
Abstract
Introduction:
Despite known benefits of breastfeeding, including prevention against infections for infants, in the presence of numerous barriers, less than half of infants in high-income countries breastfeed for 6 months. One potential barrier to breastfeeding is birth by cesarean section (C-Section), which can invoke long-term difficulties. However, our structured literature review found that existing empirical research does not fully elucidate this relationship due to differences in operationalization of C-section and breastfeeding, omission of important confounders, and failure to exclude those who did not initiate breastfeeding (or use time-to-event analyses). In this article, we attempt to overcome these limitations.
Methods:
We analyzed data from 14,414 mother-infant dyads enrolled in the United Kingdom-based prospective Millennium Cohort Study, beginning in 2001. Using multivariable logistic regression, we examined the association between mode of birth (vaginal, emergency C-section, and elective C-section) and likelihood of breastfeeding initiation. We then applied adjusted Accelerated Failure Time survival models to examine the associations between mode of birth and duration of any and exclusive breastfeeding.
Results:
Those with planned (but not emergency) C-section were less likely to initiate breastfeeding (odds ratio: 0.84, 95% confidence interval [CI]: 0.71–0.99) relative to vaginal births. However, those with either planned or unplanned C-section discontinued both any and exclusive breastfeeding sooner than vaginal births. This effect was more pronounced for those with planned C-section (time ratio [TR]: 0.75, 95% CI: 0.64–0.89) than unplanned C-section (TR: 0.85, 95% CI: 0.74, 0.97) compared with vaginal births.
Conclusions:
Through application of rigorous methods, this study provides compelling evidence that breastfeeding duration may be impeded by C-section birth. The findings suggest that additional support for mothers who intend to breastfeed and have a C-section birth may be warranted.
Introduction
Despite known benefits of breastfeeding, including infant protection against infection, less than half of infants in high-income countries and only one third of infants in the United Kingdom are breastfeeding by 6 months of age. 1 This may be owed to a panoply of barriers related to the birth (e.g., gestational age), the individual (e.g., body mass index [BMI], mental health), social influences (e.g., family, friends), and institutions (e.g., maternity leave policies).2–8 While much is known about these factors, the association between mode of birth and duration of breastfeeding warrants further inquiry.
In particular, beyond the short-term impact of cesarean section (C-section) birth on breastfeeding, as evidenced by lower milk intake and greater weight loss among babies born through C-section,9,10 important methodologic shortcomings endemic in the literature have rendered the association between C-section and long-term (i.e., duration of) breastfeeding less clear. Below we present a structured review of the literature, demonstrate an analysis that resolves these methodological issues, and report findings from the largest and most detailed study of mode of birth and breastfeeding duration conducted to date.
The reasons for, process, and sequelae of C-section can impact early breastfeeding, which may have lasting consequences. Complications that indicate C-section, for example, preterm premature rupture of membranes resulting in early gestational age at birth, may affect the ability to breastfeed.11–13 The physical removal of the baby from the point of incision can pressure cranial nerves that can indirectly impact sucking, swallowing, and, consequently, milk intake. 14 C-section may inhibit the surge in hormones during late-stage parturition, which promote infant bonding, stimulate milk production, and regulate the alertness necessary for breastfeeding initiation.15,16 Stress hormones released during emergency C-section may also impede breastfeeding.17,18
Furthermore, mother-infant separation or absence of immediate skin-to-skin contact after C-section may delay initiation of breastfeeding19,20 and continue to impede hormonal processes that facilitate early breastfeeding.15,16 Consequences of delayed initiation of breastfeeding include lower milk volume 5 days after breastfeeding and delayed lactogenesis stage II, as well as shorter breastfeeding duration.21–23 Lastly, pain and exhaustion resulting from the surgery can also limit mobility and hamper a mother's ability to feed frequently.17,24 These challenges in early breastfeeding reduce the removal of milk from the glands, influencing the ability to stimulate future milk production,17,24 and possibly lead to long-term difficulties in breastfeeding.
The association between C-section and long-term breastfeeding outcomes is less clear. A seminal meta-analysis conducted with data from 31 countries documented no association between mode of birth and either partial or exclusive breastfeeding at 6 months among the subset of studies that restricted their analysis to women initiating breastfeeding. 13 Other review articles and meta-analyses focused on specific regions or countries have come to different conclusions,25–27 with relationships that differ across populations with different cultural norms and health systems' support for breastfeeding. 28
There are four important methodologic considerations when examining the relationship between mode of birth and breastfeeding duration. First, to inform potential physiological influences on breastfeeding, studies must differentiate between types of C-section. To estimate the net effect of the procedure itself, it is necessary to parse out the confounding effects of (1) underlying preferences for a planned C-section, (2) disruption of hormonal processes of labor that occur in planned C-section (prelabor or pre-late-stage labor), and (3) complications that may indicate an emergency C-section, all of which correlate with intent or ability to breastfeed. While these preferences and complications often remain unmeasured, stratifying the analyses by the type of C-section reduces the risk of confounding by these underlying factors. Contrasting differences in breastfeeding practices by the type of C-section can help elucidate difficulties in maintaining exclusive breastfeeding for C-section-born children, preferences for partial breastfeeding, or complete cessation.
Second, analyses must account for the confounding effect of early breastfeeding on the relationship between C-section birth and breastfeeding duration. There may be underlying preferences and intentions that correlate with both having a planned C-section and breastfeeding initiation. This is evidenced by lower rates of initiation among those delivering by C-section, especially planned C-section.3,11–13,29,30 However, previous studies have not consistently excluded those who never initiated breastfeeding when examining binary outcome measures of duration (e.g., any breastfeeding at 6 months). 13
The confounding effects of intent can be reduced either by restricting the sample to those who initiated breastfeeding (when conducting logistic regression analyses of breastfeeding at a given time), or by conducting a time-to-event analysis. Preferences and intentions, while often unmeasured, can also be probed by comparing differences between emergency or planned C-section. Although data for this study were collected 20 years before this analysis, they hold important value in that at this time in United Kingdom, C-sections were only performed for medical necessity and not for maternal request 8 ; as such, the confounding effects of maternal preference are likely minimized. Third, beyond demographic variables, studies must account for health-related confounders (importantly, BMI, maternal smoking, and gestational age at birth11,12,31).
Fourth, studies must examine both exclusive and partial breastfeeding, using more sensitive measures of cessation than dichotomized outcomes. Contrasting differences in breastfeeding practices may elucidate difficulties in maintaining exclusive breastfeeding for C-section-born children, preferences for partial breastfeeding, or complete cessation. Relatedly, it is most informative to move beyond dichotomous outcomes of breastfeeding duration that are commonly used (e.g., breastfeeding at 12 weeks) to a time-to-event analysis.
We conducted a structured review to identify quantitative, multivariable time-to-event studies that examined the relationship between C-section and breastfeeding duration in high-resource settings through PubMed (January 2000 to June 2022). Figure 1 presents the search strategy, inclusion and exclusion criteria, and search terms. Among the 87 articles that met our criteria for full text review, we found considerable heterogeneity in the parameterization of the outcome (discrete or binary/categorical; exclusive or any breastfeeding; and time after birth examined), methods applied, and inclusion of important confounders. Only three articles11,29,32 considered all the methodological issues outlined above and differentiated by type of C-section, each with different conclusions (Table 1).
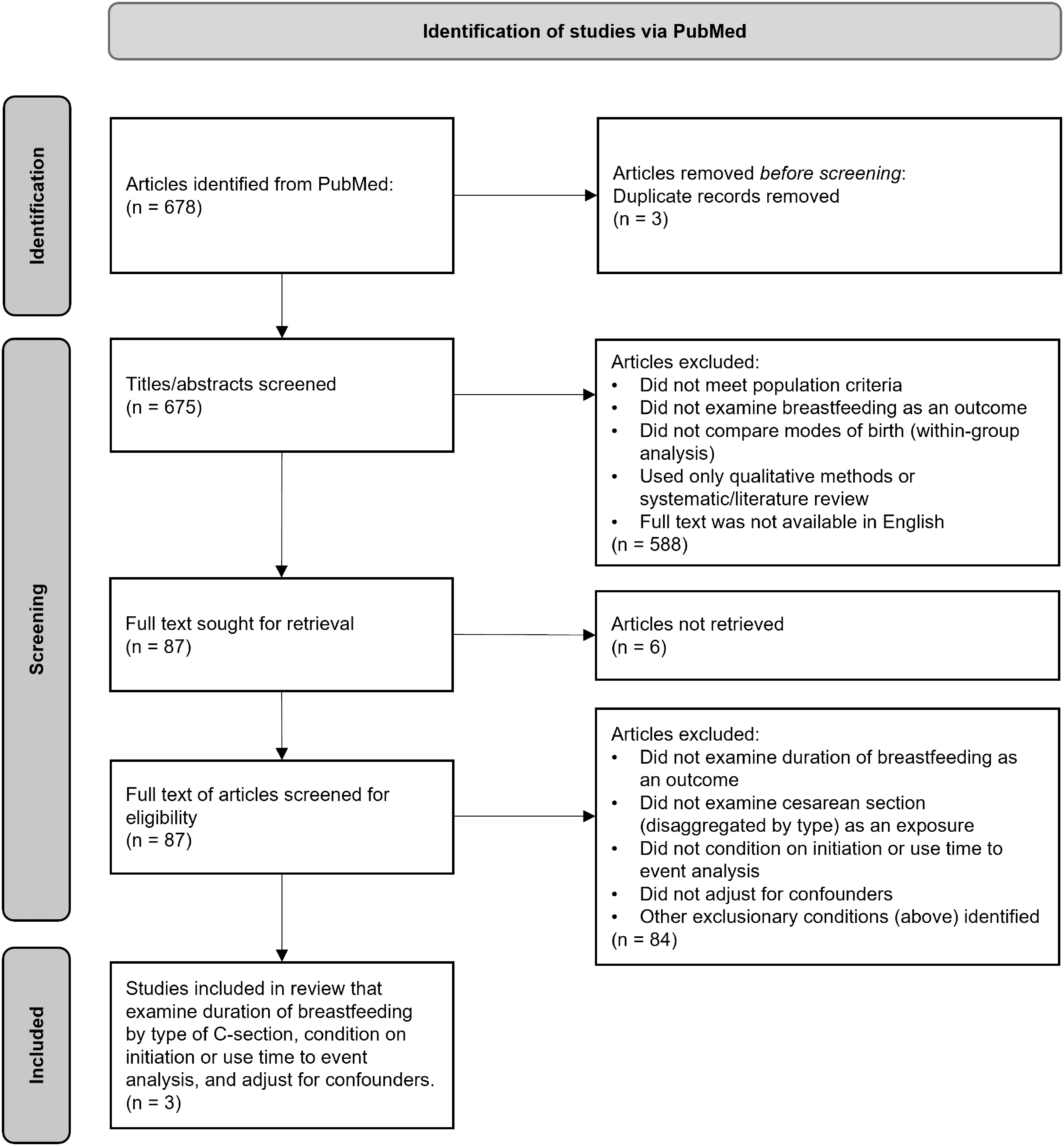
Flow diagram for structured literature review for articles published between January 2000 and June 30, 2022. The search terms included the following: (“breastfe*”[Title]) OR (“breast-fe*”[Title]) OR (“breast fe*”[Title]) AND (cesarean[Title/Abstract] OR caesarean[Title/Abstract] OR “mode of delivery”[Title/Abstract] OR “mode of birth”[Title/Abstract] OR “method of delivery”[Title/Abstract] OR “method of birth”[Title/Abstract] OR “type of birth”[Title/Abstract] OR “type of delivery”[Title/Abstract] OR “surgical birth”[Title/Abstract] OR “surgical delivery”[Title/Abstract]).
Key Studies Identified by the Structured Literature Review
ABF, any breastfeeding; BMI, body mass index; C-section, cesarean section.
Given these methodological limitations, differences in operationalization of breastfeeding outcomes, and dissimilarity of findings, the relationships between C-section and breastfeeding duration remain unclear. Thus, in our article, we estimate the association between mode of birth and (1) breastfeeding initiation, (2) duration of any breastfeeding, and (3) exclusive breastfeeding, comparing any C-section, planned C-section, or unplanned C-section to vaginal birth using a time-to-event analysis.
Materials and Methods
Data
We analyzed data from the first wave of Millennium Cohort Study (MCS, 2000–2002), conducted in United Kingdom among parents with a child born ∼9 months before (available at https://cls.ucl.ac.uk). 33 MCS used a multistage cluster sampling design with oversampling of disadvantaged and ethnic minority residents. 33 Among eligible households, the response rate was 82% (N = 18,540 families), including 18,246 families with singleton births and mothers completing an interview. Of those, 15,832 children had a known gestational age, were born at ≥37 weeks, and did not receive special or intensive care after birth, among whom 14,505 had information on maternal weight and height before pregnancy. Our analytic sample included 14,414 singleton babies and their mothers. We also examined a subsample (n = 9,708) of mother-baby dyads who ever attempted to breastfeed.
Measures
We examined three outcomes among babies 6–12 months of age: (1) Whether the mother ever attempted to initiate breastfeeding (yes/no); (2) duration of any breastfeeding for up to 6 months; and (3) duration of exclusive breastfeeding. We assessed duration of any breastfeeding based on responses to questions about how old the baby was when the mother last fed them breast milk.
We converted responses in discrete categories (days, weeks, and months) to continuous by first standardizing responses in days and then assigning the midpoint of each discrete interval, a method that has been used in analysis of time to initiation of breastfeeding. 20 Duration of exclusive breastfeeding variable was created similar to any breastfeeding; yet, if a woman fed her baby formula or solids before she last fed her baby breast milk, the age of first provision of either formula or solids replaced the time for age of last provision of breast milk.
Mode of birth was categorized as vaginal, planned C-section, and emergency C-section. Informed by our structured review, we constructed a directed acyclic graph (Fig. 2) to select confounders for inclusion in the regression models.
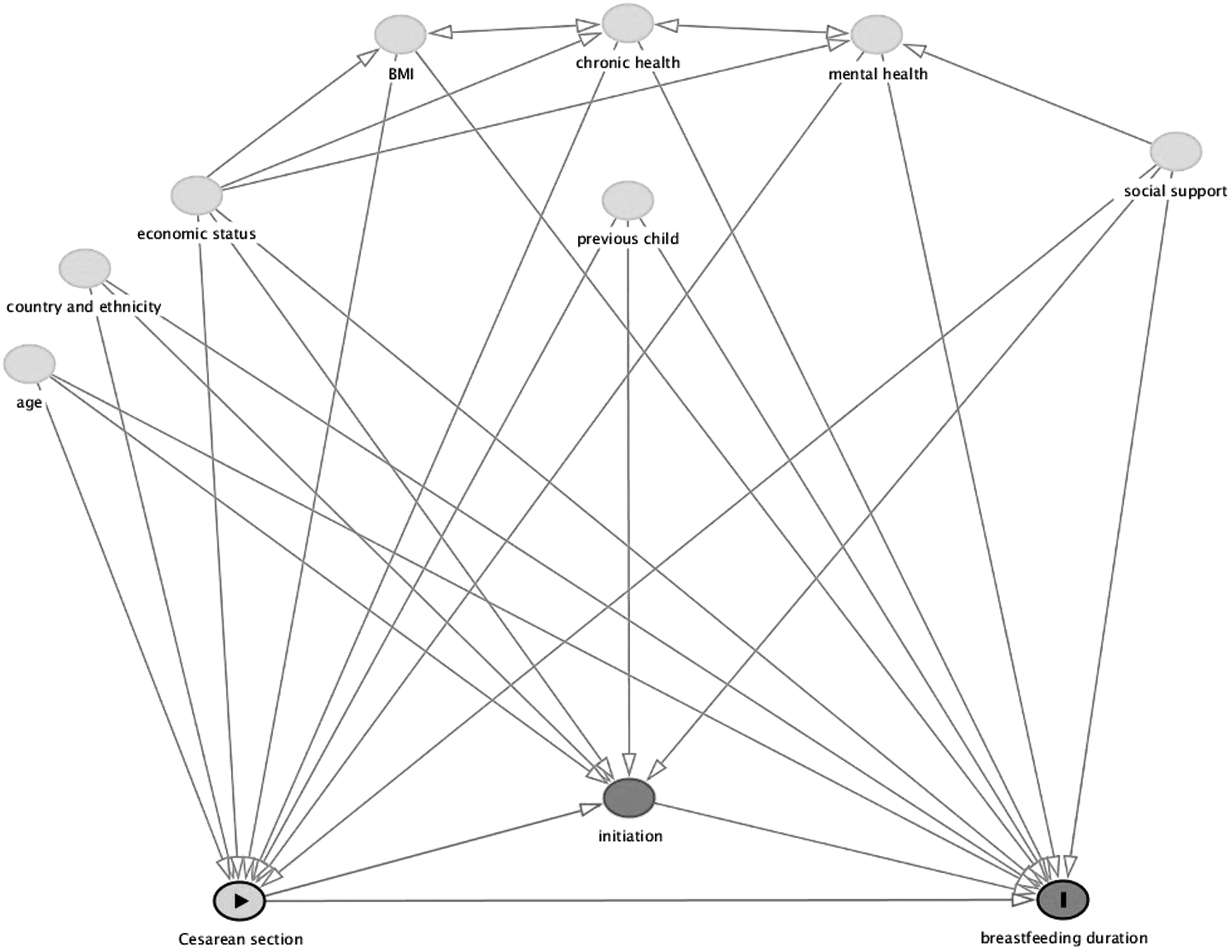
Directed Acyclic Graph depicting the pathways between cesarean section birth (exposure) and breastfeeding duration (outcome).
These were as follows: Age of the mother at birth (12–19, 20–29, 30–39, and 40+), other natural siblings of the cohort (yes/no) as a proxy for parity or birth order, ethnicity (white, mixed, Indian, Pakistani and Bangladeshi, Black or Black British, and other) and country (England, Wales, Scotland, and Northern Ireland), national vocational qualification (NVQ) equivalent of highest academic attainment (NVQ 1–3, NVQ 4–5, none, or overseas qualifications only), per annum family income (0–10,400, 10,400–20,800, 20,800–31,200, 31,200+, and other), paid work status (currently doing paid work, has paid job but on leave, has worked in the past but no current paid job, or never had a paid job), frequency of seeing parents (at least weekly or not as frequently/ever), frequency of seeing friends (at least weekly or not as frequently/ever), mothers' BMI before birth (healthy, underweight, overweight, or obese), longstanding health issue or disability (yes or no), and ever diagnosed with depression or anxiety.
Analysis
We first fit logistic regression models to examine the relationship between mode of birth and initial breastfeeding attempt. For the survival analysis, we visualized the relationships between mode of birth and duration of any and exclusive breastfeeding with Kaplan-Meier curves stratified by first birth and subsequent (second order or higher) birth to control for birth order, a key confounder in the relationship between mode of birth and breastfeeding initiation and duration. 31 We then tested for proportional hazards of exposures relative to the outcome, an important assumption of the commonly used Cox regression models, and determined that the hazards violated assumptions of proportionality.
We applied Accelerated Failure Time models with a Weibull distribution, censoring at 6 months. This distribution was selected after testing several distributions (Weibull, log-normal, log-logistic, and exponential) for goodness of fit using Akaike's Information Criterion (AIC). The Weibull distribution had the lowest AIC, thus producing the best fit models. For all three outcomes (initiation, duration of any, and exclusive breastfeeding), we examined mode of birth first by vaginal birth versus any C-section, and next by disaggregating C-section according to whether it was planned or unplanned, in both unadjusted models and models that adjusted for mothers' characteristics.
We used Stata version 16.0 for the analysis. All analyses adjusted for the complex survey design and applied survey weights to adjust for nonresponse and disproportionate sampling.
Ethical approval
This study was considered exempt by the Institutional Review Board at the University of Maryland.
Results
Compared with all respondents in the first sweep of MCS to our analytic sample, there was no meaningful difference in characteristics with exception to C-section, which had a significantly lower prevalence in our analytic sample (18.5%; 95% confidence interval [95% CI]: 17.6–19.3 versus 21.0; 95% CI: 20.2–21.8) (Supplementary Table S1). This is likely owed to our exclusion of preterm births and births with complications. Tables 2 and 3 show the characteristics of all women and women who breastfed, by mode of delivery. Among those in our sample, 71% attempted to initiate breastfeeding; 82% delivered vaginally; and 9% and 10% had a planned or unplanned C-section, respectively (Table 2). Half (49%) of the children of respondents had no natural sibling living in the household, although there were significant differences by the type of C-section.
Mothers' Characteristics Among All Those with a Singleton, Term Birth, Stratified by Mode of Birth—UK Millennium Cohort Study (2000–2002)
All estimates are weighted and account for the complex sample design.
BMI, body mass index; C-section, cesarean section; CI, confidence interval; NVQ, National Vocational Qualifications.
Mothers' Characteristics Among Those Who Ever Attempted to Breastfeed, Stratified by Mode of Birth
All estimates are weighted and account for the complex sample design.
BMI, body mass index; C-section, cesarean section; CI, confidence interval; NVQ, National Vocational Qualifications.
Among those delivered by a planned C-section, 66% (95% CI: 62.8–68.8) had a sibling compared with 24% (95% CI: 22.0–26.5) among unplanned C-sections, likely capturing differences in repeat versus primary C-section. Among those who initiated breastfeeding (Table 3), there were notable differences by mode of birth. Those with planned C-section had a significantly higher likelihood of being of older age (30–39: 66.8%; 95% CI: 62.9–70.6) relative to both vaginal (49.1%; 95% CI: 47.0–51.2) and unplanned C-section births (55.2%; 95% CI: 50.9–59.5). Those with an emergency C-section were significantly more likely to work for pay (59.2%; 95% CI: 55.2–63.0) relative to those with either planned C-section (51.9%: 95% CI: 47.6–56.3) or vaginal birth (52.2%; 95% CI: 50.5–54.0).
The adjusted odds of ever attempting to breastfeed are 10% lower among those with any type of C-section compared with vaginal birth (odds ratio [OR]: 0.90; 95% CI: 0.81–1.01) (Table 4). By the type of C-section, only planned C-section predicts significantly lower odds of breastfeeding attempt (OR: 0.84, 95% CI: 0.71–0.99) compared with vaginal birth. The odds of breastfeeding attempt for those with an unplanned C-section were not significantly different from those with vaginal birth. The results of the models, including all covariates, are presented in Supplementary Table S2.
Results of Logistic and Accelerated Failure Time Analyses Assessing Ever Breastfeeding, and, Among Those Who Attempted to Breastfeed, Duration of Any and Exclusive Breastfeeding for Any Cesarean Section, and Type of Cesarean Section Compared with Vaginal Birth—UK Millennium Cohort Study (2000–2002)
Adjusted models control for mother's age at birth, other children in the household, mother's ethnic group, country, academic NVQ equivalent, family income, employment status, frequency of seeing parents, frequency of seeing friends, mother's BMI, and lifetime diagnosis of depression or anxiety. All analyses are conducted among mothers with singleton, term babies without special care, 6 months of age or older with nonmissing information. The accelerated failure time models (duration of any breastfeeding or exclusive breastfeeding) are further restricted to mothers who attempted to initiate breastfeeding.
AOR, adjusted odds ratio; ATR, adjusted time ratio; BMI, body mass index; C-section, cesarean section; CI, confidence interval; NVQ, national vocational qualification; UOR, unadjusted odds ratio; UTR, unadjusted time ratio.
Using Kaplan-Meier curves, Figure 3 depicts the associations between mode of birth and duration of breastfeeding among those who initiated breastfeeding. The graphs are stratified by first birth or subsequent birth (the maternal characteristic that differed the most by mode of birth), and by any or exclusive breastfeeding. Overall, we see earlier cessation of breastfeeding in both planned and unplanned C-sections relative to vaginal births, but differences largely resolve by 6 months.

Kaplan-Meier estimates of the time to cessation of any or exclusive breastfeeding in days by first or subsequent birth, for up to 6 months
Among first births, the differences in duration of any breastfeeding are least apparent and, by 5 months, differences converge at 66% across each type of birth; there are more pronounced differences among first births for exclusive breastfeeding, but similar probability of cessation at 6 months (93–95%). Among subsequent births for any breastfeeding, planned C-section has a more rapid and disparate time to discontinuation of breastfeeding than both unplanned C-section and vaginal birth, which are more similar to each other. For exclusive breastfeeding, the rate discontinuation of breastfeeding is more rapid for unplanned C-section and is more like planned C-section than vaginal birth, although exclusive breastfeeding among all groups again converges at the end of the 6-month period.
After adjusting for other covariates, those with any C-section had a 20% shorter median time to weaning from any breastfeeding compared with vaginal birth (time ratio [TR]: 0.80, 95% CI: 0.72–0.90) (Table 4). For those with a planned C-section, the median time was 25% shorter (TR: 0.75, 95% CI: 0.64–0.89), but less short for unplanned C-section (TR: 0.85, 95% CI: 0.74, 0.97), although both types of C-section were significantly different from vaginal birth. For exclusive breastfeeding, the duration of time was 18% (TR: 0.82) shorter when comparing any C-section (95% CI: 0.75–0.89), planned C-section (95% CI: 0.72–0.93), and unplanned C-section (95% CI: 0.74–0.90) to vaginal deliveries. Supplementary Tables S3 and S4 provide the full results of unadjusted and adjusted models.
Finally, we conducted a sensitivity analysis to examine whether using different age cut points that reflect advanced maternal age (35+), given the increased probability of C-section, and found no substantive or meaningful change to any adjusted model.
Discussion
This large, population-based, prospective study is the first to fit hazard models that accommodate the changing effect of the exposure over time to examine duration of breastfeeding by type of C-section. Among our sample, duration of both any and exclusive breastfeeding was shorter among both planned and unplanned C-section births relative to vaginal births. Although this finding aligns with one study 32 applying proportional hazards, it conflicts with two others that found only those with emergency C-section (but not planned) 29 or planned C-section (but not emergency) 11 had a shorter time to cessation of breastfeeding compared with vaginal birth. 29
Our findings also contradict a meta-analysis 13 that found, after restricting to 11 of 15 studies that examined breastfeeding at 6 months only among those who initiated breastfeeding, there was no difference by mode of birth. Their null finding may be due to inclusion of studies situated across different health systems or with methodological issues such as lacking appropriate controls. Moreover, as seen in our study and others, breastfeeding differences by mode of birth diminish over time34,35; consequently, the reported null findings may also reflect studies that focus on this 6-month time point. In our study, this null effect holds true for exclusive breastfeeding, given that most mothers have stopped exclusively breastfeeding by this time, regardless of mode of birth.
Like previous research,11–13 our study observed that those who had a planned C-section were less likely to attempt breastfeeding and there was no difference in unplanned C-section relative to vaginal birth. When examining duration of any breastfeeding during the first 6 months of infancy, there are marked differences in complete cessation of any breastfeeding by vaginal versus C-section birth, but the effects are most pronounced for planned C-section. In terms of exclusive breastfeeding, both unplanned and planned C-section had similarly shorter durations relative to vaginal birth.
This confirms that those undergoing either type of C-section may encounter more difficulties maintaining breastfeeding without the introduction of supplemental feeding. As noted in other studies,17,25 only initiation of any breastfeeding differed by type of C-section, implicating differing maternal preferences in breastfeeding between mothers who had planned C-section and those who intended for a vaginal birth. Because we accounted for personal motivation to breastfeed by applying a time-to-event analysis, our findings further support the hypothesis that physiological mechanisms important for long-term breastfeeding may be disrupted by C-section.
This study has several strengths. Because of the large population-based sample with data collected through a complex sample design and with low missingness, our sample is representative of the population of United Kingdom. Our study expanded upon research on breastfeeding duration by using a continuous measure of breastfeeding to examine both exclusive and any breastfeeding up to 6 months. Previous studies have cited barriers in the use of survival analysis, including the violation of proportional hazards 35 ; we overcame this shortcoming by fitting accelerated failure time models. Furthermore, we differentiated between planned and unplanned surgical birth and expanded on previous research, 13 providing further insight about these complicated relationships.
We consider these findings bearing in mind the study's limitations. First, we were unable to control for all potential confounders, for example, perinatal complications, hospital policies and practices related to both C-section and promotion of breastfeeding, intent for duration of breastfeeding, or other maternal characteristics. 25 However, we excluded preterm births and those who received special or intensive care to limit the confounding effect of complications. While we were able to differentiate between planned and emergency C-section, we were unable to further distinguish the timing of the C-section relative to experience of labor, which may result in residual confounding.
There are important limitations that may arise from changes over time in medical practices. At the time of data collection for this study (2000–2002) in United Kingdom, skin-to-skin contact between mother and baby immediately after birth, known to promote breastfeeding initiation, 36 was not routinely practiced after C-section, 37 and has only recently been included in breastfeeding promotion guidelines. 28 Although breastfeeding support practices and related behaviors have expanded in United Kingdom since this study, and breastfeeding rates have increased in tandem, 38 these practices would not confound the relationship we examine based on the assertion that these practices do not predict the mode of birth.
Similarly, induction of labor likely affects breastfeeding, 29 although a recent large, randomized controlled trial found that induction in term pregnancies did not increase the risk of C-section 39 and induction is unlikely to confound our analysis. Changes to C-section procedures may also affect the relationship between mode of birth and breastfeeding over time. Recent advancements may result in shorter operation time, less postoperative pain, and quicker recovery time, 40 which could attenuate this relationship. Notwithstanding these considerations, it is essential to acknowledge the dynamic nature of medical practices, and to recognize that there may be limitations in our study that we have not identified.
In addition, it is possible that early supplementation may have been given to the baby, for example, in the hospital nursery before the mother started or resumed exclusive breastfeeding; in this case, our analysis considered these cases to no longer be exclusively breastfeeding, which may overestimate the magnitude of the relationship between C-section and duration of exclusive breastfeeding. As early supplementation is also associated with earlier weaning, 41 the potential overestimation is likely small.
As the survey did not ask about provision of donor milk, we were unable to account for it in supplementing the mothers' milk at any time. Also, our sample is of limited generalizability to settings outside United Kingdom or similar cultures or to more current settings as breastfeeding practices have changed. Future studies could explore how these relationships may differ across culture, or time, and the contribution of secular changes in breastfeeding support or skin-to-skin to this relationship.
Conclusion
Breastfeeding benefits both the mother and baby, including infant protection against infection, 1 although in the face of a multitude of barriers, not all mother-baby dyads achieve such benefits when breastfeeding is not initiated or is short in duration. Through application of rigorous methods, this study provides compelling evidence that breastfeeding duration may be impeded by C-section birth. Although additional studies using more recent data are needed, the findings have implications for interventions to improve breastfeeding initiation and duration: Additional support for mothers undergoing C-section may be warranted. Programmatic and policy-related efforts can focus on proven modifiable, health systems factors for promoting early and prolonged breastfeeding, including skin-to-skin, provider training and counseling, and supportive hospital policies for those with a C-section birth. These evidence-based interventions should also be enacted within a rights-based framework for respect for individual autonomy in the decision to breastfeed.
Footnotes
Acknowledgments
We gratefully acknowledge support from the Eunice Kennedy Shriver National Center for Child Health and Human Development grant P2C-HD041041, Maryland Population Research Center. The authors would like to thank Caroline Tumulty-Ollemar for her contribution to the structured literature review. The results of this research have been presented as posters in two conferences: Society for Perinatal Epidemiological Research, 2023, Portland, OR, 2023: https://sper.org/wp-content/uploads/2023/06/2023-Abstract-Book-1.pdf and the Population Association of America Annual Meeting, 2022, Atlanta, GA ![]() Although the results were presented at these conferences, the full article is not published, in press, or submitted elsewhere.
Although the results were presented at these conferences, the full article is not published, in press, or submitted elsewhere.
Authors' Contributions
L.M.M.: Conceptualization, methodology, software, formal analysis, data curation, writing—original draft, writing—review and editing, visualization, and project administration. E.D.S.: Conceptualization, methodology, writing—review and editing, and supervision.
Disclosure Statement
We have no conflict of interests to declare.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.