat an inadvertent observed decline in MOM utilization at discharge after DM initiation.
Patients and Methods
Study design
This study was conducted at the CHoR at VCU Health System. The study was approved as exempt by the VCU Human Institutional Review Board, HM20026634. We conducted a retrospective review of prospective feeding utilization data, as well as the medical records of VLBW infants admitted to the NICU between January 2010 and December 2020 to evaluate infant demographics and incidence of MOM, DM, and formula feeding at discharge. Infants who expired before discharge were excluded since our primary outcome was feeding type at discharge.
Additional infants excluded were those who were not eligible to receive their MOM due to maternal health-related limitations such as maternal exposure to nonprescription opioids or illicit substances, HIV, or mothers taking medications contraindicated with breastfeeding, or infants who would not be in the mother's care after hospital discharge. Demographic and clinical data collected included the following: Date of birth, maternal race and ethnicity, gestational age (GA) at birth, birth weight, gender, single versus multiple birth, and mode of delivery. Clinical parameters collected included the following: Type of enteral feed provided (DM versus MOM), lactation support initiation, feeding type at discharge (any human milk, human milk only, human milk and fortifier/formula, or formula only), and length of stay in the hospital.
DM program
We initiated the DM Program in 2017 soon after the BF designation in 2015, with the aim to avoid formula exposure in the VLBW infant or introduction of DM as a bridge to MOM for all VLBW infants. We affiliated with a Virginia-certified DM Program and instituted early DM feeding for all VLBW infants.
MOM bundle intervention
In 2018, we instituted a MOM bundle in response to identified decline in MOM at discharge for the VLBW infant. We modeled this intervention based on a provider and maternal pilot perception survey related to DM utilization, maternal feeding plan, lactation support, and goals for MOM at discharge.
The survey results that were used to inform the MOM bundle included the following: (1) early (day of life 1 and 2) nurse and parent education on benefits of MOM utilization at the time of admission to the NICU, (2) dedicated NICU lactation consultants, activation of lactation consult at the time of infant admission, and initial maternal lactation consult visit within 7 days of the birth of the VLBW infant, (3) provision and use of a hospital-grade breast pump to mothers within 48 hours of infant admission, and (4) offering DM, but counseling mothers on DM benefits and differences from MOM within 48 hours of admission of the VLBW infant.
Statistical analysis
Data analysis included descriptive statistics with mean and standard deviation for numerical variables, χ 2 and Fisher's exact tests for categorical variables, t-tests for continuous variables, and percentage within different categories for categorical variables. A p-value ≤0.05 was considered statistically significant.
Results
Demographics of study population
In this analysis, 616 inborn VLBW infants who survived to discharge home between 2010 and 2020 were included. Table 1 outlines the demographics of the study population group as before and after institution of the DM program. The mean birth weight was 1,081 ± 309 g versus 1,090 ± 340 g, in the pre-DM and post-DM groups, respectively. The mean GA at birth of 28 ± 3 weeks for both groups. There was no significant difference in the demographical characteristics between the pre-DM and post-DM program groups (Table 1).
Demographic Characteristics of the Study Population (n = 616)
DM, donor milk; NEC, necrotizing enterocolitis; SD, standard deviation; SGA, small for gestational age.
DM utilization after initiation of a DM program
The utilization of DM was available for all infants through 34 weeks corrected gestation to avoid early formula feeding (EFF) in the VLBW infant. In every maternal racial and ethnic category, 100% avoidance of EFF was achieved through the combined use of MOM and DM in this population, Figure 2. The effect of maternal race and ethnicity on DM utilization identified some variability in the use of DM by race or ethnicity, Figure 1. Mothers characterized as Other race and ethnicity were the least likely to utilize DM at 50% with Hispanic mothers at 75% compared to African American (AA) mothers at 89% and White mothers at 83% (Fig. 2); results were not statistically significant (p = 0.33).
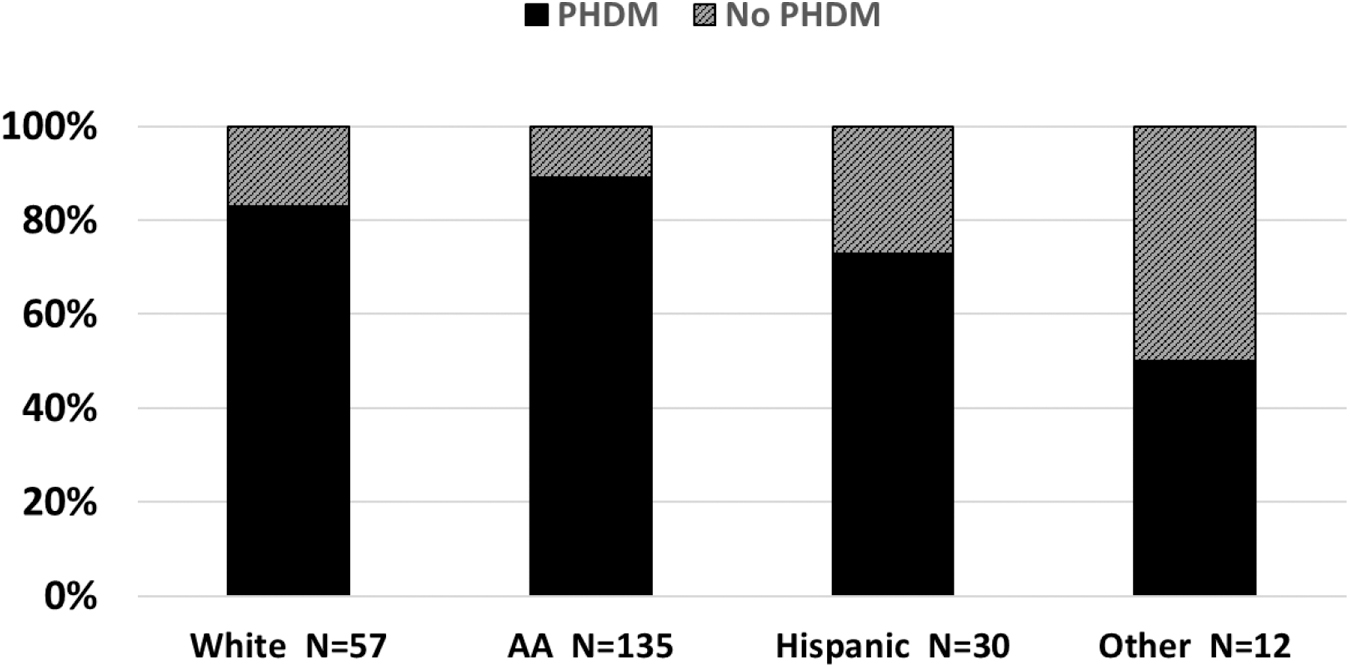
Use of PHDM by maternal race and ethnicity, 2017–2020, n = 234. PHDM, pasteurized human donor milk.
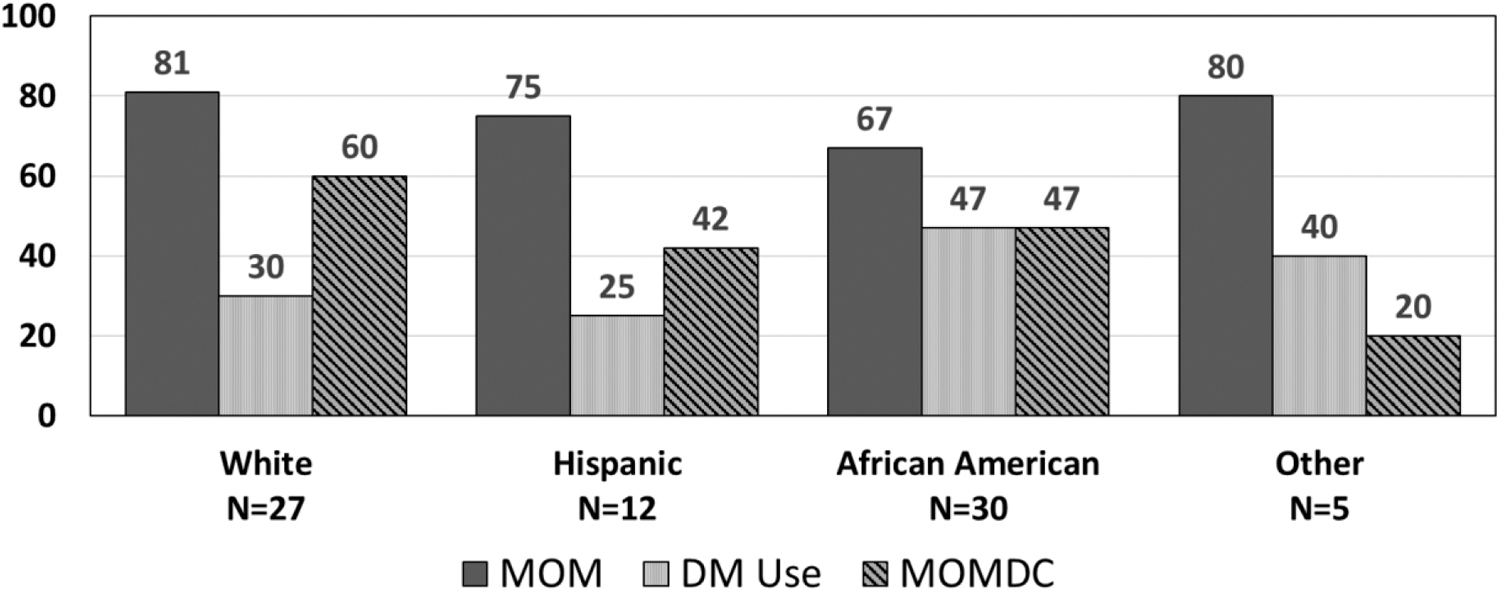
Percentage MOM during hospitalization, DM during hospitalization, and MOM at discharge by maternal race/ethnicity, n = 74 (2020). DM, donor milk; MOM, mother's own milk.
Also, in examination, if DM decreased mother's initiation and utilization of MOM during hospitalization, we noted that regardless of race or ethnicity, the maternal rate of MOM during hospitalization was similar with 67% of AA mothers, 75% of Hispanic mothers, and 81% of White and Other mothers choosing to initiate MOM during hospitalization. However the continued use of MOM declined at discharge with disparities among racial and ethnic groups (Figs. 2 and 3). The decline at the time of discharge was based on maternal individual preference for a variety of reasons, which collectively were due to a return to work-life balance after infant discharge (survey data not shown).
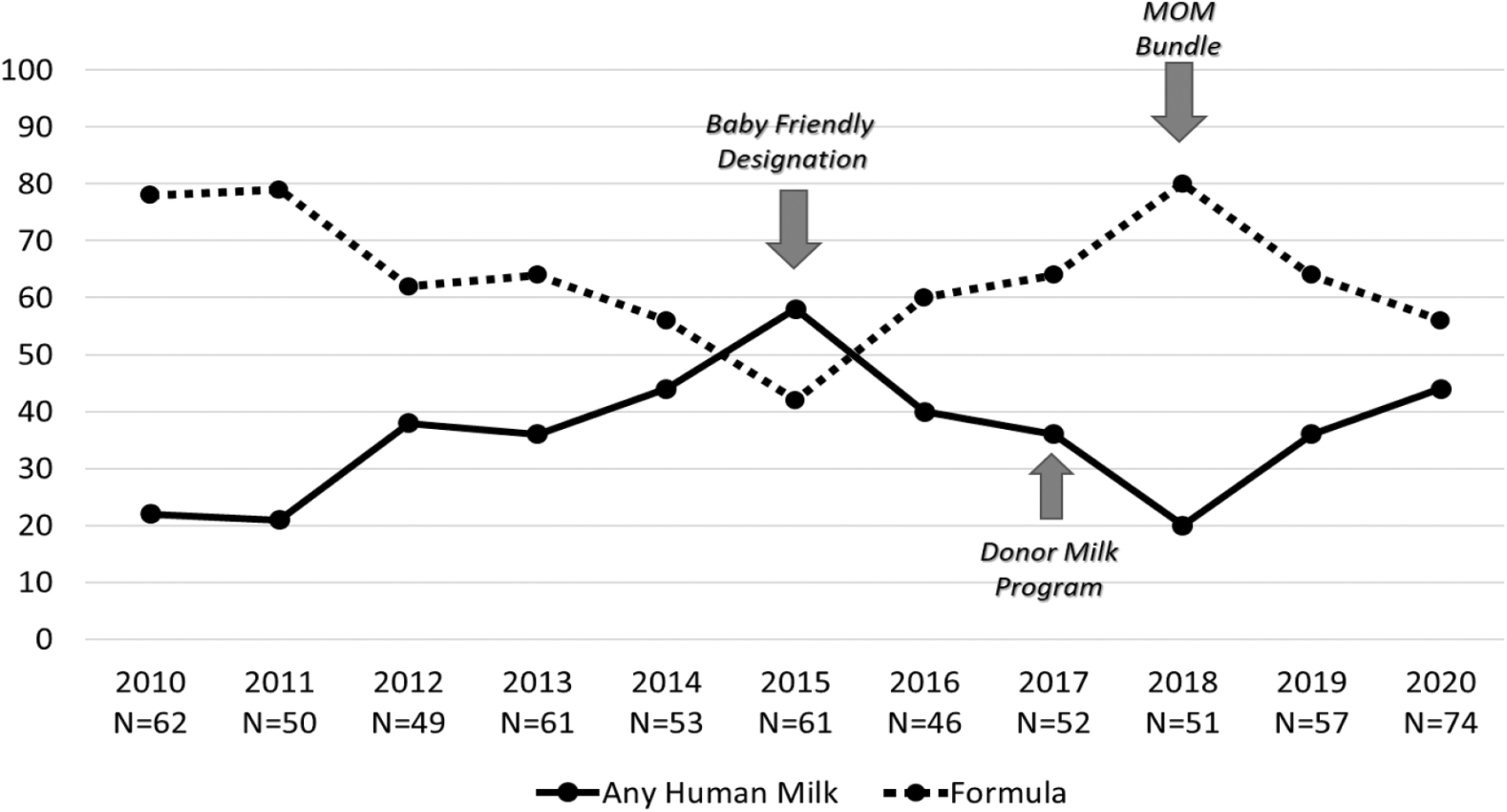
Enteral feeding at discharge for VLBW infants, 2010–2020, n = 616. VLBW, very low birth weight.
Mother's milk at discharge before and after implementation of DM program
Attainment of the BF designation before introduction of the DM program resulted in an increase in MOM at discharge in VLBW infants from 22% in 2010 to 57% in 2015, Figure 3. In examination, if DM decreased MOM during hospitalization, we noted that, although all mothers of VLBW avoided EFF in their infants regardless of race and ethnicity and increased their rates of MOM during hospitalization, the program influenced the continued use of MOM at discharge with a universal decline that reached 19% in 2018, Figure 3. The decline at the time of discharge was based on maternal individual preference for a variety of reasons, which collectively were due to a return to work-life balance after infant discharge, (survey data not shown). In response to the decline in MOM at discharge, implementation of the MOM bundle lead to an improvement of MOM at discharge to 46%, Figure 3.
Mother's own milk at discharge before and after implementation of DM program by maternal racial and ethnicity
In examination of the effect of maternal race and ethnicity on the various initiatives, we identified that, overall there was a uniform increase in MOM at discharge for mothers of all races and ethnicities, with the implementation of the BF designation, Figure 4. These increases were most pronounced within non-White mothers with increase of 66% and 45% for AA and Hispanic mothers, and 37% and 33% increase for White mothers and Mothers of Other race/ethnicity.
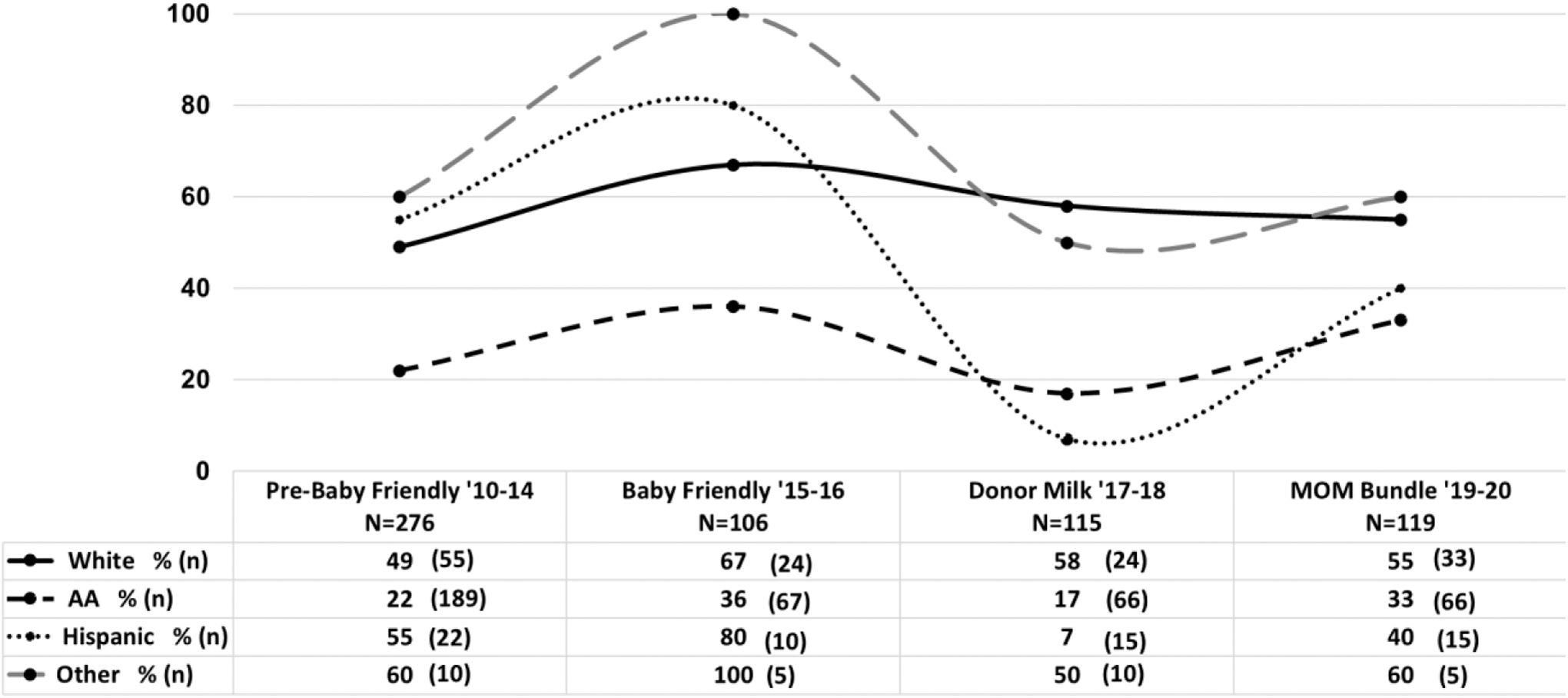
Percentage of VLBW infants discharged on MOM feeding by maternal race/ethnicity during changes in feeding strategies (2010–2020). n = 616.
The initiation of the DM Program was associated with an overall decline in MOM at discharge with greatest decline among Hispanic mothers at 91%, AA mothers at 53%, and other mothers at 50% compared to the 13% decline among White mothers. The institution of the MOM bundle lead to improvement of MOM at discharge for AA mothers to 33% (p < 0.027), and for Hispanic mothers to 40% (p < 0.031), with no statistical change in the level for mothers of White or Other racial ethnic categories where these levels were sustained, Figure 4.
Discussion
Given the importance of early human milk for this high-risk population, our NICU developed several strategies over the years in our goals to avoid formula exposure, including BF Hospital designation and the use of early DM as a bridge and support to MOM initiation and discharge. As a BF designated Hospital, we continuously tracked the nutritional support provided to infants in the NICU to assess need for realignment with successful strategies. In our observation, during the first year of DM initiation, we identified a very positive acceptance of DM by mothers of all cultural backgrounds with nearly 100% successful decrease in formula exposure for the VLBW infant. We evaluated if this was a result in a decline in MOM initiation and found that there were additional factors as well as educational understanding among staff and parents related to the key importance of MOM for the VLBW infant.
However, in evaluating the impact of these initiatives on MOM at discharge, we noted an important decline after the initiation of the DM Program. In our environment, as we sought to avoid all exposure to formula, the early implementation of DM aimed to serve as a bridge during the early initiation of MOM or to avoid formula exposure in all VLBW infants until 34 weeks corrected age in those mothers who chose not to breastfeed was important. To understand the decline in MOM at discharge, we performed a convenience pilot survey of mothers as well as nurses in the NICU related to perception in MOM and DM use. Through these surveys, we identified that MOM was regarded as the best source of nutrition for all infants by both mothers and nurses.
We noted that almost half of nurses and mothers were concerned about the safety of DM for infants as well as concerns that DM might interfere with successful breastfeeding during hospitalization. These results informed the changes that we incorporated into a MOM bundle that included nursing and maternal education related to the timing and important distinctions between MOM and DM, the safety of DM, and the importance that MOM continued as long as possible as the best nutrition for their infant. We also identified that maternal lack of early access to lactation support within a 7-day period, including breast pump availability in each private room within 72 hours, was a barrier to MOM use. These MOM supportive strategies were incorporated into the DM Program guidelines, which were critical for improvement in MOM at discharge.
In our NICU, initiation of DM resulted in >95% of VLBW infants exposed to human milk in the form of DM, MOM, or both through 34 weeks corrected age, accounting for at least 2 months during their hospitalization in the NICU. Thus, the DM strategies were successful in decreasing formula exposure in our VLBW population through a critical developmental phase. Furthermore, the addition of the MOM bundle strategies of early and continued access to lactation support with lactation specialists and lactation equipment, as well as NICU nursing education related to value of sustained MOM compared to DM were additional factors that led to improvement of MOM feeding at discharge in our population.
Our MOM support strategies continued during challenges of the COVID-19 pandemic with the associated maternal infant separation due to the initial widespread concerns for viral transmission by the family to the infant in the NICU, as well as concerns for viral spread in human milk.9,10 Despite the changing implementation of maternal-infant separation policies within our NICU, 11 the VLBW exposure to human milk during hospitalization and discharge on MOM did not decline with consistent support of the strategies employed.
In review of the influence of maternal demographics on MOM at discharge, our investigation identified that mothers of varied race and ethnicity utilized DM consistently. However, the decision for mothers to continue to provide MOM at discharge differed among infants born to AA and Hispanic mothers compared to White mothers with AAs and Hispanic mothers benefitting from additional education and support on the importance of MOM to increase MOM at discharge. Nevertheless, AA mothers had the lowest rate of MOM at discharge at term corrected gestation, despite consistently utilizing DM during the baby's NICU stay.
Overall, the results of our strategies indicate that the use of DM can have an unintended negative influence on MOM use during hospitalization and MOM at discharge. However, these negative effects can be countered by a focused MOM program with intentional lactation support strategies. Our study suggests that inclusion of a DM program to avoid early formula exposure can be extremely successful in providing human milk feeding to the very preterm infant during critical developmental periods. However, the use of DM to serve as a bridge with the goal to increase mother's milk feeding during the NICU hospitalization, as well as MOM at discharge in our population required an additional focused MOM program with attention to maternal lactation support resources and maternal education, as well as mother's feeding plans after the infant is discharged home.
In our populations, maternal racial differences in long-term MOM feeding at discharge appeared consistent with prior studies 12 and emphasized the continued need for individualized and targeted breastfeeding education and MOM support, especially in mothers with limited resources, or mothers who work outside the home who may need special or individualized strategies to support continued MOM at discharge after 40 weeks corrected GA.
Given the prolonged hospitalization in the NICU with a large proportion of mother's who must resume employment, or mothers with additional socioeconomic concerns, individualized considerations must be incorporated in supportive factors that may influence continued MOM feeding of the VLBW or ELBW infant at discharge from the NICU.
Conclusion
Strategies that utilize DM early exposure and support MOM at discharge can be successful in avoidance of formula for the VLBW infant. However, without additional lactation support resources, these strategies alone did not correspond to increased use of MOM at discharge and varied in their effect among maternal racial and ethnic populations. A comprehensive interdisciplinary MOM program coupled with a DM program can be successful in all VLBW infants being exposed to human milk during the critical NICU period and at discharge. It is important to acknowledge that the prolonged length of hospitalization affecting the VLBW infant, of 90–150 days in the NICU, requires emphasis on maternal individualized education and significant lactation support, as well as efforts to target socioeconomic circumstances that can influence MOM feeding at discharge.
Footnotes
Authors' Contributions
K.D.H-M. was responsible for study concept, intellectual concept, and original study design; K.D.H-M., S.N-L., N.C., L.S., M.D., J.X., and V.C. were responsible for study design refinement and methodology; N.D., S.N-L., L.S., and J.X. were responsible for data curation. K.D.H-M., N.D., and N.C. were responsible for statistical analysis; K.D.H-M. and N.D. were responsible for interpretation of data and drafting article. All authors contributed to article reviewing, revision, and editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the CHoR JACKS Summer Scholar Foundation Fund.