
Abstract
Background:
Breast milk (BM) is a nutritive fluid that is rich in bioactive components such as hormones and cytokines that can shape the newborn's feeding habits and program the newborn's immature immune system. BM components can change under different scenarios that include maternal body mass index (BMI) and premature birth. This study aimed to study the interaction of premature status or maternal obesity on the hormonal and cytokine profile in BM according to the sex of the offspring.
Materials and Methods:
We recruited 31 women with preterm births from the Centro de Alta Especialidad Dr. Rafael Lucio in Mexico. Luminex multiplexing assay was used for quantifying cytokine profile of monocyte chemoattractant protein-1, tumor necrosis factor (TNF)-α, interferon-γ, interleukin (IL)1-β, IL-2, IL-4, IL-6, IL-7, and hormones insulin, ghrelin, leptin, and glucagon in mature BM samples. Biological modeling was performed to predict the interaction between cytokines and hormones, maternal BMI status, infant birth sex, parity, and gestational age.
Results:
BM multiplex analysis showed positive correlations for TNF-α and increasing prematurity and for higher maternal BMI and IL-2, IL-4, and IL-6 cytokines. Multiple regression models identified an interaction between maternal BMI and gestational weeks in male infants that is associated to TNF-α accumulation in BM. Biological modeling predicts that preterm delivery in mothers with obesity modulates TNF- α levels in mature BM of women with male offspring.
Conclusion:
Prematurity and obesity modify BM's immune profile. TNF- α expression increases as prematurity increases, and maternal BMI correlates positively with increases in IL-2, IL-6, and IL-4. Our multiple regression model also shows that maternal BMI and gestational weeks in male infants predict TNF-α.
Introduction
Breast milk (BM) is the ideal form of infant feeding, especially during the first 6 months of life, as it provides all the water, nutrients, and bioactive components required for the integral and systemic development of the infant. 1 BM is also dynamic, as the health-programming bioactive components can be changed and adapted according to the body's status.2–4 For instance, day and night cycles can modify the expression of immune, hormonal, and nutritious BM components,2,5,6 and child infection can also trigger specific immune changes in BM. 3
Prematurity can also modulate the immune components of BM, and neonates specially premature are at high risk of infection, 7 as a newborn's immune system is yet immature and not well trained.7–9 Accordingly, the bioactive components in BM such as cytokines can contribute to immune maturation in the newborn by forming complex interactions with immune cells and modulating the infant's immune response allowing a better transition from the womb-protected ambient to an extrauterine environment.10,11 At this stage, the newborn is deficient in cytokines so BM is the main source of cytokines. 11
BM components also regulate pro- and anti-inflammatory response, contribute to maintaining the infant's homeostasis, prevent sepsis, and help in the development of the immune system. 10 For instance, there are reports that pro-inflammatory interleukin (IL)1-β, monocyte chemoattractant protein (MCP)-1, tumor necrosis factor (TNF)-α, interferon (IFN)-γ, IL-2, IL-6, and the anti-inflammatory IL4, IL-7 cytokines control both maternal and newborn health.10,12 Experimental evidence reported a decrease for MCP-1, 8 IL1-β, IL-2, IL-69 and an increase for TNF-α 7 in BM from preterm deliveries compared to term deliveries which mean that cytokines are dynamic and can be modified; however, such immune modulating factors are not completely studied in other scenarios that also include maternal obesity.
Obesity and overweight are a health problem related to abnormal or excessive fat accumulation 13 and persistent chronic low-grade inflammation. 14 The Latin American population is currently heavily affected by overweight and obesity, 15 including during pregnancy, which are related to negative outcomes in newborns. Maternal obesity or overweight affects feeding-related metabolic hormones, showing aberrant changes such as a decrease in ghrelin 16 and an increase in insulin, 17 leptin,16,18 and glucagon. 19 BM bioactive immune components during maternal overweight or obesity can also be modified. A study from Finland showed that BM from mothers with obesity has increased IL-2 and IL-620 and decreased IL-4, TNF-α, and IFN-γ 20 compared to mothers with normal weight. We conceive that the most critical health-programming opportunity through BM takes place during the first stages of life, 1 so maternal obesity could negatively modify immune and hormonal BM components, resulting in negative health outcomes for the newborn.
In the current study, we aim to predict the interaction between maternal body mass index (BMI) status, infant birth sex, parity, and gestational age (GA) on the cytokines and hormone profile in BM.
Materials and Methods
Participants
We recruited 31 women with premature births aged 18 years and older into the study. The women had the intention to breastfeed and attended the lactarium at the hospital “Centro de Alta Especialidad Dr. Rafael Lucio” from April to July, 2022. We integrated two experimental populations which were defined according to World Health Organization (WHO) preterm birth categories by GA. First group was extremely preterm (<28 weeks GA) to very preterm (28 to <32 weeks GA) (EP-VP: <28 weeks GA to <32 weeks GA), and second group was moderately preterm (MP): 32 to <37 weeks GA). 21 In addition, maternal height and weight before pregnancy were collected from medical records for BMI calculation and assigned to one of three groups: normal weight (NW, BMI from 18.5 to 24.9), overweight (OW, BMI from 25 to 29.9), or obese (OB, BMI 30+). All women gave written informed consent. We excluded women with immune deficiencies, confirmed thyroid disorders, metabolic dysfunctions, more than five previous pregnancies, alcohol, tobacco, or illicit drug use, who gave birth to babies with congenital abnormalities.
The current protocol was approved by the research committee of the hospital “Centro de Alta Especialidad Dr. Rafael Lucio” in Xalapa, Veracruz, México (approval no. 18/22).
BM collection
Whole mature BM was collected from postnatal day 21–30 between 9 and 11 am at the lactarium facilities of the hospital “Centro de Alta Especialidad Dr. Rafael Lucio.” BM was collected in 100 mL sterile glass flasks and then aliquoted in 1.5-mL sterile polypropylene tubes and stored at −80°C for multiplex analysis (see below). Qualified staff aided in BM collection using the Marmet technique under hygienic conditions that included hand washing with soap before milk collection and, for the participating women, cleaning the nipple area with soap and water before milk extraction.
BM multiplex analysis
Frozen BM was thawed at room temperature (22°C), vortexed for 15 seconds, and then centrifuged at 605 ×g for 10 minutes at 4°C. The fat supernatant was discarded, and 25 μL of the defatted milk was used for multiplex analysis. For cytokine analysis, we used the HCYTOMAG-60K Human Cytokine MAGNETIC panel/MAGNETIC Cytokines/Chemokines Kit (Merck Millipore, Burlington) for IL-1B, IL-2, IL-4, IL-6, IL-7, MCP-1, IFN-γ, and TNF-α. For hormone analysis, we used the HMHEMAG-34 MILLIPLEX MAP Human Metabolic Hormone Magnetic Bead Panel—Metabolism Multiplex Assay Kit (Merck Millipore) for ghrelin, glucagon, insulin, and leptin. For both analyses, the manufacturer's instructions were followed, and the reads were performed in the Luminex® 200TM Multiplexing Instrument (Luminex Corporation; LX200-XPON3.1).
Multiple regression model
Using data collected from the cytokine and hormonal quantification in BM from women with normal weight, overweight, or obese, a multiple regression analysis was performed to predict the effect of independent variables (Sex, BMI, Gestational week) over the dependent variables (cytokine and hormones in milk). These analyses were performed in R studio version 3.6.3 with the next equation:
lm(Cytokine/hormone − Sex × BMI × Gestational week,database)
Correlation analyses were based on linear regression models presented as beta (β) coefficient and 95% confidence interval. For all performed analysis a p-value ≤0.05 was considered statistically significant (Table 1).
Multiple Linear Regression of Cytokine, Body Mass Index, and Gestational Age
Statistical model female and male.
BMI, body mass index; DF, degrees of freedom; GA, gestational age; IFN, interferon; IL, interleukin; MCP-1, monocyte chemoattractant protein-1; TNF-α, tumor necrosis factor-α.
Statistical analyses
All values obtained from multiplex analysis were normality-tested with Shapiro–Wilk test. Cytokines (IL-1B, IL-2, IL-4, IL-6, IL-7, MCP-1, IFN-γ, and TNF-α) and hormones (ghrelin, glucagon, insulin, and leptin) were compared with sex at birth (male versus female), premature status (EP-VP versus MP), and parity status (primipara versus multipara).
For Gaussian-distributed data, differences were analyzed using unpaired t-test; and non-Gaussian distributed data used Mann–Whitney test. Univariate correlations among evaluated hormones and cytokines between maternal age, maternal BMI, and GA were studied using Pearson correlation test for Gaussian-distributed data and Spearman correlation test for non-Gaussian distributed data (Table 2). When cytokines and hormones were compared in more than two groups (Maternal BMI groups divided as normal weight: NW; overweight: OW; and obese: OB), Gaussian-distributed data were analyzed using one way analysis of variance (ANOVA) with Bonferroni correction for multiple comparisons. For Non-Gaussian distributed data, differences were analyzed using Kruskal–Wallis test with Dunn's correction for multiple comparisons test. Graphs are expressed as mean ± standard deviation, and GraphPad Prism Version 9.0.0 (La Jolla, CA) was used.
Correlations Between Tested Cytokines and Hormones with Age, Body Mass Index, and Gestational Age
Correlations in bold have p ≤ 0.05.
BMI, body mass index; GA, gestational age; IFN, interferon; IL, interleukin; MCP-1, monocyte chemoattractant protein-1; TNF-α, tumor necrosis factor-α.
Results
Maternal age ranged from 18 to 43 years, maternal BMI ranged from 19.6 to 39 distributed as n = 10 in NW group; n = 8 in OW group; and n = 13 in OB group. As only preterm births were considered for the study, GA ranged from 19.6 to 36.9 with n = 10 in the EP-VP group and n = 21 in the MP group. Fifteen mothers were primiparous and 16 multiparous. Most common delivery type was cesarean section, and for sex at birth, 14 were females and 17 were males. When EP-VP group was compared with MP group only GA was significantly different in the EP-VP group than in the MP group (p = < 0.001), and mode of delivery in the EP-VP group was also significantly different (p = < 0.001) than the MP group (Table 3).
Characteristics of Women and Infants Included in the Study According to Prematurity Status (Extremely Preterm to Very Preterm and Moderately Preterm)
Data for all groups are shown as mean and SD or percentages (%). Data for preterm status are mean ± SD (range) or percentages (%). Statistical differences were calculated using unpaired t test and Mann–Whitney U-test; and square chi. Correlations in bold have p < 0.05.
BMI, body mass index; EP, extremely preterm; MP, moderately preterm; SD, standard deviation; VP, very preterm.
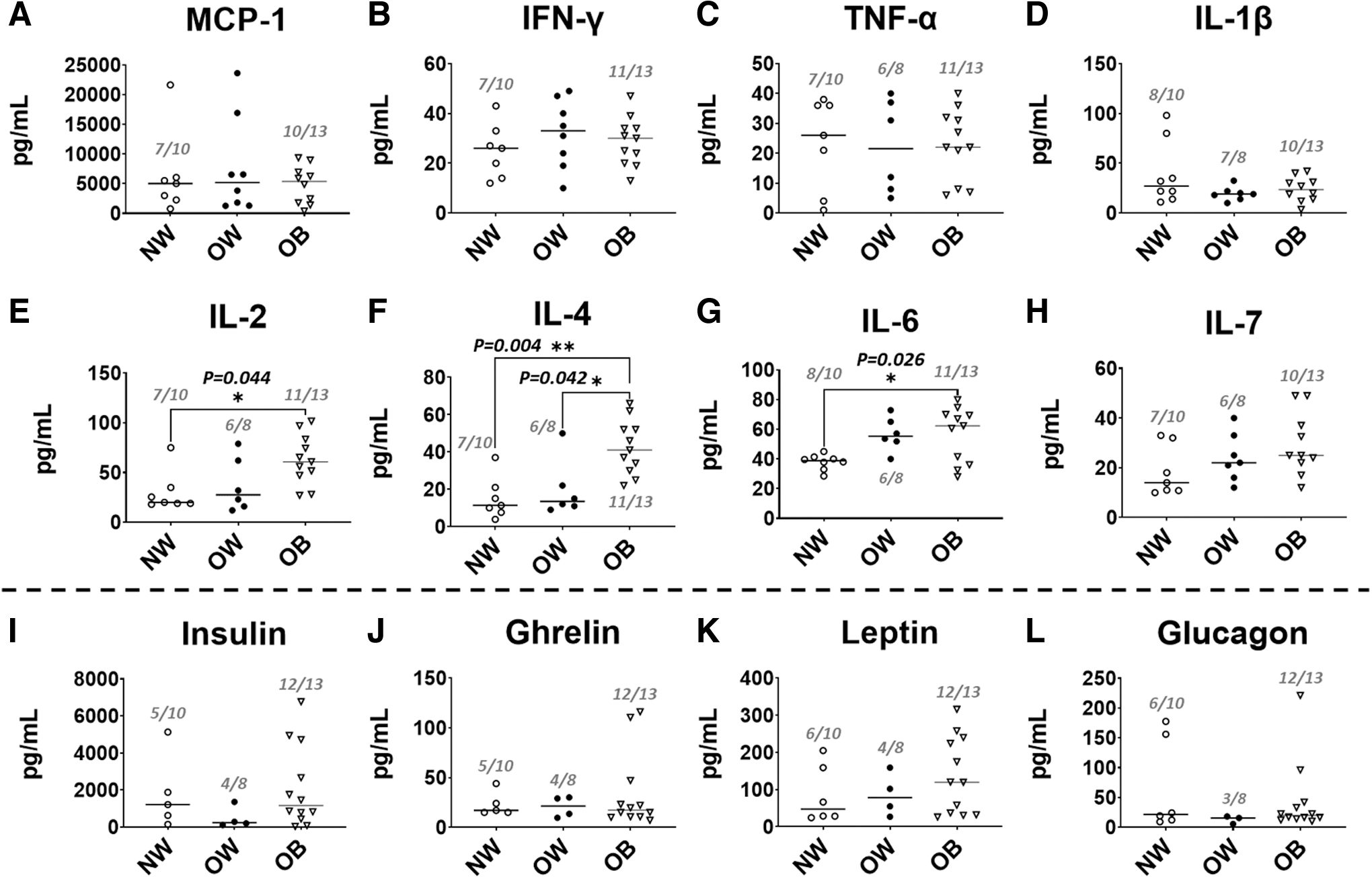
Cytokines IL-1β, IL-2, IL-4, IL-6, IL-7, MCP-1, IFN-γ, and TNF-α and hormones ghrelin, glucagon, insulin, and leptin levels in BM samples were compared with premature birth status (EP-VP and MP), sex at birth (female or male), parity status (Primipara versus Multipara), and maternal BMI status (NW, OW, and OB). We found a significant increase in TNF-α levels (p < 0.015) in the EP-VP group compared with the MP group (Fig. 1C). No significant changes in IL-1β, IL-2, IL-4, IL-6, IL-7, IFN-γ, and MCP-1 levels (Fig. 1A, B, D–H) were detected, nor in the levels of glucagon, ghrelin, insulin, and leptin when comparing EP-VP group with MP groups (Fig. 1I–L).

Cytokines and hormones in BM compared with preterm status.
Accordingly, when cytokine and hormone profiles were analyzed by parity status (primipara versus multipara) or infant sex (female versus male) no significant differences were detected. Notably, when cytokine and hormone profiles in BM were compared according to BMI status (NW, OW, OB), we found a significant increase in the levels of IL-2 in the NW versus OB group (uncorrected p = 0.015; corrected p = 0.044) (Fig. 2E). In addition, IL-4 levels increased in the BM of OB mothers compared to NW (uncorrected p = 0.001; corrected p = 0.004) and in OB compared to OW (uncorrected p = 0.014; corrected p = 0.042) (Fig. 2F). We found IL-6 accumulation in the BM of OB mothers compared to NW (uncorrected p = 0.009; corrected p = 0.026) (Fig. 2G). No significant changes in the BM profiles were found in the OB mothers compared to NW and OW for MCP-1, IFN-γ, TNF-α, IL-1β, and IL-7 levels (Fig. 2A–D, H), nor for insulin, ghrelin, leptin, and glucagon (Fig. 2I–L).
Cytokines and hormones in BM compared by maternal BMI.
When levels of prematurity were analyzed by maternal BMI, no significant differences were detected (Kruskal–Wallis test p = 0.975; Spearman's r = −0.04) (Table 2). In addition, correlations among cytokines and hormones with maternal factors were found. Maternal age was positively associated with IL-7 (r = 0.50, p = 0.015); maternal BMI correlated positively with IL-2 (r = 0.48, p = 0.017) and IL-4 (r = 0.66, p = < 0.001); and GA correlated negatively with TNF-α (r = −0.66, p = < 0.001) (Table 2).
We performed a multiple linear regression to establish the association between sex at birth (Male versus Female), BMI of the mother, and severity of the preterm birth to cytokine and hormone profiles in BM for a predictive model. According to our mathematical model, we tested several interactions between the cytokines and hormones in BM TNF-α, IFN-γ, IL2, IL4, IL6, IL7, IL1B, Ghrelin, Insulin, Glucagon, and Leptin (Table 1).
We predicted that TNF-α concentration in BM was displayed as the major interaction. Our multiple regression analysis demonstrated a negative interaction between higher maternal BMI and preterm birth in male babies that predicts concentration of TNF-α in BM. Finally, this multiple regression analysis displayed an adjusted R2 = 0.7117 with p = < 0.001. Correcting for mode of delivery resulted in a slight increase in the adjusted R2 = 0.750 with no significant change in the p-value (<0.001). However the predictor mode of delivery showed to be nonsignificant (p = 0.09987) (Table 1). Our model that considers maternal BMI, infant sex, and GA states that higher maternal BMI and less gestational weeks delivery are associated with TNF-α levels in BM of mothers bearing male babies (Fig. 3).
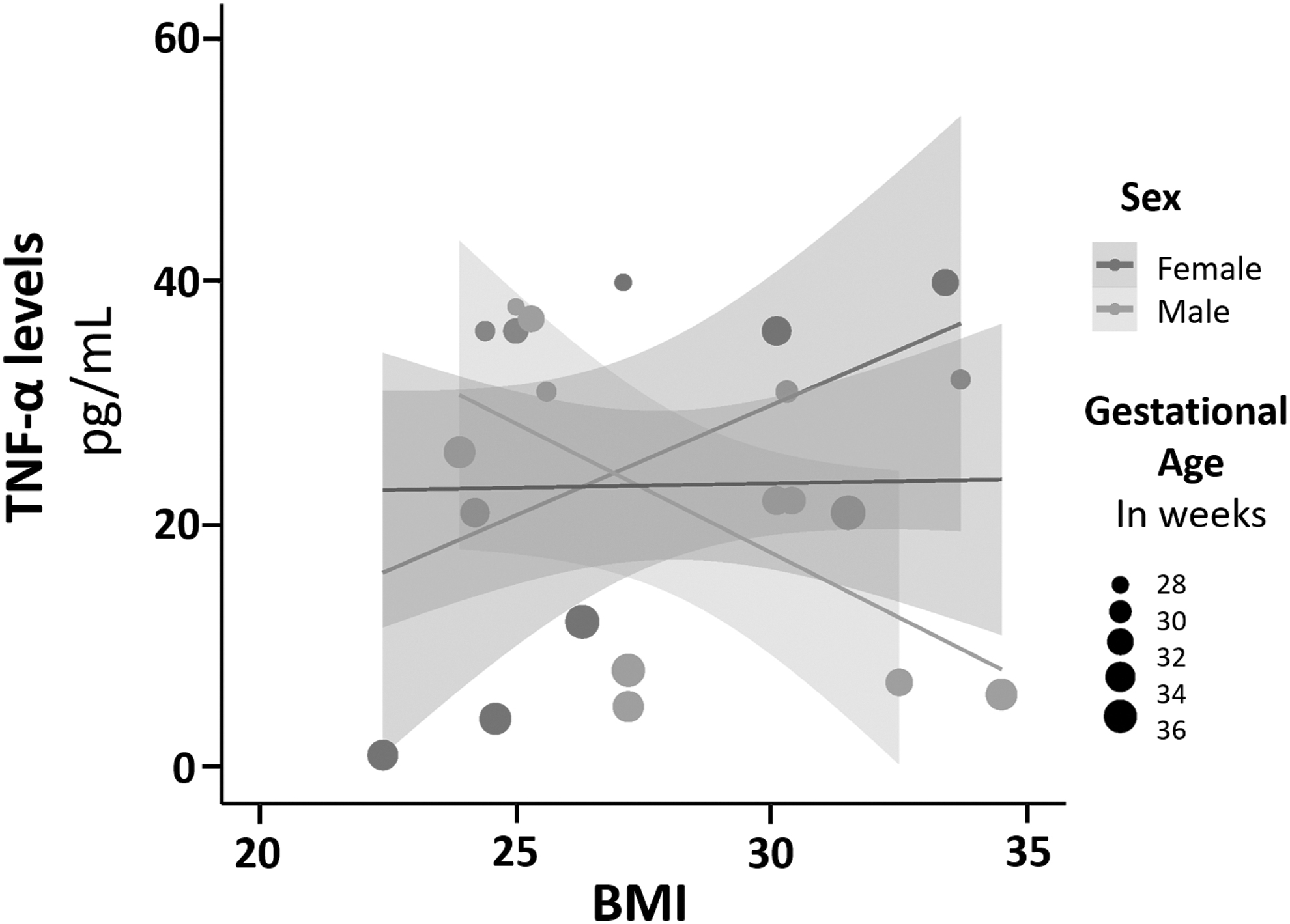
Higher maternal BMI and less gestational weeks predict TNF-α levels in milk of mothers bearing male babies; multiple linear regression analysis shows the interaction between infant sex at birth (female versus male), maternal BMI, preterm birth status expressed in weeks as GA and TNF-α. BMI, body mass index; GA, gestational age; TNF-α, tumor necrosis factor-α.
Discussion
We aimed to associate cytokines and hormone profiles in the BM of mothers with obesity or normal weight according to their BMI status before pregnancy in a cohort that only considered preterm infants. Using a multiple linear regression model, the interaction between the child's sex, maternal BMI, and preterm status to cytokine and hormone concentration in BM was explored. Our multiple linear regression model revealed that higher maternal BMI and higher prematurity are associated with TNF-α levels in the milk of women bearing male babies. Increased group size could improve our model for better predictions of TNF-α in BM. Multiplex analysis also revealed that the pro-inflammatory cytokine TNF-α has a positive association with increasing prematurity and that the pro (IL-2, IL-6) and anti (IL-4) inflammatory cytokines also showed positive association with maternal BMI. Bivariate correlation tests also identified a negative correlation between GA and TNF-α and positive correlations between maternal age and IL-7, maternal BMI and IL-2, and maternal BMI and IL-4.
Epidemiological studies have documented that premature births are increasing worldwide. 21 In the current study, we characterized the immune and hormonal profiles in BM of women with normal weight and obesity according to whether they had extremely to very preterm or moderately preterm deliveries. We found that major accumulation of TNF-α levels in the BM of mothers bearing male babies is dependent on higher maternal BMI and on less gestational week delivery. TNF-α is a pro-inflammatory cytokine with protective properties that does not cause inflammation in the highly susceptible neonate.9,22
Experimental evidence supporting the role of pro-inflammatory cytokine TNF-α in premature births is still under investigation and in some cases has been controversial, reporting different outcomes.7–9,22–24 Some research groups have reported no differences when comparing mature BM of term and preterm groups;22,24,25 whereas others have found negative association in premature BM compared with term milk. 8 Moreover, others have reported increased TNF-α in preterm milk but only compared to term BM analysis. 7 In our study a negative correlation between GA and TNF-a was identified. In addition, there is no consensus in premature grouping as authors define prematurity differently. In the study from Mehta and Petrova, there was only a single premature group from 28 to 32 weeks of GA 7 ; Castellote group defined preterm (30–37 GA) and very preterm group (<30 weeks GA) 22 ; O'Rourke group defined preterm as <35 weeks GA, 25 whereas Ramiro-Cortijo et al. 20238 and Ustundag et al. 20059 defined the group as <37 weeks GA and only Trend et al., 201624 used WHO premature groups.
Notably, in BM some authors reported that cesarean delivery, but not GA, was associated with the increase of TNF-α. 7 Contrasting to our study population, authors reported that up to 66.7% of the preterm mothers had cesarean delivery, whereas more than 90% women in our study had cesarean deliveries (Table 3). Other research groups did not consider birth mode in the analysis,9,22,25 and others did not find associations.8,24 When our multiple regression analysis was adjusted for mode of delivery, no significant differences were found likely due to our predominantly cesarean delivery cohort. Thus, a wider cohort with more balanced birth mode groups should be explored. According to previous studies, surgical stress from cesarean delivery can also increase TNF-α levels in BM; however, the TNF-α concentration decreases within the first 3 weeks. 26 As our BM was collected from postnatal day 21–30, it is unlikely that the surgical stress from cesarean section could relate to the increase in TNF-α from our results.
Also, additional reports documented that maternal BMI status for overweight and obese women in BM premature analysis was not considered to be associated with plasma cytokine levels.7–9,22,24,25 In all, a significant contribution of our current study was the inclusion of maternal BMI delivery as key predictors for TNF-α levels in BM. We propose that TNF-α increases in the very preterm group might potentially be considered as an adaptation to the neonate's prematurity status. In any case, additional causality analysis with bigger sample size is needed to validate this hypothesis, considering not only cesarean delivery groups but also extremely premature and term groups modulating immunologic outcomes in the offspring.
The effect of BMI on inflammatory systemic and central profiles has been reported by several authors.13,20,22,27–30 In our study we provided selective inflammatory signatures in the BM of women according to BMI. We found a significant increase in IL-2, IL-4, and IL-6 in BM that correlated with maternal BMI, and IL-2 and IL-4 also correlated positively with maternal BMI in Pearson's correlation test. However, these correlations failed when comparing with premature groups, parity status, or childbirth sex.
As obesity is a chronic low-grade inflammatory environment with presence of increased IL-2, 31 IL-6, 14 and IL-4,27,32 the increased IL-2, IL-4, and IL-6 in mature BM found in our study could be directly related to increased maternal BMI and premature status. Several reports confirmed the effect of obesity on IL-2, 31 IL-6, 14 and IL-4 in BM27,32; however, other authors reported contradicting evidence. For instance, IL-2 increased in BM from women with increased BMI where no preterm births were considered, 20 or a decrease in IL-6 levels when premature milk was compared with term milk; however, this study lacked validation and integration of BMI. 9 In addition, authors reported a negative correlation between IL-6 levels and BMI 20 or no associations for BMI and cytokine profile,13,29,30 with none of the aforementioned studies considering preterm groups. Another group found no associations in IL-6 for term milk in term or preterm groups 22 which is consistent with our results of no interaction between IL-6 and premature status; however, authors did not consider the effect of BMI on this outcome.
In addition, few studies linking obesity and IL-4 are currently available.20,27 A report found that IL-4 decreased in milk from women with high BMIs, 20 and another study showed increased IL-4 levels in diabetic population with overweight and obesity, 27 which is in agreement to our results that found IL-4 increase in high BMI maternal groups.
Based on this evidence, IL-2, IL-4, and IL-6 levels in BM have inconclusive reports as some studies only consider BMI status and other premature status, but none of them considered both. Maternal age and IL-7 were found to correlate positively; however, no other association with any other analysis for these variables was seen in our study; for instance, this association needs to be explored in future studies. We conceive that accumulative interaction of BMI and premature status may integrate a more realistic scenario of inflammatory profiles in BM.
Finally, metabolic hormones are important bioactive components in BM as they can mediate satiety in feeding infants. 33 We found no significative differences between preterm status, gestational status, childbirth sex status, or BMI status for insulin, ghrelin, leptin, and glucagon.
Insulin showed no differences when analyzed by maternal BMI groups; 30 however, a positive interaction between female birth sex and maternal BMI has been reported. 29 In addition, authors reported that obese mothers displayed higher hormone levels than normal weight mothers. 34 For the appetite suppressing hormone leptin, some groups have also found no correlation with maternal BMI and hormone levels, 34 whereas another group reported higher BM leptin in the NW group compared with higher BMI groups, 30 and others have reported positive correlation with maternal BMI 35 or with higher percentage of fat mass. 33 In fact, statistical differences found in the study of Enstad et al. 202135 could be explained by the adjustment for maternal race and postpartum days for milk collection.
Serum and BM comparisons of insulin and leptin and pro-inflammatory TNF-α and IL-6 cytokines with different maternal BMI groups have found that blood and BM levels are not always correlated. 30 In addition, no correlation in BM immune variations was found in a large international cohort study even after adjusting for race. 11 This evidence provides a rationale of obesity-dependent hormonal profile in BM, but still inconclusive evidence. More research is required to define a selective approach to tackle and modulate BM hormonal components.
Strengths that we identified in our study is the grouping of our severe premature cohort, GA, infant sex, and maternal BMI category which to our knowledge have not yet been explored. As limitations, we identified that a group of term infants could have been included for additional comparisons and that higher “n” values could provide greater understanding of how maternal and infant factors are interacting and thus enable a clearer overview of the analyzed maternal and infant factors and their impact on BM. In addition, in some cases we identified that not all hormones or cytokines could be detected through multiplex technology which has also been an issue detected by other groups when analyzing BM 22 or even when using similar enzymatic chemiluminescence technology. 36
Conclusion
Our study provides evidence suggesting that higher maternal BMI and less gestational weeks are associated with higher TNF-α levels in BM. Our results also suggest that this could be higher for women bearing male babies. In addition, we found that increasing maternal BMI status accumulates IL-2, IL4, and IL-6 levels in BM. Our study contrasts with previous research that has integrated non-Latin-American populations, and it highlights the importance of investigating how biological traits such as obesity and preterm status can impact the composition of BM in selective ethnic groups. A larger sample size would allow to predict associations between maternal BMI and gestational weeks on cytokine accumulation in BM.
Footnotes
Acknowledgments
The authors thank Dr. Juan Gerardo Neme Kuri for the support in the Hospital “Centro de Alta Especialidad Dr. Rafael Lucio” and to the Hospital Staff Dr. David Huerta Morales, Dr. Samantha Ponce Ramos, Psychologist Edith Nava Bustos, Nutritionist Nieves Mestizo González, Nutritionist Ana Carolina Espinoza Murrieta, and the Student Nancy Colorado Muñoz for the support in the data and BM sample collection process. The authors also thank M.S. Alejandra Arreola-Triana for her support on editing this article.
Authors' Contributions
The idea for the article was suggested by M.D.C-F., A.C-M., C.M-V., and R.V-C. Sample collection was performed by M.D.C-F. and R.V-C. Sample processing was performed by M.D.C-F., M.C-T., and R.O-L. Data analysis was performed by M.D.C-F., A.C-M., J.I.Z-L., and C.C-G. Multiplex sample kits were provided by C.M-V. and J.I.Z-L. Original draft was written by M.D.C-F. and A.C-M. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the CONAHCYT Posdoctoral Fellowship Program Estancias Posdoctorales por México 2022 to M.D.C-F. and by PAICYT 2022 to A.C-M.