
Abstract
Background:
Benefits of early skin-to-skin contact (SSC) between mother and newborn are widely documented, including improved breastfeeding outcomes. While promoting immediate SSC is standard practice for vaginal birth, it happens less often after cesarean birth. It is not known how changes in hospital practices and staffing shortages during the COVID-19 pandemic have influenced the practice of SSC in the operating room (OR). This study aims to identify the relationship between SSC after cesarean birth and breastfeeding and compare SSC before and during the COVID-19 pandemic at a single institution.
Materials and Methods:
This was a retrospective cohort study of 244 subjects who had scheduled cesarean births during 2019 and 2020. The primary outcome was newborn feeding at hospital discharge. Secondary outcomes were time to initiate breastfeeding, newborn feeding at 4–8-weeks postpartum, and location of SSC initiation in 2019 versus 2020.
Results:
SSC within 3 days of birth was significantly associated with feeding type on discharge and/or 4—8 weeks postpartum. More subjects intending to exclusively breastfeed met this intention at discharge with SSC in the OR. Newborns who had SSC in the OR had significantly earlier initiation of breastfeeding. There was an increase in SSC in the OR between 2019 (27%) and 2020 (39%).
Conclusion:
SSC in the OR was associated with improved short-term breastfeeding outcomes in our study. If immediate SSC is not possible, SSC within 3 days of birth may have breastfeeding benefits. The increase in SSC in the OR during the COVID-19 pandemic indicates that SSC practices can be implemented, despite challenging circumstances.
Introduction
The health benefits of breastfeeding are widely documented. 1 Skin-to-skin contact (SSC) between newborn and mother within the first hour of birth improves breastfeeding outcomes. 2 While promoting immediate SSC has become standard practice for vaginal births, it happens less often after cesarean births. 3 Importantly, it is not known how changes in hospital practices and nursing staff shortages during the COVID-19 pandemic influenced the practice of SSC in the operating room (OR) after cesarean birth.
SSC is defined as placing the naked or diapered newborn baby in the prone position on the mother's bare chest or abdomen shortly after birth so that the baby has ready access to the maternal nipple. Mother and baby are covered with a prewarmed blanket, leaving the baby's head exposed. 4 The American Academy of Pediatrics (AAP) recommends that, regardless of feeding choice, routine procedures should be conducted while SSC is underway, and procedures that may be painful or require separation from the mother should be delayed until after the first hour and until after the first breastfeeding is completed, if breastfeeding is desired. 1 In the case of cesarean births, AAP recommends that SSC be initiated when the mother is awake and able to respond to her newborn. 1
Promoting early initiation and longer duration of breastfeeding is recognized as a global health priority. In their Baby-Friendly Initiative, the World Health Organization (WHO) recommends that birthing facilities adopt policies and procedures to support breastfeeding; these are summarized in a list of “Ten Steps to Successful Breastfeeding.”5 Initiation of immediate and uninterrupted SSC between mother and newborn as soon as possible after birth is one of the ten steps, as is exclusive breastfeeding unless medically contraindicated. 5 Benefits of SSC between mother and newborn are widely documented, including improved breastfeeding outcomes, newborn cardiorespiratory stability, thermoregulation, glucose regulation, newborn self-regulation, and reducing neonatal stress of birth, while facilitating transition to extrauterine life.6–9
Regardless of mode of birth, SSC reduces the duration of the third stage of labor, decreasing the risk of obstetric hemorrhage, reduces maternal stress, and increases maternal–newborn bonding.8–13 During and after cesarean birth specifically, SSC reduces maternal pain and increases birth satisfaction.9,14 In addition, SSC in combination with the initiation of breastfeeding within the first 30 minutes after birth reduces the risk of immediate postpartum hemorrhage. 15 Breastfed infants have a reduced risk of gastrointestinal infection, otitis media, respiratory tract infection, asthma, allergies, obesity, type 1 and 2 diabetes mellitus, and sudden infant death syndrome.16–19 In the long-term, mothers who breastfeed have a reduced risk of ovarian cancer, breast cancer, hypertension, coronary artery disease, and type 2 diabetes.20–25
Despite 31.8% of the U.S. births in 2020 occurring by cesarean, few studies have focused on evaluating SSC after cesarean birth, and the relationship of this intervention to breastfeeding outcomes. 26 Compared to SSC after vaginal birth, SSC in the OR is associated with challenges that include potential contamination of the surgical field, limited space at the head of the OR table, lack of communication regarding a mother's wishes for SSC, transferring mother and baby at the end of surgery, ability to perform newborn assessments, and ambiguity regarding roles of the health care team regarding SSC practices. 27 Despite the added challenges of SSC in the OR, if the mother and baby are stable after birth, it is possible to put evidence-based practices in place to facilitate safe SSC practices following cesarean birth.3,27,28
In 2018, SSC was introduced in the OR at our institution, as a component intervention in the Enhanced Recovery After Cesarean (ERAC) program. ERAC is a concept that aims to accelerate patient recovery by adopting a bundle of perioperative interventions, and is based on core elements of the Enhanced Recovery After Surgery protocols, which were initially successfully adopted in colorectal surgery, followed by the widespread adoption by other surgical specialties.29,30 Early initiation of breastfeeding is recognized as one important outcome of SSC within the context of the ERAC.29–31
The COVID-19 pandemic disrupted life globally. Nationally, changes to hospital practices, including visitor policies, use of personal protective equipment, delivery management, and newborn care, were made rapidly and based on limited data.32,33 Concerns about COVID-19, some based on scientific evidence and some not, may have influenced beliefs and attitudes surrounding SSC and breastfeeding by birthing families and their health care team. 34 Despite these concerns, evidence indicates that the benefits of breastfeeding outweigh the risk of transmission of SARS-CoV-2 virus, and practices that support breastfeeding, such as SSC, should not be discontinued. 35 Our institution maintained ERAC protocols during the pandemic; however, given that SSC in the OR depended on the availability of a nurse from the postpartum floor to assist with positioning and to monitor the newborn, there was concern that staffing shortages would affect the ability to undertake SSC in the OR during that period.
This study was designed to test the hypothesis that at a single institution, SSC practices after scheduled cesarean birth are associated with newborn feeding type at discharge and at the 4–8-week postpartum visit, and with earlier breastfeeding initiation. The study tested a secondary hypothesis that SSC practices decreased during the COVID-19 pandemic compared to before the pandemic.
Materials and Methods
Subjects
This study was a retrospective cohort study. The study was approved by the University of Iowa Institutional Review Board (No. 202103558). A waiver of informed consent was granted. Data were collected from electronic health records (EHR) of mother–newborn dyads who met the inclusion criteria of term (≥37 weeks' gestation) scheduled cesarean births. Subjects were excluded if record of SSC was not included in the EHR, if general anesthesia was used, or if there were contraindications to breastfeeding, including newborn with galactosemia, or maternal Human Immunodeficiency Virus (HIV) infection, Human T cell lymphotropic virus type I or type II infection, active untreated tuberculosis or varicella infection, active Herpes Simplex Virus lesions on the nipple, or breast surgery affecting duct function.
A convenience sample of all subjects who met the inclusion criteria and delivered between April and October 2019 (Group 1, before the COVID-19 pandemic) and between April and October 2020 (Group 2, during the COVID-19 pandemic) was collected. No subject in our study tested positive for COVID-19 during hospitalization.
Demographics
University of Iowa Hospitals and Clinics (UIHC) is an 800-bed academic medical center and regional referral center in the Midwest region of the United States. During the study time frame, there were ∼2,400 births per year, including almost 800 cesarean births. Of these, more than 200 were scheduled cesarean births. Figure 1 shows subject selection for our study. Two hundred thirty subjects were identified for analysis, with 117 subjects in Group 1 and 113 subjects in Group 2.

Flowchart diagram of subject selection. The study identified 230 subjects meeting criteria. Of the original 245 subjects identified, one was excluded due to contraindications to breastfeeding and 14 were excluded due to missing skin-to-skin data.
Context
Initially, the main concern with implementing SSC in the OR at UIHC was related to staffing, in terms of who would monitor the newborn during SSC. It was determined that the circulating nurse in the OR could not do this as they are needed to support the surgical team. As a result, SSC was initiated for scheduled cesarean births only, and arrangements were made for a nurse from the postpartum unit to monitor the newborn in the OR after the pediatric team completed their initial assessment and determined that the newborn could remain with the mother. During preliminary interviews with nursing staff in preparation for this study, staffing shortages and lack of predictability in terms of timing were identified as barriers to offering SSC in the OR after all scheduled cesarean births.
Data collection
Subjects meeting inclusion criteria were identified from the EHR. Study data were collected and managed using REDCap electronic data capture tools hosted at University of Iowa.36,37
Definitions and criteria
The primary outcome was defined as discharge feeding type. Secondary outcomes were defined as time to initiate breastfeeding, 4–8-week postpartum feeding type, and rate of SSC in 2019 compared to 2020. The mothers' self-reported newborn feeding type, exclusive breast milk feeding (EBMF), breast milk feeding supplemented with formula (BMFSF), or exclusive formula feeding (EFF), at discharge and at 4–8-weeks postpartum (when available) was identified from the EHR. For this study, EBMF was defined as feeding exclusively breast milk, including directly from the breast, expressed breast milk, and donor breast milk. Exposure was defined as any SSC within the first 3 days after birth, captured in the EHR by nursing staff as a dichotomous “yes/no,” with secondary analysis based on SSC location established, based on time of SSC and mothers' location, as recorded in nursing flow sheets.
At UIHC, regardless of desire for SSC, it is standard practice following cesarean birth for the newborn to be initially evaluated under a warmer by pediatric providers. If the newborn is stable, they return to their mother within a few minutes of birth. Subjects were grouped based on whether they had SSC at all, and further divided based on the location of SSC initiation: In the OR, postanesthesia care unit (PACU), or mother–baby care unit (MBCU).
In addition, times from birth to initiation of SSC and from birth to initiation of breastfeeding were collected, based on documentation in EHR nursing flow sheets. The infant's admission nursery was identified as the newborn nursery (NBN), transition nursery, or newborn intensive care unit (NICU). With NBN designation, an infant may remain with their mother and room-in, without physically being transferred to the NBN. Admission to the transition nursery or NICU implies that a neonate is transferred to a separate location for care.
Data collection
Data on demographic variables, including maternal age, self-identified race and ethnicity, preferred language, gravidity, parity and maternal body mass index (BMI), and obstetric/neonatal variables, including reason for scheduled cesarean birth, intrapartum complications, anesthesia type, perceived postpartum pain intensity, Edinburgh Postpartum Depression Score (EPDS), Apgar scores at 1 and 5 minutes, newborn birth weight, plan for newborn feeding, admit nursery, and reason SSC was not performed, when applicable, were collected from the EHR.
Postpartum pain intensity was assessed using two methods. First, the percentage of occasions over 24 hours that patients reported pain intensity as “acceptable” was calculated. Second, the morphine equivalent dose of analgesic use over 24 hours was calculated. EPDS scores were grouped as ≤8, 9–11, 12–13, and ≥14 based on validation studies showing that scores above 9 indicate possible depression with high sensitivity, but low specificity, and scores above 12 have lower sensitivity but higher specificity for diagnosing depression postnatally. 38 Apgar scores were grouped as 1–3, 4–6, and 7–10 based on the generally accepted rationale that newborns with Apgar scores between 1 and 3 tend to have higher clinical acuity compared to newborns with Apgar scores >7. 39
Statistical tests
The study utilized frequency distribution to describe the study population. Student's t-test and one-way analysis of variance tests were used to assess associations between normally distributed continuous variables by SSC exposure and between time points. Mann–Whitney U and Kruskal–Wallis tests were used for associations between continuous variables that failed Shapiro–Wilk testing for normality, by SSC exposure and between time points. Chi-squared analysis was used to test the association between categorical variables and SSC exposure and between time points. (SigmaPlot v13). A p < 0.05 represented an acceptable level of statistical significance.
Results
Demographics
Table 1 shows the demographic and obstetric/neonatal characteristics of our study population; these variables were similar in Group 1 and Group 2.
Demographic and Obstetric/Neonatal Characteristics by Study Period Pre-COVID-19 Pandemic (Group 1) and During COVID-19 Pandemic (Group 2), and Total Subject Population
Student's t-test for significant differences by study period (t statistic [degrees of freedom], two-tailed p-value).
Mann–Whitney U test for significant differences by study period (Mann–Whitney U statistic, p-value).
Chi-square test for significant differences by study period (Pearson's chi-square statistic [degrees of freedom], p-value).
BMI, body mass index; IQR, interquartile range; NBN, newborn nursery; NICU, neonatal intensive care unit; SD, standard deviation; SSC, skin-to-skin contact.
Any SSC during first 3 days after birth
Overall, 150 (65%) subjects were identified as having SSC within 3 days of birth. At discharge, 69% of newborns who had SSC within 3 days were EBMF compared to 45% who did not have SSC, and 48% were EBMF at the 4–8-week postpartum visit compared to 31% who did not have SSC (Fig. 2). Significant differences in discharge feeding type (p < 0.001) and/or postpartum feeding type (p = 0.04) were identified between subjects who had SSC compared to those who did not have SSC (Table 2). Newborns who had SSC within 3 days of birth were more likely to be EBMF on discharge (odds ratio = 2.7, 95% confidence interval [CI 1.6–4,8]) and at the postpartum visit (odds ratio = 2.0, 95% CI [1.1–3.7].
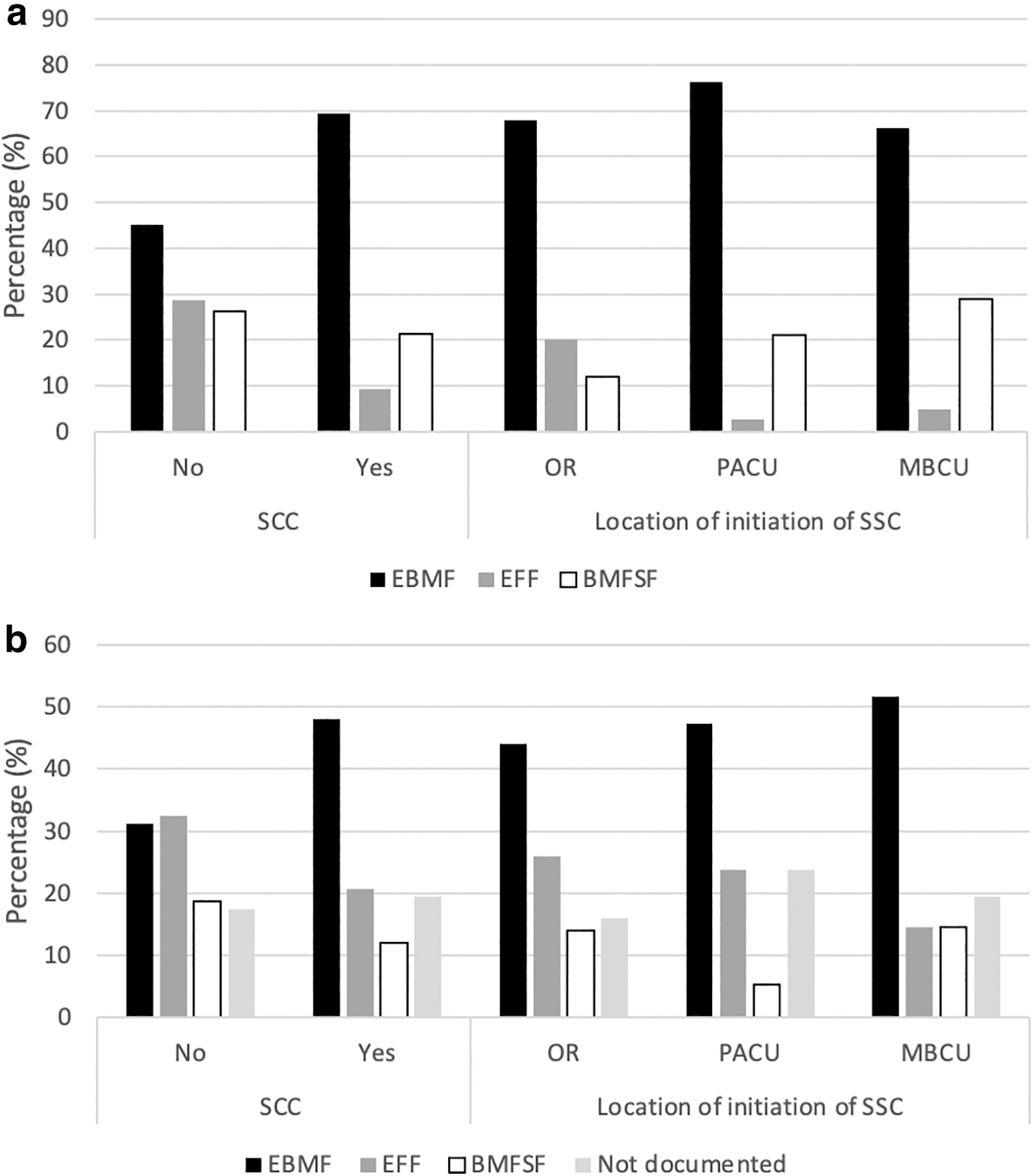
Chart showing percentage distribution of different feeding types grouped by SSC exposure.
Distribution of Outcomes and Covariates by Skin-to-Skin contact Exposure During the First 3 Days After Birth and by Location of First Skin-to-Skin contact in the Operating Room, Postoperative Care Unit, or Mother–Baby Care Unit
Chi-square test for significant differences by SSC exposure during first 3 days after birth (Pearson's chi-square statistic [degrees of freedom], p-value).
Chi-square test for significant differences by first SSC location (Pearson's chi-square statistic [degrees of freedom], p-value).
BMFSF, breast milk feeding supplementing with formula; EBMF, exclusive breast milk feeding; EFF, exclusive formula feeding; FTND, feeding type not documented; MBCU, mother–baby care unit; OR, operating room; PACU, postoperative care unit.
Location and timing of SSC
There were significant differences in discharge feeding type by location of SSC initiation, based on Chi-squared analysis (Table 2). EBMF occurred slightly, but not significantly, more often if SSC was initiated in the PACU (76%) versus OR (68%) or MBCU (66%) (Fig. 2). Chi-squared analysis of EBMF compared to BMFSF and EFF combined, by SSC location, revealed that these differences were not significant, X2 (2, N = 150) = 1.21, p = 0.55.
However, Kruskal–Wallis H test of time to initiate breastfeeding by SSC location revealed newborns who had SSC in the OR had significantly earlier initiation of breastfeeding, (m[IQR] = 88[111] minute) versus PACU (m[IQR] = 102[180] minutes) or MBCU (m[IQR] = 262[385] minutes), H(2) = 26.8, p ≤ 0.001 (Fig. 3). A significant association between SSC location and 4–8-week postpartum feeding type was not identified. Regardless of location of SSC initiation, median time to initiate SSC was earlier for subjects who were EBMF on discharge (m[IQR] = 94 [312] minutes] versus BMFSF (m[IQR] = 226 [408] minutes), H(2) = 7.66, p = 0.022. Time to initiate SSC was similar across feeding types at the 4–8-week postpartum visit (Supplementary Table S1).

Box and whisker plot showing median time to initiate breastfeeding for each SSC location. Newborns who had SSC initiated in the OR (m[IQR] = 88[111] minute) had earlier initiation of breastfeeding versus PACU (m[IQR] = 102[180] minutes) or MBCU (m[IQR] = 262[385] minutes), p ≤ 0.001.
Pre-COVID-19 pandemic versus during COVID pandemic
Group 1 undertook SSC in the OR significantly less often than Group 2 (27% versus 39%, p = 0.03; Fig. 4a). Time to SSC initiation following birth was significantly earlier in Group 2 (m[IQR] = 81[240] minutes] compared to Group 1 (m[IQR] = 171[371] minutes) (Mann–Whitney test, z = 2.22, p = 0.026; Fig. 4b). However, our study found no significant difference in EBMF on discharge (52.1% versus 47.9%) or 4–8 weeks postpartum (53.6% versus 46.4%) between 2019 and 2020 (Supplementary Table S1).

Chart showing percentage distribution of SSC during 2019 (Group 1) and 2020 (Group 2) time points. (a), Percentage distributions of SSC initiated in each location (OR, PACU, or MBCU) and all locations are represented for subjects who gave birth prepandemic (Group 1) and during the pandemic (Group 2). There was a significant difference between SSC initiation in each location for 2019 versus 2020 (p = 0.03). In Group 1, more subjects had SSC in the MBCU (OR 27%, PACU 21%, MBCU 52%), whereas in Group 2, more subjects had SSC in the OR (OR 39%, PACU 30%, MBCU 31%). Overall, in Group 1 (N = 117), 62% of subjects had SSC in any location during the first 3 days after birth with a slight increase to 68% in Group 2 (N = 113).
Covariates
When analyzing for confounding variables, no significant difference was identified between SSC exposure and maternal race, ethnicity, preferred language, age, BMI, gestational age at delivery, gravidity, parity, neonatal sex, birth weight, reason for scheduled birth, anesthesia type, EPDS, pregnancy or intrapartum complications, or postpartum pain intensity (Supplementary Table S2).
Significant differences in plan for feeding (p = 0.004), admitting nursery (p = 0.003), and Apgar scores at 1 and 5 minutes (p = 0.003 and p = 0.040, respectively) were identified between subjects exposed to SSC versus those who were not (Table 2). Newborns who had SSC within 3 days after birth had increased odds of admission to NBN (odds ratio = 5.2, 95% CI [2.8–9.9]), or Apgar scores 7–10 at 1 minute (odds ratio = 2.9, 95% CI [1.5–5.8]) and 5 minutes (odds ratio = 6.0, 95% CI [1.2–30.5]). Mothers who intended to EFF had significantly reduced odds of having SSC within 3 days after birth (odds ratio = 0.30, 95% CI [0.14–0.66]).
Among subjects who had SSC within 3 days after birth, significant differences were identified between location of SSC initiation and both admission nursery (p = 0.01) and plan for feeding (p = 0.03). Newborns who had SSC in the OR had increased odds of admission to NBN (odds ratio = 13.0, 95% CI [1.7–99.9]). When the analysis was restricted to only subjects planning to EBMF, subjects who had SSC in the OR more often were EBMF at discharge (91.7%) versus PACU (84.8%), MBCU (78.0%), or no SSC (63.2%). Chi-squared analysis revealed these differences were significant, X2(6, N = 176) = 16.64, p = 0.011. Among those planning to EBMF, the rates of EBMF at the 4–8-week postpartum visit were similar for SSC in the OR (55.6%), PACU (54.5%), MBCU (56.0%), or no SSC (42.1%), X2(9, N = 176) = 14.86, p = 0.095.
Supplementary Table S1 shows that discharge feeding type was associated with differences in admitting nursery (p = 0.02), plan for feeding (p ≤ 0.001), and 4–8-week postpartum feeding type (p ≤ 0.001). Postpartum feeding type was associated with differences in admission nursery (p = 0.004), and plan for feeding (p ≤ 0.001). Discharge feeding type and postpartum feeding type were not associated with Apgar score at 1 minute or Apgar score at 5 minutes (Supplementary Table S1).
Discussion
Various studies have found that cesarean births are associated with decreased breastfeeding initiation, increased time to first breastfeed, a lower incidence of exclusive breastfeeding, delayed onset of lactation, and increased likelihood of supplementation compared to vaginal births. 40 Our study demonstrates that SSC in the OR after cesarean birth at our institution is associated with improved short-term breastfeeding outcomes, including increased rate of EBMF and reduced BMFSF among mothers who planned to exclusively breastfeed, as well as earlier breastfeeding initiation. Our findings are consistent with other research showing improved breastfeeding outcomes with early SSC after cesarean births.41,42
While the breastfeeding benefits of immediate SSC compared to no SSC are well documented, studies comparing breastfeeding outcomes by location of SSC initiation or timing of onset are lacking, especially following cesarean birth. 9 In our study, any SSC within the first 3 days following cesarean birth was associated with increased EBMF at the 4–8-week postpartum visit; however, location and timing of SSC initiation were found to be less important at this time point. Our findings are consistent with other research showing similar long-term breastfeeding outcomes between SSC initiated at different time points after vaginal birth. 43 Our findings suggest that when SSC is not possible immediately following birth, it is still beneficial to initiate SSC later after birth.
Newborn feeding plan was associated with both SSC exposure and newborn feeding type at discharge and postpartum in our study. Newborn feeding intention is well documented as a powerful predictor of short-term feeding outcomes. 44 Although it is expected that not all mothers will follow their anticipated course for newborn feeding, we would expect to see a significant association between plan for newborn feeding and actual feeding type at hospital discharge and at the 4–8-week postpartum visit. Few studies have examined the influence of breastfeeding intention on SSC practices. However, given that a positive relationship between immediate SSC and breastfeeding outcomes after vaginal births is well known, 9 it is possible that knowledge of this relationship could have biased SSC decisions made by staff and parents in our study.
Even though immediate SSC is recommended for all newborns, including clinically complex newborns, born by all modes, low Apgar scores and admission to NICU have been identified in previous studies as negative predictors of SSC at vaginal birth, and uncertainty about newborn eligibility based on clinical condition has been identified as a barrier to implementation of SSC.45–47 Our findings of (1) reduced rates of any SSC after cesarean birth when Apgar Scores are <7 and (2) reduced SSC in the OR for newborns admitted to transition nursery or NICU are consistent with findings for vaginal births, and indicate that newborn clinical instability is currently a barrier to immediate SSC for cesarean births.
In our study, SSC was initiated in the OR more often during 2020 than 2019, indicating that despite challenges related to the COVID-19 pandemic, it was feasible to undertake SSC in the OR. 48 Staff shortages have been noted as a potential reason for low rates of SSC in the OR immediately following cesarean birth. 42 During the COVID-19 pandemic, our institution continued practices to support breastfeeding, including SSC after scheduled cesarean birth.
Medical staff knowledge, staff resistance to change, and workflow issues have been identified as other potential barriers to implementing SSC in the OR; thus, the significant increase in SSC during the 2020 interval in our study could be attributed to implementation of new practice guidelines, acceptance of the change in practice by staff on the care team, and/or increased staff education about SSC in the OR.45,49 Since the completion of this study, to help alleviate future concerns about staff shortages as a barrier to SSC in the OR, and to assure that the OR circulating nurse can attend to the needs of the surgical team, we have created a dedicated postpartum nursing role to facilitate mother–newborn SSC in the OR for scheduled cesarean births.
Strengths of the study include standardized documentation of data in the EHR with few pieces of information missing. In addition, our data were collected from a single site, and from relatively homogenous cohorts that were reflective of the Iowa population. While this adds to the validity of our study when making conclusions about populations that are similar to our study population, the wider application of our results may be more difficult. Thus, a limitation of our study is that patients and practices from a Midwest regional referral center may not be generalizable to other practice settings. Another limitation of our study is the retrospective study design, which relies on accurate documentation of feeding type. These data were missing for the 4–8-week postpartum visit in 43/230 cases.
In addition, the lack of information about duration and frequency of SSC meant that we were not able to ensure a standardized SSC dose or establish a dose–response relationship in our study. Due to the observational nature of our study design, we were not able to assess causation. While we did have limited data on reason SSC was not performed in the OR, details about maternal and neonatal ineligibility would significantly add to research in this area, especially considering that clinically complex newborns may benefit most from immediate SSC. 47
Finally, due to convenience sampling, our study was limited by sample size, which may negatively affect the validity of subanalyses of disaggregated variables such as feeding type and race. Future studies should focus on identifying barriers to SSC after cesarean birth from both patient and medical staff perspectives and standardize reporting of SSC practices.
Conclusions
SSC practices after cesarean birth at our institution were positively associated with breastfeeding outcomes, including EBMF at hospital discharge and 4–8 weeks postpartum. There was an increase in SSC in the OR between 2019 and 2020, despite concerns regarding staffing and other negative impacts of the COVID-19 pandemic on maternity care. This indicates that practices that are felt to be of benefit can be implemented, despite challenging circumstances. Exploring SSC practices, including location, timing, and duration of first SSC, and breastfeeding outcomes with a larger sample size from multiple institutions would help to determine whether these results can be generalized, and would contribute to a better understanding of the complex interactions between these and other variables during the first hours following cesarean birth.
Footnotes
Authors' Contributions
S.C.: Conceptualization, methodology, formal analysis, investigation, data curation, writing—original draft, and visualization. D.S.: formal analysis, resources, data curation, and writing—review and editing. A.S.: Conceptualization and writing—review and editing. N.B.: Conceptualization, methodology, resources, writing—review and editing, supervision, and project administration.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure Statement
No competing financial interests exist.
Funding Information
Research reported in this publication was supported by the National Center For Advancing Translational Sciences of the National Institutes of Health under Award No. UM1TR004403.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.