
Abstract
Background:
It is well accepted that lactation consultant (LC) services can enhance the breastfeeding success in mother–infant dyads. However, despite such advantages, not all neonatal intensive care units (NICUs) offer LC services. The objective of this systematic review was to assess the available evidence on the effect of LC service on breastfeeding outcomes for mothers whose infants are in the NICU.
Methods:
The PRISMA Extension for Systematic Reviews were used to conduct this systematic review. The following databases: Embase, Medline, CINAHL, and Cochrane library were searched. An initial 464 studies were obtained. Duplicates and studies that did not fit the inclusion criteria were removed, leaving 30 full-text articles to review. Nineteen were further excluded after full-text review. A total of 11 studies were included. Due to the heterogeneity of the included studies, a meta-analysis could not be performed, instead a qualitative numerical summary was conducted.
Results:
Overall, 10/11 (90%) of studies observed a 6–31% increase in the number of infants who received mother’s own milk, and 11–27% in the number of infants who received direct breastfeeds associated with the implementation of LC services in the NICU. The two most common types of LC services studied included: i) multidisciplinary lactation support—described as a team-based approach that includes at least one LC and ii) designation of LC formal role in the NICU.
Conclusions:
This review highlights that having LC services in the NICU is vital for meeting the unique needs and enhancing breastfeeding outcomes for mothers whose infants are in the NICU.
Introduction
Mother’s own milk (MOM) is composed of factors tailored to meet the immunological, nutritional, and developmental needs of individual infants1,2 and is regarded as the optimal source of nutrition for all infants, in particular for those requiring neonatal intensive care.1,2 Although donor human milk is a good alternative when MOM is not sufficient or unavailable, it may lack some immunological factors because of the pasteurization process. Furthermore, formula is also an option when there is insufficient mother’s own milk; however, it lacks the bioactive components found in human milk.2,3 MOM, in comparison to formula, has been shown to decrease the rate of common medical complications in critically ill infants including late-onset sepsis, chronic lung disease, and necrotizing enterocolitis.2,3 These benefits can be further enhanced when MOM is provided directly to infants from the breast rather than expressed and given by bottle.3–5 Such findings form the basis of the World Health Organization statement that calls for exclusive breast milk for all infants for at least the first six months of life.1,2 Despite these well-known benefits, the rates of obtaining MOM and direct breastfeeding for infants who are in the neonatal intensive care unit (NICU) remain relatively low in comparison with infants in well-baby nurseries.1,6–9
There are a myriad of infant, mother, and environmental barriers to sustaining breast milk production and establishing direct breastfeeding while in the NICU.8,10,11 These infants must be fed via gastric tube until they are medically stable. 12 As a result, mothers rely on breast pumps to initiate and maintain milk supply for weeks or months before the infant can suckle at the breast. 12 Prolonged pumping is not only taxing for mothers, but they may not be able to produce sufficient quantities of MOM to meet their infant’s nutrient needs, consequently leading to early cessation of pumping or breastfeeding. 12 Furthermore, obstetrical and pre-existing maternal illness (e.g., depression and anxiety, and gestational diabetes mellitus), combined with the stress of having their infant in the NICU, can further aggravate the situation and make direct breastfeeding the infant a very demanding task resulting in early cessation of direct breastfeeding within the first month of initiation. 13 The NICU environment, particularly the open bay units, entails mothers are physically separated from their infants and lack of privacy, which can negatively influence breastfeeding outcomes.14,15 These challenges necessitate that mothers and infants require additional support to engage in and sustain breastfeeding practices during their stay in the NICU.
Lactation consultants (LC) provide care to mothers and infants following birth by providing support services to encourage both breast milk production and direct breastfeeding.16,17 A recent Cochrane systematic review of 52 studies on breastfeeding support for mother’s with usual maternity care (56,451 mother–infant pairs) from 21 countries has shown that LC support increases the duration and exclusivity of breastfeeding. 16 These results are not applicable to mothers whose infants require neonatal care. The NICU provides unique challenges to the mother–infant dyad.18–20 Mothers require specific lactation support to optimize their breast milk production and direct breastfeeding initiation and duration. It is well accepted that LC services are key for optimizing both MOM production and direct breastfeeding opportunities in mother–infant dyads during the NICU stay because they are able to meet the unique needs of this population.16,21 Despite such advantages, less than half of NICUs in the United States offer LC services. 22 Furthermore, in most NICUs who have LC(s), the position is often shared with postpartum units, which often results in less time for the LC(s) to provide adequate support.22–25 In units with partial or no LC services, it becomes the expectation that the bedside nurses, neonatologist, or occupational therapists provide lactation counseling to families. Unless the hospital has a Baby-Friendly Hospital Initiative (BFHI) designation, which ensures all team members are trained and proficient in breastfeeding support, their primary professional duties often take precedence over providing lactation counseling.9,22 Elucidating LC services and positive influences on the provision of MOM and direct breastfeeds is important for further understanding the role of LC services in this critical setting and for informing the implementation of LC services within NICUs.
To the authors’ knowledge, there have been very limited reviews that assess the available evidence on the beneficial impact of LC services in the NICU, with the exception of the study by Mercado and colleagues (2019). 25 They identified that an NICU-designated LC improves the delivery of MOM in very low birth weight infants. 25 However, their review was a practice brief, with a focus on very low birth weight infants and the LCs’ role in the provision of MOM, but did not direct breastfeeds. Hence, results cannot be generalized to all infants who are in the NICU setting. Therefore, the purpose of this systematic review was to assess the available evidence on the effect of LC services on breastfeeding outcomes, in particular, the provision of MOM and direct breastfeeds in the NICU. A systematic review method was selected because it is a formal methodological approach to answer a research question. It is used to synthesize all available evidence and evaluate the quality of the evidence to make recommendations for practice. 26 The findings from this systematic review will provide clinicians and researchers with a comprehensive understanding of the effectiveness of LC services to facilitate achievement of MOM provision and direct breastfeeding experiences for the mother–infant dyads in the NICU, and to advocate further for the implementation of LC services across all NICUs.
Methods
Study Design
A systematic review was performed using the Preferred Reporting items for Systematic Reviews and Meta-Analyses Protocol (PRISMA) as a guide. 26
Stage 1: Research question
The primary research question for this systematic review was: What is the impact of LC services for mothers and their newborns in the NICU on breastfeeding outcomes, including provision of MOM and direct breastfeeds? The secondary questions included: What is the nature (type) of the LC service offered? And, what are the knowledge gaps in this area? These questions were used to guide the search and obtain information on what has been published in the existing literature.
Stage 2: Eligibility Criteria
To be included in this review, articles must have met the following inclusion criteria: 1) address LC services such as implementation of designated NICU LC, multidisciplinary lactation support, or any lactation support in the NICU, 2) evaluate the impact of LC service in the NICU breastfeeding outcomes, including provision of MOM and/or direct breastfeeds, and 3) keywords (or synonyms) must be identified in the title or abstract. Articles were excluded if the studies: 1) were not from a peer-reviewed journal, 2) were scoping or systematic reviews, 3) focused on nurses’ experiences with LC support; 4) mothers were unable to provide breast milk (e.g., HIV, drug use, chemotherapy), and 4) focused on feeding equipment, e.g., type of nipple shield or breastfeeding pump.
Stage 3: Information Source
The search strategy was developed by the three authors (S.F., S.W., and P.P.) using PRISMA guidelines and in consultation with a Health Sciences librarian. A comprehensive search of four databases, EMBASE, MEDLINE, CINAHL, and COCHRANE, was conducted. The limits applied included: 1) human, 2) infant, newborn, 3) English language, and 4) publications beyond the year 2000. The MeSH and key search terms used included: lactation consultant, or breastfeed* (*indicates include all studies where the MeSH term begins with “breastfeed” regardless of its ending), or lactation, AND human milk or breast milk, AND neonatal intensive care unit, or newborn intensive care unit, or NICU. The words newborns or infants were not included because it was assumed in the literature that all NICU patients are infants and/or their mothers. All of these key search terms and their extensions were used for each of the databases. The reference list generated was cross-referenced between each database to confirm that the search results accurately represented the research questions.
Stage 4: Search strategy
Articles were independently screened for inclusion by two trained assessors (S.W. and P.P.) at each stage of the PRISMA framework. 26 Any discrepancies were resolved with a third researcher (S.F.). Figure 1 includes a flow chart describing the study selection process. The titles and abstracts were first screened separately for relevance according to the above inclusion and exclusion criteria. A full-text review was then conducted by the two assessors. For the full-text review, a data abstraction sheet was created to ensure both assessors were abstracting the same information.
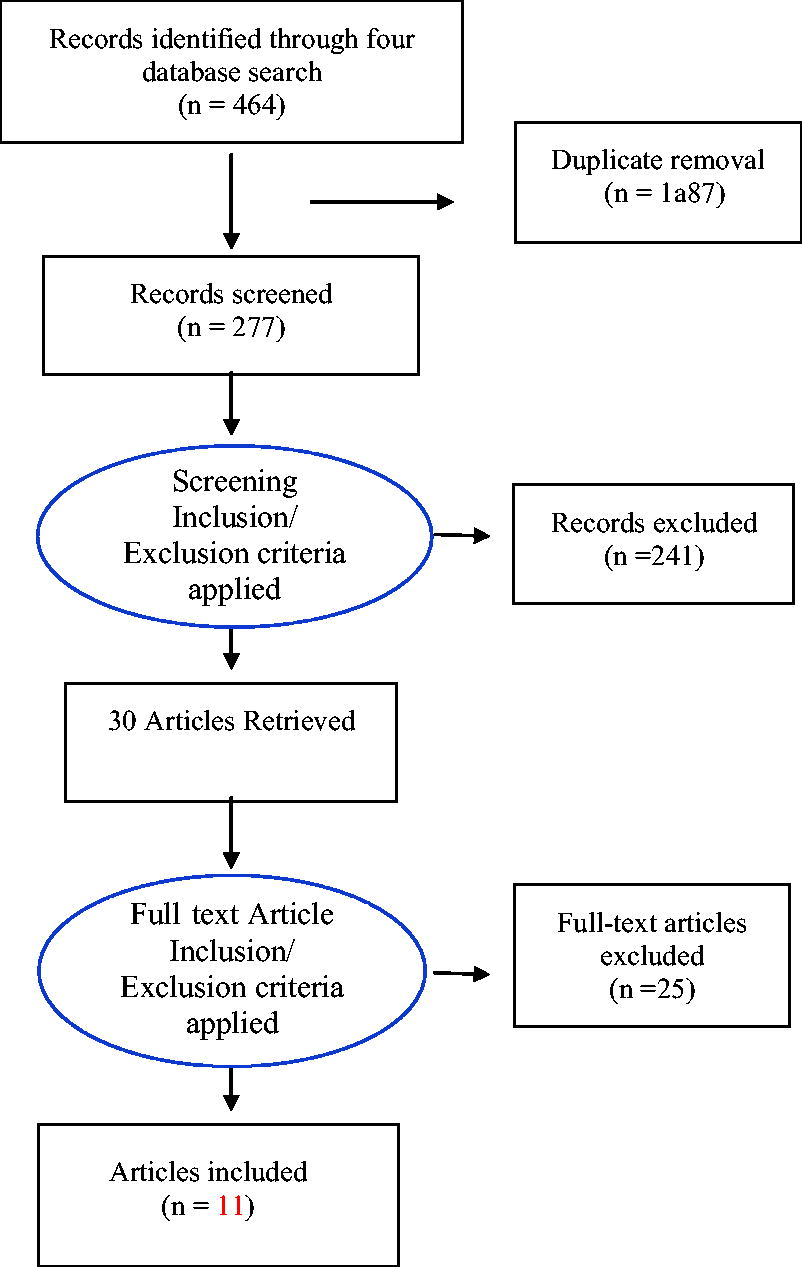
Flow chart describing the study election process.
Stage 5: Study records and data item collection
The following data were abstracted and compared for each article included: Year of publication, aim, study design and level of evidence, setting and population, type of LC service, and MOM and direct breastfeeds outcomes and results. The level of evidence was determined using The Oxford Centre for Evidence-Based Medicine System, 27 where level 1 is the highest level of evidence and 5 is the lowest level of evidence. Two authors (P.P. and S.W.) participated in data extraction and crossed checked each other, and any inconsistencies were resolved by the third researcher (S.F.). Each assessor was trained by the senior author (S.F.) to complete the data abstraction sheet to ascertain that the appropriate data were collected by the two assessors.
Stage 6: Outcome and prioritization
The outcomes included: (a) provision of MOM outcome defined as the number of infants who received any MOM during their hospital stay and (b) direct breastfeed outcome described as the number of infants who received direct breastfeeds during their stay in the NICU. The included articles were initially assessed for the impact of LC services on the above two breastfeeding outcomes. Then by differentiating the nature (type) of LC services investigated.
Stage 7: Risk of bias
The ROBINS-I tool was used to assess the risk of bias of the included studies. 28 The ROBINS-I tool was selected because it evaluates the risk of bias for nonrandomized studies. 28 It evaluates seven domains for risk, including biases because of confounding, in the selection of participants, measurement of intervention, departures from intended intervention, missing data, measurement of outcomes, and selection of the reported results. Each domain was assigned a risk of bias by two assessors using the following options: low risk, moderate risk, serious risk, critical risk, or not enough information. 28 A final judgment with the same options was made for the entire study based on the findings from each domain. Discrepancies were discussed with a third reviewer until a consensus was reached.
Results
Figure 1 illustrates the search flow for selecting articles. The article search was conducted from June 2022 to January 2023 and generated a total of 464 articles from the four electronic databases. After removing 187 duplicates, 277 article titles and abstracts were screened independently by two assessors for relevance according to the inclusion and exclusion criteria. Thirty articles were retrieved for full-text reading. Of these, 19 articles were excluded because they did not meet the inclusion criteria for this systematic review. A total of 11 articles were included in the final data extraction.22,29–38
Table 1 provides a summary of all the studies included in this systematic review. All the articles included in this review were published in North America, specifically nine from the United States of America and two from Canada. Population samples included mothers and infants who were in level II or higher NICUs, and sample sizes ranged from 100 to 7581 participants. There was a variety of research designs and levels of evidence across the included studies. Specifically, there was one randomized clinical trial (level 1b), 38 four pre- and poststudy designs (level 2c),29–32 four retrospective cross-sectional studies (level 2a),33–36 one prospective cross-sectional study (level 2a), 37 and one case–control study (level 4). 36 Due to the heterogeneity of the included studies, a meta-analysis could not be performed; instead a qualitative numerical summary was conducted. The overall risk of bias and risk of bias for each domain are presented in Table 2. Among the studies analyzed, the majority exhibited an overall low risk of bias,22,29–35,37,38 with only one study demonstrating a moderate risk. 36 The prevalent bias observed across the studies was related to missing data, as none of the studies provided information on how they addressed this issue.
Summary of all Included Studies
CI, confidence interval; IBCLC, International Board Certified Lactation Consultant; LC, lactation consultant; NICU, neonatal intensive care unit; MOM, mother’s own milk; NS, not significant; OR, odds ratio.
Risk of Bias in Nonrandomized Studies of Intervention Results
Low, low risk; Mod, moderate risk; SR, serious risk; CR, critical risk; NI, not enough information.
Overall, 10/11 (91%) of the studies observed an improvement in the number of infants who received MOM and direct breastfeeds during their NICU stay associated with LC service(s) (Table 1).22,29–37 Specifically, six studies assessed the impact of LC services on provision of MOM, and they all found an increase from 6% to 31% in the number of infants who received MOM after the implementation of LC services,29,31–33,35 or a direct positive correlation with LC services and MOM provision.33,34 Three studies assessed the impact of LC services on direct breastfeeding opportunity only. Of these, two studies found an increase (27%) in the number of infants who received direct breastfeeds associated with the implementation of LC service in the NICU.36–38 Two studies assessed the impact of LC services on both outcomes,22,30 and one found a 0.2 mean increase in direct breastfeeds only, 22 and the other found a 10% and 11% increase in provision of MOM and direct breastfeeds, respectively. 30
Upon review of the included articles, the authors identified two types of LC services being offered. These were multidisciplinary lactation support and designation of LC formal role in the NICU. Multidisciplinary lactation support is described as a team-based approach to support lactation in the NICU. This team-based approach includes at least one LC and other members of the neonatal team and they are involved in daily or weekly lactation rounds, providing direct bedside lactation support to mothers, e.g., assessing infant’s latch on the breast, provision of counseling sessions, and/or education to mothers on various breastfeeding topics such as preventing mastitis, pumping, and holding positions. Designation of lactation consult formal role in the NICU includes a proactive-care model of service where LC services are part of standard care (i.e., direct referral to an LC), mothers receive a lactation consultation within 24 hours to 72 hours of NICU admission, individualized breastfeeding assessment and intervention provided, education and support to families given by LC only, and LC attends medical rounds daily. Table 3 provides a synthesis of studies by type of LC services and findings. Two of the included studies, Bixby et al., 2016, and Oza-Frank et al., 2013, assessed the impact of multidisciplinary LC service type. Both studies used a pre- and poststudy design (level of evidence of 2c) and observed an increase in the provision of MOM and an increase in direct breastfeeds in their participants. The nine remaining studies assessed the impact of a designed LC formal role in the NICU. The study by Pinelli et al., 2001, was the only randomized clinical trial (level of evidence of 1b), and it did not reveal a significant difference in direct breastfeeding outcomes. Five studies by Hoban et al., 2022, Mercado et al., 2019, Gonzales et al., 2003, Castrucci et al., 2007, Frank et al., 2014, and Dweck et al., 2008, which conducted pre- and poststudy design (level 2c) or case–control (level 4) studies observed an increase in MOM and direct breastfeeds. Three studies by Gharib et al., 2018, Sankar et al., 2022, and Lessen and Crivelli-Kovach, 2007, performed an association analysis and found a positive relation between the implementation of a formal designated NICU LC with MOM and direct breastfeeds.
Synthesis by Type of Intervention Provided
√ indicates the type of LC service assessed within study, + indicates that the study found beneficial effect on the breastfeeding outcome, − indicates that the study did not find a beneficial effect on the breastfeeding outcome.
DBP, direct breast feeds; MOM, mother’s own milk; NICU, neonatal intensive care unit.
Discussion
There is consensus within the literature that LC services have a positive influence on promoting and optimizing breastfeeding outcomes in mother–infant dyads.16,33,39 In spite of the known benefits, the practice of providing LC services in NICUs is not standard.16,17 Elucidating the impact of LC services on the provision of MOM and direct breastfeeds is important for further understanding the vital role of LC services in this critical setting and for informing the implementation of LCs services within NICUs. Hence, the purpose of this systematic review was to evaluate the evidence on the effectiveness of LC services in enhancing mother–infant breastfeeding outcomes in the NICU.
The available evidence included in this systematic review supports the inclusion of LC services in enhancing breastfeeding outcomes of the mother–infant dyad who are in the NICU. All but one study included in this review observed an improvement in the provision of MOM and/or increased direct breastfeeds during the NICU stay associated with LC services. The study by Pinelli al., 2001, was the only randomized clinical trial with a high level of evidence (1b), but it did not reveal a significant difference in direct breastfeeding outcome between infants who received a supplementary structured breastfeeding counseling by an LC and those who received conventional breastfeeding support by neonatal staff. The lack of significant difference in this study may be because the other health professionals were well trained in lactation support and thus were able to offer services analogous to the LCs. In addition, this finding may be attributed to the lack of blinding of the neonatal staff, which may have inadvertently influenced their behavior toward breastfeeding support, and in turn biased the results. In addition, the studies that demonstrated positive breastfeeding outcomes, specifically increased MOM provision and direct breastfeeds with LC services, included four pre- and poststudy designs (level 2c),29–32 four retrospective cross-sectional studies (level 2a),33–36 one prospective cross-sectional study (level 2a), 37 and one case–control study (level 4). 36 It is understood that the lack of randomized clinical trials and low level of evidence studies limit the strength of generalizable recommendations, and thus larger multicenter prospective cohort studies are needed in this area to affirm results. However, the known evidence that LC services have positive impact on breastfeeding outcomes in full-term, 16 alongside with findings from this systematic review, warrants the implementation of LC services in NICUs.
There were two types of LC services identified in this review. These include a multidisciplinary lactation support and designation of lactation consult formal role in the NICU. The multidisciplinary team-based lactation support that involved at least one LC and other members of the neonatal team to provide direct hands-on intervention, counseling sessions and/or education to families. The designation of lactation consult formal role in the NICU included a proactive-care model service where lactation services are part of routine standard care (i.e., direct referral to an LC) along with provision of individualized breastfeeding assessment and intervention within 24 hours to 72 hours of NICU admission. Methodological differences across studies preclude the provision of specific recommendations on what type of LC service NICUs should offer. More specifically, each included study assessed a variation of the two aforementioned types of LC services, in different levels of NICU care, and used different outcome measures, which makes it difficult to abstract and/or quantify more precise information, such as the exact number of hours of interaction between LC and mothers’ yields to positive breastfeeding outcomes, or whether a sole designated formal LC versus multidisciplinary team-based LC optimizes breastfeeding outcomes. However, irrespective of the type of LC service offered, a key tenant to improving breastfeeding outcomes in the NICU is having some form of LC service for mothers.
A common reason for not offering LC services in the NICU is associated with organizational financial constraints and lack of immediate financial benefit of their investment. 22 However, LCs have the potential to indirectly impact health care costs. Based on the appraisal of current evidence in this review, LC services can enhance the proportion of infants who receive MOM and direct breastfeeds in the NICU. The benefits associated with increased human milk consumption are associated with decreased total parental nutrition duration and central lines due to improved tolerance of human milk.2,3 Furthermore, human milk decreases the occurrence of severe neonatal medical conditions such as sepsis, necrotizing enterocolitis, and chronic lung disease.2,3 Hence, the improved breastfeeding outcomes may reduce the occurrence of neonatal morbidities associated, and thus indirectly reduce associated costs. Moreover, donor human milk is often provided to infants as a strategy to reduce neonatal morbidity. However, there are costs of purchasing, maintaining, and administering donor human milk diets, which can be significantly reduced if infants receive all or more of MOM. 22 Taken together, LCs can offer a significant return on investment by decreasing overall common health care costs associated with infants in the NICU. Future research should focus on identification of specific approaches to promote and optimize breastfeeding outcomes in this highly vulnerable population.
This systematic review has some limitations. A search of the grey literature was not conducted, which could have led to missed studies. However, there was an intentional selection of only peer-reviewed studies to increase the rigor of the results. The review generated single institution in North America only which limits the generalizability of results. Further, all but one study indicated if they were not a BFHI-designated institution. The lack of such information may bias findings. A large multinational study with an indication of BFHI designated institutions is needed to confirm these results. Methodological differences across studies impede upon precise information abstraction and/or quantification to make specific clinical recommendations. However, this review identified that a having LC services in the NICU is a key factor in improving breastfeeding outcomes in infant-mother dyads during their NICU stay.
Conclusion
It is well established that human milk is the optimal source of nutrition for infants. Infants who require neonatal intensive care face distinctive challenges necessitating specialized strategies for providing optimal nutrition. This review reveals that LC services in the NICU are vital for meeting the unique needs and enhancing the provision of MOM and direct breastfeeding rates for mothers and their newborns who are in the NICU.
Footnotes
Authors’ Contributions
S.W. and P.P.: contributed to the search strategy, data collection and analysis, and writing of the manuscript. S.F.: contributed to the conceptualization of the study, data analysis, and writing of the manuscript.
Ethical Approval
The study has been approved by Queens’s University Health Science Research Ethics Board.
Clinical Trial Registration
Not applicable.
Preprint Disclosure
The work has not been published before and is not under consideration by another publisher.
Disclosure Statement
S.W., P.P., and S.F. have no competing interests to declare.
Funding Information
The authors have no funding to disclose.