
Abstract
Background:
The objective of this study was to investigate the relationship between the Edinburgh Postpartum Depression Scale (EPDS) score on the 10th day postpartum and the number of breastfeeding sessions per day among puerperal women (with no known depression risk factors and a low [<10] EPDS score after delivery).
Materials and Methods:
A total of 1,451 nulliparous, 37- to 41-week pregnant women who gave birth between August 2020 and August 2022 and who underwent routine postpartum checkups on the 10th day after delivery were included in this study. Pregnant women with risk factors for depression before pregnancy, during pregnancy, and after delivery were not included. Patients with an EPDS score of ≥10 after delivery were excluded from the study. On the 10th day after birth, the mean number of breastfeeding sessions per day of the population in the study was determined. Patients with a number of breastfeeding sessions per day above the mean value were classified as Group A (n = 45), and those with values below the mean were classified as Group B (n = 67).
Results:
The mean number of breastfeeding sessions per day was 10.15. The EPDS scores of Group A (6 [0–19]) were significantly lower than those of Group B (8 [0–20]) (p < 0.05). A negative linear relationship was found between the number of breastfeeding sessions per day and the EPDS scores on the 10th day postpartum (p < 0.05). No statistically significant difference was found between the EPDS scores and the education status, age, or gestational week of the patients (p > 0.05). There was no statistically significant difference between the number of breastfeeding sessions per day and the education status or age of the patients (p > 0.05).
Conclusions:
Higher number of breastfeeding sessions per day is associated with less risk of maternal postpartum depression. There is a need for new studies on the consequences of the number and quality of breastfeeding sessions.
Introduction
Postpartum depression (PPD) is a serious cause of maternal morbidity and has potential negative consequences for infants. A major depressive episode occurring in the first 4 weeks after birth is defined as PPD.1,2 It has been reported that biological, psychological, and sociocultural factors are involved in the etiology of PPD.3,4 The Edinburgh Postpartum Depression Scale (EPDS), consisting of 10 items, each scored from 0 to 3, was developed to understand whether PPD will develop in patients with risk factors for depression. A score of 10 and above on this 30-point scale indicates a mild-high risk for the development of PPD.5,6
Studies have shown that in patients with high PPD scores, the number of breastfeeding sessions (number of breastfeeding sessions per day) is lower. In addition, these patients stop breastfeeding early in the postpartum period (4–8 weeks).7–11 Studies on PPD were conducted in patients with known prenatal depression risk factors or in patients with high postpartum depression risk scores. While it has been shown in many studies that the number of breastfeeding sessions per day decreases due to depression, there is no study in the literature on whether a decrease in the number of breastfeeding sessions per day independent of depression paves the way for the development of depression.
In the current study, we predicted that patients with no known depression risk factors and a higher number of breastfeeding sessions per day would have lower EPDS scores on the 10th day postpartum.
Therefore, the aims of this study were to investigate the relationship between the EPDS score on the 10th day postpartum and the number of breastfeeding sessions per day among puerperal women (with no known depression risk factors and a low [<10] EPDS score after delivery) and to ascertain whether an increase in the number of breastfeeding sessions per day has a protective effect against possible PPD.
Materials and Methods
The study was planned and completed as a retrospective cohort study. This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the ethics committee of the Basaksehir Cam and Sakura City Hospital Local Ethical Committee (date: October 12, 2022, No. 2022.10.323/protocol No. 323).
Design of the study
Pregnant women who gave birth in the Basaksehir Cam and Sakura City Hospital between August 2020 and August 2022 and who underwent routine postpartum checkups on the 10th day after delivery were screened retrospectively using hospital records. Risk factors that may cause depression before pregnancy, during pregnancy, and after delivery were assessed by administering a questionnaire to a total of 1,451 nulliparous, 37- to 41-week pregnant patients, and those with risk factors were not included in the study. EPDS scores were examined using the EPDS, which was completed in the labor room after delivery by the patients who did not have risk factors for depression. Patients with an EPDS score of ≥10 were excluded from the study.
The study continued with a total of 249 evaluable patients who met the standardization criteria (without depression risk factors and with an EPDS score of <10). On the 10th day after birth, the patients were routinely evaluated by an obstetrician and gynecologist and psychologist in our puerperium clinic. The data collected for each patient from the puerperium clinic were the average number of breastfeeding sessions per day (24 hours) recorded by the obstetrician and gynecologist and the EPDS score on the 10th day postpartum recorded by the psychologist. When determining the number of breastfeeding sessions per day, only mothers who breastfed with skin contact were included. Mothers who used bottle feeding or formula feeding in addition to breastfeeding were not included in the study. The number of times the mother breastfed per day within a 24-hour period was determined. The average number of breastfeeding sessions per day during the 10-day postpartum period was determined. Patients who did not come to the puerperium control and who had missing information about the number of breastfeeding sessions per day or EPDS score were excluded from the study.
The mean number of breastfeeding sessions per day of the population in the study was determined. The patients with a number of breastfeeding sessions per day above the mean value were classified as Group A, and those with a number below the mean value were classified as Group B. The study was completed with a total of 112 patients. We investigated whether there was a statistically significant difference between the two groups in the EPDS score on the 10th day postpartum. The relationship between the EPDS score on the 10th day postpartum and the education status, age, and gestational week of the patients was investigated. In addition, the relationship between the number of breastfeeding sessions per day and the education status or age of the patients was investigated.
Inclusion and exclusion criteria
To minimize the effects of different factors on EPDS scores, term pregnant women between the ages of 20 and 38 years who were pregnant for the first time and were at or beyond 37 weeks were included in the study. Postterm pregnant women (41 weeks and later) were not included in the study. Only pregnant women who had a normal unassisted vaginal delivery were included. Patients who had undergone cesarean section and who underwent labor induction with oxytocin or prostaglandin E2 during labor were not included. Mothers with feeding methods other than breastfeeding (e.g., bottle or formula feeding) were excluded from the study.
Only mothers who breastfed their babies with skin contact were included in the study. In the questionnaire survey, patients with secondary school and above education levels were included in the study. Patients with the following were ineligible and excluded from the study: a history of depression, any chronic disease (high blood pressure, diabetes, migraine, etc.), antidepressant use, drug addiction, smoking, a history of alcohol use, a family member with a chronic illness that could affect domestic peace, a first-degree relative who died in the past 5 years, a self-reported special stress situation, a divorce or a deceased spouse, and a household income below the national poverty line. Patients with an EPDS score of 10 or above following delivery or with a complicated delivery were excluded from the study.
Patients with stress factors related to the neonate (such as admission to the neonatal intensive care unit, jaundice, or anything requiring any extra follow-up) were also not included. Patients who were discharged at 24 hours postpartum were included, and those having prolonged hospitalization for any reason were excluded from the study.
Statistical analysis
For statistical analysis, SPSS Version 22.0 was used. To evaluate the distribution of the data, the Shapiro–Wilk test was used. Variables that did not conform to the normal distribution are reported as median, minimum, and maximum values. The Mann–Whitney U test was used to analyze the differences between the two groups, and the Kruskal–Wallis H test was used to analyze the differences among three or more groups. The relationships between the variables were examined with the Spearman correlation coefficient. A p-value of 0.05 was taken as the threshold level for statistical significance.
Results
Within the scope of the study, the records of 1,451 nulliparous women were examined. After applying the inclusion/exclusion criteria, the study continued with 249 eligible patients. Patients who did not come to the 10th day puerperium control and who had missing information about the number of breastfeeding sessions per day or EPDS score were excluded from the study. The study was completed with a total of 112 patients.
Comparison of EPDS scores and the number of breastfeeding sessions per day between the groups
The mean number of breastfeeding sessions per day in the entire study group was 10.15. It was determined that there were 45 puerperal women with a number of breastfeeding sessions per day above the mean value (Group A) and 67 puerperal women with a number of breastfeeding sessions per day below the mean value (Group B). A statistically significant difference was found in the EPDS score on the 10th day postpartum between Group A and Group B (p < 0.05). The EPDS scores of Group A were lower than those of Group B (Table 1). In addition, a negative linear relationship was found between the number of breastfeeding sessions per day and the EPDS score on the 10th day postpartum (p < 0.05) (Fig. 1). It was determined that the EPDS score decreased as the number of breastfeeding sessions per day increased.
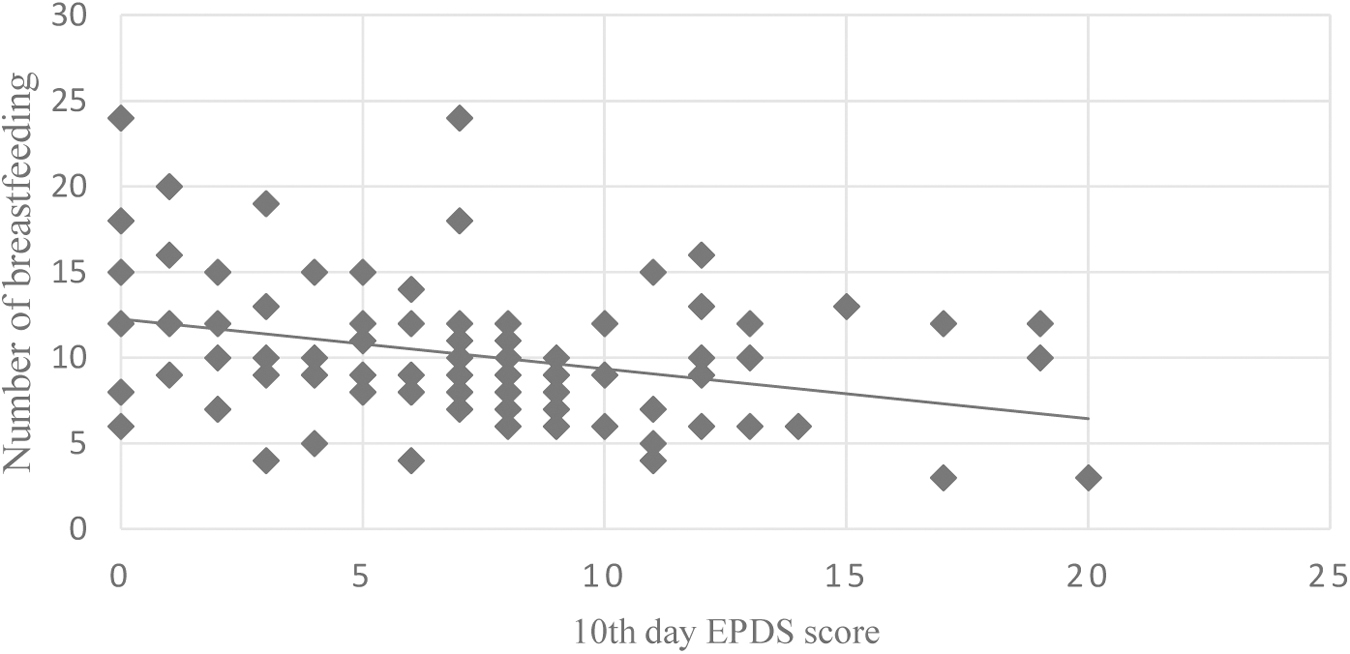
Negative linear relationship between the number of breastfeeds and the 10th day EPDS scores. EPDS, Edinburgh Postpartum Depression Scale.
Comparison of the 10th Day Edinburgh Postpartum Depression Scale Scores Between the Groups
p < 0.05, Mann–Whitney U test.
EPDS, Edinburgh Postpartum Depression Scale.
Evaluation of descriptive statistics
No statistically significant difference was found between the groups regarding the EPDS scores on the 10th day postpartum and the education status, age, or gestational week of the patients (p > 0.05). There was no statistically significant difference between the number of breastfeeding sessions per day and the education status or age of the patients (p > 0.05).
Discussion
In this study, it was shown that the number of breastfeeding sessions per day in the early postpartum period affects PPD risk scoring. Higher number of breastfeeding sessions per day is associated with lower EPDS score. It was determined that the number of breastfeeding sessions per day was not affected by education level or age. Moreover, maternal age, education status, and gestational week did not play a determining role in terms of the risk of early PPD in pregnant women between 37 and 41 weeks of gestation.
Many studies have indicated that breastfeeding influences maternal mood and psychological state. To demonstrate the importance of breastfeeding, a study comparing breastfeeding with bottle feeding examined maternal mood before and after breastfeeding. It was observed that there was a decrease in negative emotions after breastfeeding, and breastfeeding stabilized maternal mood in a positive way. Among the patients who bottle fed, there was no decrease in negative emotions, and a decrease in positive emotions was even observed. 12
There are many studies investigating the relationship between PPD and breastfeeding in the literature. Studies have shown that the presence of depression significantly affects the number and duration of breastfeeding sessions, which has positive effects on maternal mental health. Patients with antenatal depression were less likely to continue breastfeeding at 6 weeks postpartum than healthy puerperal women. In addition, the rates of initiation of breastfeeding were found to be lower among patients with depression. Similarly, mothers with a history of antenatal depression were found to have a lower number of breastfeeding sessions.13–16 In another study on breastfeeding and depression, the first-, second-, and third-trimester EPDS scores and the pattern and continuity of breastfeeding were examined. It was found that puerperal women with higher third-trimester depression scores had less continuity of breastfeeding. 17 These studies revealed the negative effects of prenatal depression on the number and duration of breastfeeding sessions.
Depressed mothers reported that their milk production was periodically too much or little, and they had more difficulty breastfeeding. They also needed more support.18,19 In a study examining the depression tendencies of mothers who have difficulty breastfeeding for various reasons, such as postpartum pain, it was determined that puerperal women who had difficulty breastfeeding have a higher tendency toward depression in the second month after delivery. In this study, which offers valuable evidence that regular and successful breastfeeding can be protective against depression, it was not investigated whether the included patients had a history of depression during the prenatal period or a tendency toward depression. 20 A prenatal depression background may have affected the results of the study. In the presence of a depression background, higher pain levels may have been experienced during breastfeeding due to the relative decrease in the pain threshold. Patients may have experienced increased breastfeeding difficulties due to depressive mood. 21 The main factor affecting the number and continuity of breastfeeding sessions may be a depressive state. 16 Likewise, an existing depressive illness may have been detected as a high EPDS score at the end of the second month postpartum.
In this context, how difficulty and failure in breastfeeding can affect depression scores may not have been fully revealed. Rather than factors causing discontinuity or a decrease in the number of breastfeeding sessions, such as pain during breastfeeding or incompatibility, the reason for the increase in EPDS scores may be a negative consequence of an undiagnosed depressive illness causing a reduction in the number or discontinuity of breastfeeding sessions.
In our study, mothers who used feeding methods other than breastfeeding with skin contact were excluded so that the study results would not be affected. In this way, the standardization of the study group was strengthened. Depression risk factor assessment was performed before and after birth to eliminate all the abovementioned effects and possibilities. The EPDS scores of women after birth were examined. Since the pregnant women who had met any of the exclusion criteria were excluded from the study, the study could continue with 112 of the 1,451 participants. Thus, by creating a standardized patient group, the effect of breastfeeding on EPDS scores was investigated exclusively. With this feature, our study is the first in the literature to examine the effects of breastfeeding on maternal mood independent of depression. In addition, this is the first study to show a negative linear relationship between the number of breastfeeding sessions per day and EPDS scores in a standardized group model.
In the study by Figueiredo et al., which investigated the relationship between breastfeeding and depression, it was determined that the depression scores of breastfeeding women in the third month postpartum were lower than those in the first trimester. No difference was observed in the scores of non-breastfeeding puerperal women in the third month postpartum and the first trimester. It has been stated that breastfeeding has a decreasing effect on depression scores. 17 In a study investigating the effects of breastfeeding on cortisol and adrenocorticotropic hormone (ACTH) blood levels, it was determined that breastfeeding reduced blood ACTH and cortisol levels. 22 These studies suggest that breastfeeding has a positive effect on postpartum maternal mood. Similarly, our study is supporting the conclusions in the literature.
Limitations of the study
Regarding the first limitation of this study, although the positive effects of breastfeeding on early postpartum EPDS scores were shown, long-term evaluations should be made at the sixth month, first year, and second year to determine the certainty of the protective effects of breastfeeding against depression. Evaluating the distribution of the number of breastfeeding sessions during the day on an hourly basis and especially analyzing how the frequency of breastfeeding at night affects EPDS scores would have increased the sensitivity of the study. In this study, the breastfeeding experiences of mothers in the postpartum period were not evaluated. It is impossible to determine from data of this study if the reduced number of breastfeeding sessions reflected breastfeeding difficulties. Thus, one cannot conclude if the frequency of breastfeeding sessions per se is the factor or that lower frequency of breastfeeding reflects difficulties in breastfeeding that is the cause of the reduction. Breastfeeding difficulties should be analyzed in new studies about the number of breastfeeding sessions.
Conclusions
Higher number of breastfeeding sessions per day is associated with less risk of maternal PPD. There is a need for new studies on the consequences of the number and quality of breastfeeding sessions.
Footnotes
Authors' Contributions
Study concept and design were performed by İ.İ.A. and M.C.S. Data collection was performed by İ.İ.A., M.C.S., and K.O.C. Data analysis was performed by K.O.C., İ.İ.A., and M.C.S. The first draft of the article was written by M.C.S. All authors commented on previous versions of the article. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.