
Abstract
Background and Objectives:
Few U.S. women meet the public health recommendations to exclusively breastfeed for 6 months and continue breastfeeding for at least 1–2 years. We compared prenatally collected demographic, health, and breastfeeding support/intention variables to examine how these factors intersect to predict meeting breastfeeding recommendations.
Methods:
PREVAIL, a CDC-funded birth cohort in Cincinnati, OH, was approved by the IRB at CDC, Cincinnati Children's Hospital, and the hospitals where enrollment (third trimester, 2017–2018) occurred. The prenatal questionnaire captured sociodemographics, pre-pregnancy weight and height, breastfeeding environment, and breastfeeding intention, while health factors were obtained from obstetrical records. Body mass index (BMI) (kg/m2) was categorized as healthy (18.5–24.9), overweight (25–29.9), obesity 1 (30–34.9), and obesity 2+ (≥35). Mothers self-reported date of exclusive and any breastfeeding cessation through quarterly postnatal questionnaires. Random forest was used for variable selection, cross-validated in multivariable logistic models.
Results:
Analysis included n = 237 mothers with BMI ≥18.5. Random forest identified BMI category, prenatal intention, and insurance type as the most important predictors of meeting breastfeeding recommendations. The resulting logistic models explained >40% of the variance with an area under the curve of ≥0.89 for both recommendations. More than 73% of the risk of not meeting breastfeeding recommendations was attributable to having an elevated BMI or lacking strong breastfeeding intention.
Conclusions:
In PREVAIL, maternal BMI and prenatal intention explained most risks of not meeting breastfeeding exclusivity and duration recommendations. Our findings suggest efforts to improve breastfeeding exclusivity and duration should focus on strengthening prenatal breastfeeding intention and identifying effective interventions for supporting breastfeeding among mothers with higher BMI.
Introduction
The American Academy of Pediatrics (AAP
Prior research has shown that a wide range of sociodemographic, support, intention, and maternal health factors are associated with breastfeeding duration.10–12 However, few studies have simultaneously adjusted for maternal health and prenatal intention or examined factors associated with meeting breastfeeding recommendations specifically. Using a CDC-sponsored birth cohort of Cincinnati-area mothers, we examined how prenatally assessed factors associated with sociodemographics, maternal health, intention, and breastfeeding environment predict meeting breastfeeding exclusivity and duration recommendations. Our goal was to identify key risk factors for not meeting recommendations to better focus research and public health policies aimed at improving U.S. breastfeeding rates.
Methods
Study design
The Pediatric Enteric and Respiratory Viral Immunogenesis Longitudinal Cohort (PREVAIL) is a CDC-funded, 2-year birth cohort in Cincinnati, OH, with rolling prenatal enrollment conducted between April 2017 and July 2018. PREVAIL was approved by the institutional review boards at the CDC, Cincinnati Children's Hospital Medical Center, and the birth hospitals where maternal enrollment and delivery occurred. PREVAIL's aim was to examine the natural history of viral disease from birth until age two, including identifying risk factors for infection and symptomatology. This study is a secondary analysis using the prenatally (3rd trimester) collected demographic, breastfeeding intention, and maternal health data and the postnatal maternal-reported dates of formula introduction and breastfeeding cessation. A full description of PREVAIL's study design was previously published; 13 methods relevant to this work are described here.
Expectant mothers were provisionally enrolled in the third trimester of pregnancy from two urban hospitals, completing a questionnaire that included sociodemographics, pre-pregnancy weight and height, and breastfeeding intentions and comfort level. Maternal health factors were abstracted from the obstetric record. Final inclusion criteria were delivery of a healthy, singleton infant, between 35 and 42 weeks of gestational age, birth weight ≥2500 g, and without known congenital anomalies, residence within 20 miles of the birth hospitals, ownership of a cell phone capable of receiving text-administered surveys, and completion of a 2-week postnatal home visit. Participants with a history of illicit drug use during pregnancy or maternal HIV infection were excluded.
Exposure variables
Breastfeeding predictors were selected based on variables consistently identified in the literature 12 and collected prenatally in PREVAIL 13 from the following domains: sociodemographic (race, income, education, and insurance type), maternal health (BMI category, maternal age at birth, delivery mode, and diabetes during pregnancy), and breastfeeding environment (living with a partner, parity, prenatal counseling, comfort level, birth hospital, and intention strength). Race was defined as “Black” or “White or Other.” Due to the small number of participants (<5%) who identified as “Other” (Asian and multiracial), this category was not evaluable on its own and combined with White. In addition, the small proportion of mothers who identified as Hispanic (<3%) were evenly split between Black and White families, and thus were not evaluated as a separate category.
Family income was categorized as above or at/below the Cincinnati median family income (>$50,000/year or ≤$50,000/year). 14 Insurance status was classified as public or private. Maternal education was based on completion of at least 2 years of postsecondary training/education or not. Mothers were classified as living with a partner or not, independent of marital status. Maternal age was calculated at the child's date of delivery and dichotomized as greater/equal versus under the median age of the cohort. The presence of any prenatal diagnosis of diabetes (Type I, Type II, or gestational) was coded as diabetes in pregnancy. Delivery mode was categorized as vaginal or c-section.
Maternal height and pre-pregnancy weight were self-reported at enrollment. 15 BMI (kg/m2) was calculated and categorized as healthy (18.5–24.9), overweight (25–29.9), class 1 obesity (30–34.9), or ≥class 2 obesity (≥35, obesity 2+). Although prenatal underweight (BMI <18.5) has been associated with reduced duration of breastfeeding, 16 this study was not powered to examine underweight as a separate group and so excluded mothers in this category from analysis. All PREVAIL participants with a pre-pregnancy BMI ≥18.5 were included in this study.
Both birth hospitals, The University of Cincinnati Medical Center (UCMC) and The Christ Hospital, Cincinnati (TCH), have policies in place to promote, protect, and support breastfeeding. UCMC is a certified Baby Friendly Hospital, 17 and serves as the region's public hospital. TCH is a private hospital and is not certified as Baby Friendly, but participates in Ohio's First Steps for Healthy Babies program, 18 which encourages, but does not require adherence to the Baby Friendly 10 Steps for Successful Breastfeeding. 17
At the prenatal enrollment visit, breastfeeding intention was assessed using the Infant Feeding Intentions Scale, 19 a validated 5-question, 5-point Likert scale. Based on maternal response to “When my baby is 6 months old, I will be breastfeeding my baby without using any formula or other milk,” intention to exclusively breastfeed was categorized as strong (“very much” agree), moderate (“somewhat” agree), neutral (“unsure”), or weak (“somewhat” or “strongly” disagree). The prenatal survey also asked if the mother had received any type of prenatal breastfeeding counseling (yes/no) and her level of comfort with the “idea of breastfeeding” on a 4-point Likert scale. 20 Comfort level was categorized as high (very comfortable), moderate (either of the “somewhat” responses), or low (very uncomfortable).
Outcome variables
Maternally reported date of first formula use and date of breastfeeding cessation were collected on postnatal surveys administered at postnatal weeks 2, 6, and 16 and then quarterly from 6 to 24 months until breastfeeding cessation was reported. 13 Time to formula introduction and breastfeeding cessation for participants who were lost to follow up was imputed using the date of last known exclusive or any breastfeeding, respectively. All references to breastfeeding include any provision of the mother's own milk—at the breast, expressed and provided by bottle, or in combination. Meeting the exclusive breastfeeding recommendation was defined as no use of infant formula before 5 ½ months of age without consideration of complementary foods. Breastfeeding to 1 year was defined as providing any level of breastfeeding until the child's first birthday.
Statistical plan
Our statistical approach was designed to identify key predictors of meeting breastfeeding recommendations using variables related to sociodemographics, maternal health, and breastfeeding environment. Fisher's exact test was used to test bivariate associations between proportions of each categorical variable and meeting breastfeeding exclusivity and duration recommendations. Univariable logistic regression compared odds of meeting breastfeeding recommendations by each variable.
To select variables that provided the most predictive models, all 14 exposure variables were used to train random forest algorithms. Random forest is a supervised machine-learning approach based on classification and regression tree (CART) analysis and assesses how variables function relative to each other in terms of reducing prediction error. 21 CARTs for each outcome are constructed by first randomly selecting about two-thirds of the data into a subset representing one “tree.”
Variables are scored based on how much error in the tree is increased (accuracy) and how much less homogenous each split point is (purity) when excluding each variable from consideration. This process is repeated and resulting scores from each tree are then combined (forest) and averaged to determine the mean accuracy and purity scores associated with each variable across the entire forest. For this analysis, we constructed a forest of 1000 trees for each outcome (minimum node size of 3), selecting variables for final model inclusion, which were above the third quartiles of mean purity and accuracy scores. 22
Cross-validation was performed by including the selected set of variables into a multivariable logistic model and calculating the resulting Area Under the Receiver Operator Characteristic Curve (AUROC). The percent of variance explained (R
2
) and test classification error rate, indicating the percentage of erroneous prediction, was calculated for each final model. Comparison models were then constructed using any clearly demarcated predictor identified and the resulting model's predictive value was compared using DeLong's test for correlated ROC curves. If the predictive value was at least adequate for these parsimonious models, attributable risk was calculated using the formula  . Predictive value is considered adequate with an AUROC from 0.70 to 0.79, excellent from 0.80 to 0.89, and outstanding if ≥0.90.
23
. Predictive value is considered adequate with an AUROC from 0.70 to 0.79, excellent from 0.80 to 0.89, and outstanding if ≥0.90.
23
Posthoc power analysis found that we had at least 80% power to detect a moderate to large effect size using all statistical methods. Sensitivity analysis was performed on all analyses by excluding participants who identified as Other, by re-categorizing Other as Black race, and by removing participants with imputed exclusive or any breastfeeding duration from all analyses. All analyses were completed using the R Environment for Statistical Computing (version 4.2.3 “Shortstop Beagle”), including the randomForest and pROC packages.22,24
Results
This analysis included n = 237 participants with BMI ≥18.5 kg/m2; of the 245 enrolled in PREVAIL, 8 (3%) were excluded due to pre-pregnancy underweight. Table 1 summarizes the sociodemographic, maternal health, and breastfeeding environment characteristics of the cohort. The cohort was racially and economically diverse and births were evenly split between the public and private hospital. Although breastfeeding initiation rates were high (87%, n = 207), only 17% (n = 41) of mothers met exclusivity recommendations, 23% (n = 54) continued any breastfeeding until the child's first birthday, and 14% (n = 33) met both recommendations.
Characteristics of the Cohort
Bolded values represent variables that met criteria for statistical significance (p < 0.05).
Black race includes participants who identify as Black only. White participants and those who identified as multiracial or other than Black or White (<5%) were categorized as White or Other.
Participants without insurance and those who listed both private and public insurance were classified as publicly insured.
Cohort median maternal age at child's birth: 29.6 years (IQR 25.8–33.2).
Healthy (BMI 18.5–24.9), Overweight (BMI 25–29.9), Obesity 1 (BMI 30–34.9), Obesity 2+ (BMI ≥35).
Prenatal diagnosis of Type I diabetes, Type II diabetes, or gestational diabetes.
Measured in third trimester using the Infant Intentions Feeding Scale. 19
UCMC = University of Cincinnati Medical Center (public); TCH = The Christ Hospital, Cincinnati (private).
Study characteristics of participants in the Pediatric Respiratory and Enteric Viral Acquisition and Immunogenesis Longitudinal Cohort (PREVAIL), a 2-year birth cohort conducted in Cincinnati, OH, from April 2017 to August 2020. Maternal pre-pregnancy weight was self-reported at baseline and height was abstracted from the obstetrics records. Body mass index (BMI) was calculated as kg/m2, and classified as healthy (18.5–24.9), overweight (25–29.9), obesity 1 (30–34.9), and obesity 2+ (≥35). Maternal intention to exclusively breastfeed to 6 months of age was determined prenatally using the Infant Feeding Intentions Scale. 19 Mothers who responded “very much agree” to the statement, “When my baby is 6 months old, I will be breastfeeding my baby without using any formula or other milk,” were classified as having a strong prenatal intention, those who responded “somewhat agree” were categorized as moderate intention, and those who responded either “neutral” or any disagreement category were categorized as neutral or weak, respectively. Omnibus comparisons of expected proportions were made using Fisher's exact test.
In unadjusted logistic regression models (Table 2), only two predictors (maternal age and parity) showed no association (p > 0.10) with exclusive breastfeeding to 6 months; and only four predictors (parity, diabetes in pregnancy, prenatal breastfeeding counseling, and delivery mode) showed no association with any breastfeeding to 1 year. Random forest identified three variables with a mean accuracy and purity score above the third quartile for both the exclusive and any breastfeeding outcomes (Supplementary Table S1): prenatal breastfeeding intention, BMI category, and insurance type. In addition, maternal education met inclusion criteria for predicting any breastfeeding to 1 year. When plotted, a clear delineation between intention and BMI and the remaining variables was observed (Supplementary Fig. S1).
Univariable Regression Models for Meeting Exclusive and Any Breastfeeding Recommendation in the PREVAIL Cohort
Reference values (resp.): White or Other, income>$50,000/year, private insurance, ≥2 years postsecondary education, primiparous, age above median, vaginal birth, healthy BMI, no diabetes, lives with partner, received counseling, high comfort level, strong prenatal intention, TCH.
Bolded values represent variables that met criteria for statistical significance in univariable models (p < 0.05).
Black race includes participants who identify as Black only. White participants and those who identified as Other (<5%) were categorized as White or Other.
Cohort median maternal age at child's birth: 29.6 years (IQR 25.8–33.2).
Healthy (BMI 18.5–24.9), Overweight (BMI 25–29.9), Obesity 1 (BMI 30–34.9), Obesity 2+ (BMI ≥35).
Prenatal diagnosis of Type I diabetes, Type II diabetes, or gestational diabetes
Measured in third trimester using the Infant Intentions Feeding Scale. 19
Birth hospitals: UCMC = University of Cincinnati Medical Center (public); TCH = The Christ Hospital, Cincinnati (private).
Odds Ratios (OR) reflect univariable odds, calculated using logistic regression. R2 represents the proportion of variance explained by the exposure variable.
In the resulting multivariable logistic models (Fig. 1), elevated BMI, not having a strong prenatal intention, and public insurance were associated with significantly lower odds of achieving either breastfeeding outcome. While maternal education was included in the multivariable logistic modeling of any breastfeeding to 1 year, it did not achieve statistical significance. In cross-validation (Fig. 2), both multivariable logistic models had an excellent to outstanding predictive value (AUROC = 0.90 and 0.89 for exclusive and any breastfeeding models, respectively), explained >40% of the variance, and recorded a test classification error rate of 12.2% and 19.8%, respectively.

Random forest feature selection (1000 trees, minimum node number = 3) was used to select the most parsimonious models with the highest predictive accuracy based on a resulting mean decrease in accuracy and mean decrease in Gini purity score above the 3rd quartile of scores. Variables for inclusion in the random forest models were collected prenatally and selected from the following domains: sociodemographic (race, income, education, and insurance type); maternal health (age, delivery mode, BMI category, and diabetes in pregnancy), and breastfeeding environment (lives with partner, parity, birth hospital, receipt of counseling, comfort level with breastfeeding, and intention). Pre-pregnancy BMI was categorized as follows: healthy (18.5–24.9), overweight (25–29.9), obesity 1 (30–34.5), or obesity 2+ (≥35). Panels illustrate the forest plots of the resulting models predicting exclusive breastfeeding to 6 months of age
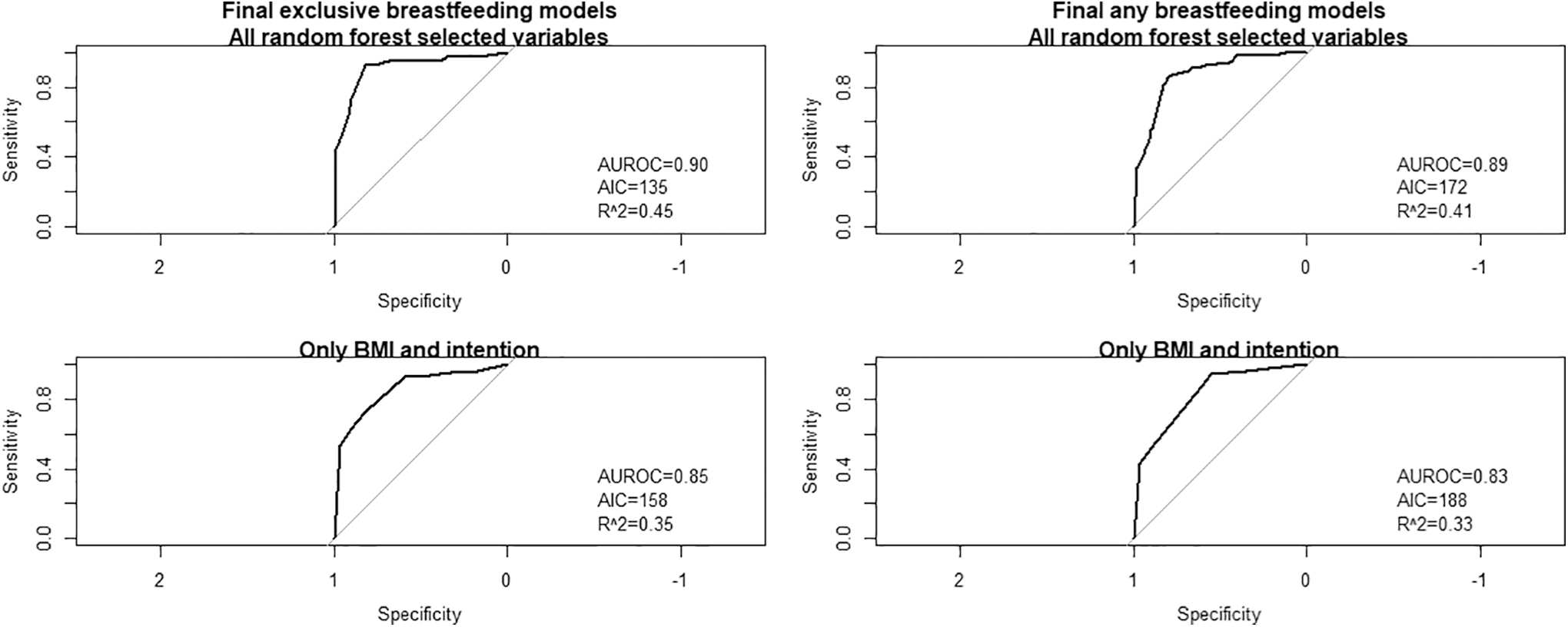
Random forest feature selection (1000 trees, minimum node number = 3) was used to identify the most parsimonious models with the highest predictive accuracy based on a resulting mean decrease in accuracy and mean decrease in Gini purity score above the 3rd quartile. Variables for selection in final models included maternal pre-pregnancy BMI [healthy (18.5–24.9) vs. overweight (25–29.9), obesity 1 (30–34.5), or obesity 2+ (≥35)], prenatal breastfeeding intention (strong vs. not strong), and insurance type (private vs. public). The any breastfeeding model also included maternal education level (2 or more years postsecondary vs. not). Cross-validation of the resulting logistic models was made by calculating the resulting area under the receiver operator characteristic curves (AUROC, ≥0.70 adequate), Akaike Information Criterion (AIC, lower is better), and proportion of variance explained (R 2 , higher is better).
As BMI and intention were clearly demarcated in the random forest output (Supplementary Fig. S1), final regression models using only these variables were also constructed (Supplementary Table S2) and the resulting predictive value was compared to the full models (Fig. 2). Although the predictive values of these more parsimonious models significantly differed from that of the full models (z = 2.20, p = 0.028 and z = 2.53, p = 0.011 for exclusive and any breastfeeding models, respectively), the estimates for the effects of BMI and intention did not significantly vary and the models retained excellent predictive value (AUROC = 0.85 and 0.83, respectively).
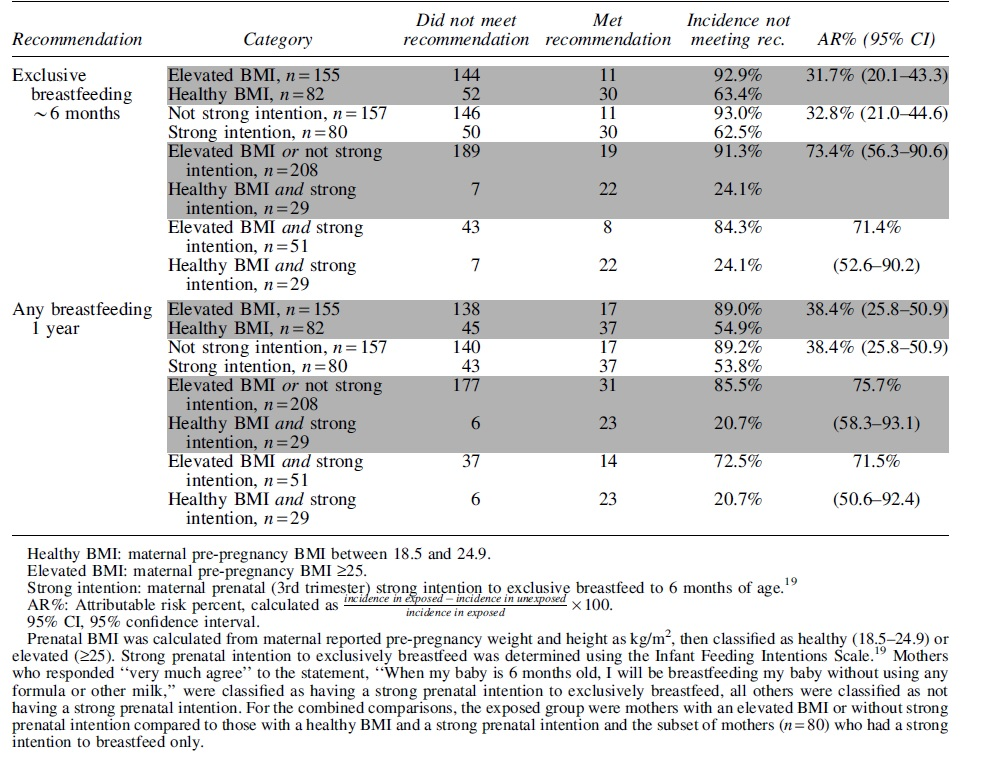
Comparisons of the prevalence of meeting exclusive and any breastfeeding recommendations by BMI category and intention can be found in Figure 3. Incidence of not meeting the exclusivity recommendation was over 91% of those with an elevated BMI or without a strong prenatal intention (Table 3), with 73% of the risk of not meeting exclusive recommendations attributable to these factors compared to mothers with a healthy BMI and strong intention. Comparing only those participants who had a strong prenatal intention to exclusively breastfeed did not significantly alter the estimates; 71% of the risk of not exclusively breastfeeding to 6 months was attributable to an elevated BMI in the strongly intentioned group. Calculations for incidence and attributable risk percent for not meeting the recommendation for any breastfeeding followed a similar pattern to those for not meeting the exclusive breastfeeding recommendation.

Proportions of mothers who met exclusive breastfeeding (∼6 months) and any breastfeeding (1 year) recommendations by pre-pregnancy BMI category in the PREVAIL cohort
Attributable Risk of Not Achieving Public Health Breastfeeding Recommendations by Body Mass Index and Prenatal Breastfeeding Intention in the PREVAIL Cohort
After excluding the 11 (4.6%) participants who identified as “Other” race, sensitivity analysis found no significant difference in any outcome or when re-categorizing these participants as Black. Excluding mothers with imputed exclusive and any breastfeeding duration based on last known breastfeeding status (n = 18, 7.6%) did not result in a significant change in any outcome.
Discussion
Despite high breastfeeding initiation rates, fewer than 20% of mothers in the PREVAIL cohort met the public health recommendation to exclusively breastfeed their infant to about 6 months of age and less than 25% met the recommendation to continue breastfeeding for 1 year. These rates closely parallel 2019 national surveillance data, which show that 25% of U.S. children are exclusively breastfed to 6 months of age and only 36% are breastfed to age one. 4 When comparing the individual established risk factors for early breastfeeding cessation, we found significant differences in meeting recommendations by most variables within sociodemographic, maternal health, and breastfeeding environment domains. However, when combining and selecting variables using a machine-learning approach, we found that BMI category and strength of prenatal intention were, by far, the strongest drivers of meeting recommendations.
To our knowledge, an analysis of data from the Healthy Start Study by Kaar et al. 25 is the only other contemporary examination of factors associated with adherence to U.S. breastfeeding recommendations. Kaar examined factors associated with adherence to the AAP infant feeding recommendations in 835 mother-infant dyads residing in the Denver, Colorado area, finding that 40% exclusively breastfed to about 6 months and 36% continued to breastfeed to at least 1 year.
The higher rates in their study may be due to differences in populations or reporting. In contrast to the close surveillance of infant feeding in PREVAIL, Healthy Start reported infant feeding history at two time points (about 5 months and 22 months postpartum). Also, exclusive breastfeeding cessation in Healthy Start was based on age at initiation of daily formula use, whereas in this analysis, it was based on age at first formula use. However, despite differences in reporting methodology, Kaar also reported a negative association between elevated pre-pregnancy BMI and adherence to infant feeding recommendations.
Our study is the first to our knowledge to examine strength of breastfeeding intention and BMI class in the same models. In our study, more than 73% of the risk of not meeting either recommendation was attributable to having either an elevated BMI or a lack of strong prenatal intention. These two variables explained the highest percentage of variance in univariable models, were clearly demarcated in the random forest output, remained strong, independent, and significant predictors within the final multivariable models, and their effects did not significantly change when other sociodemographic variables were excluded from the models.
However, when comparing only those mothers with a strong prenatal intention, we found that mothers with a healthy BMI exceeded the Healthy People 2030 goals for exclusivity and duration, 5 but fewer than 30% of mothers with an elevated BMI met either recommendation. Indeed, when comparing only those mothers with a strong prenatal intention to breastfeed, the attributable risk of not meeting either recommendation remained over 71% for both recommendations among mothers with an elevated BMI. These findings suggest that unique breastfeeding barriers exist for mothers with elevated BMI, which are not related to prenatal intention strength.
A myriad of factors may explain this relationship. For example, women with elevated BMI may experience weight stigma among health care providers; specifically, women with obesity are less likely to experience breastfeeding supportive maternity care, and their infants are more likely to require medically indicated formula supplementation.26–28 The risk of delayed lactogenesis also increases with increasing BMI category, and there is emerging evidence that physiologic conditions more common among women with elevated BMI, such as suboptimal metabolic health and inflammation, may impede milk production.29,30 While we did not ascertain reasons for first use of infant formula or breastfeeding cessation, concern about milk supply is a frequently cited reason for formula use31,32 and is more commonly reported by mothers with obesity,33,34 suggesting, at least partially, an underlying metabolic explanation for these differences in breastfeeding rates.
These possible explanations for disparities by elevated BMI may also explain why Black race, strongly predictive of both outcomes in univariable analysis and a frequently reported predictor of breastfeeding disparities in the literature,10–12 did not meet criteria for inclusion in either breastfeeding prediction model. In a separate analysis of the same cohort examining markers of systemic racism as predictors of mothers meeting their own prenatal breastfeeding goals, 35 our group found that a mediation model, including obesity, diabetes, delivery mode, and insurance type significantly, but not completely, attenuated the disparities in breastfeeding duration in Black versus White mothers.
This may be because Black mothers face barriers similar to those faced by mothers with obesity, including less health system support for breastfeeding and reduced exposure to evidence-based interventions that promote and enable breastfeeding.6,36,37 Given the significantly higher rates of obesity in our study among Black mothers, this collinearity of exposures may have reduced race's importance in the predictive models. However, it should be noted that due to the strong correlation between race and obesity rates in the United States, 38 identifying and addressing breastfeeding challenges uniquely faced by women with elevated BMIs may have a disproportionate effect on reducing disparities in breastfeeding found by race.
When controlling for other sociodemographic factors, obesity category and intention, public insurance was the sole socioeconomic indicator that remained a significant predictor in our models. This may be because public insurance is strongly correlated to, and thus acts as a proxy for the intersection of, a wide range of socioeconomic factors, including income, education, and career type, all of which are associated with multiple barriers to breastfeeding. For example, access to public insurance is based on income level, so mothers who qualify for public insurance may be more likely to a hold lower-wage job, such as hourly shift-work, which is associated with lack of paid maternal or family leave, 39 shown to be predictive of reduced duration of exclusive and continued breastfeeding.40,41
We found that the risk of not meeting breastfeeding recommendations was similar across all elevated BMI categories, which contrasts with two large perinatal cohort studies that identified a dose–response association with increasing BMI.16,25 This may be due to differences in methodology, rather than effect. For example, Kaar and colleagues 42 defined the outcome of “adherent” as meeting all three AAP breastfeeding recommendations (exclusive breastfeeding to 6 months, continued breastfeeding to 1 year, and no introduction to complementary foods before 6 months) compared to those who did not meet all three recommendations, using BMI as a continuous variable, and then summarized the estimates into 5-unit increments for reporting.
Similarly, the dose–response reported in Winkvist et al. was only in the subset of mothers who had an elevated pre-pregnancy BMI and reported higher gestational weight gain than recommended. 16 Kaar et al. did not report differences by individual recommendation, and Winkvist et al. did not find differences among mothers with gestational weight gain either below or within recommendations.
The Baby Friendly Hospital initiative has been an important guide for setting hospital policies that promote, protect, and support breastfeeding. 17 We did not find that giving birth in a certified Baby Friendly Hospital was associated with improved odds of meeting either recommendation. However, in Cincinnati, the larger, publicly funded hospital (UCMC) is certified as Baby Friendly, while the private hospital (TCH) has policies in place in line with the Baby Friendly Hospital initiative, 18 but has not sought certification.
This skewed the proportions in each hospital in variables we found to be associated with lower rates of achieving breastfeeding recommendations, such as obesity prevalence (51% UCMC vs. 33% TCH, p = 0.006) and public insurance use (71% UCMC vs. 24% TCH, p < 0.001). Indeed, the Baby Friendly policies in place at both hospitals may have reduced disparities by commonly reported socioeconomic predictors in our cohort, such as income and education level.
This work is not without limitations. While not possible to draw causal inference from observational data, the prospective nature of our study provided temporality to our findings and reduced recall bias in both intention and cessation reporting. Although our study was adequately powered to detect moderate differences in proportions and odds of meeting recommendations, the modest sample size resulted in small numbers who met exclusivity and duration goals when parsed by many sociodemographic categories, limiting our power to observe significant differences by these factors. Furthermore, while our cohort was representative of hospitals from which we recruited and enrolled participants, compared to the greater Cincinnati area, our study was overrepresented in Black (44% vs. 11%) and lower income (51% vs. 36%) families. 14
Finally, our region has seen a differential increase in breastfeeding initiation rates in Black compared to White mothers between 2015 and 2019, resulting in a significant decline in the Black-White disparity in initiation rates during the time of our study (23% in 2015 vs. 12% in 2019). 43 Thus, our findings may not be generalizable to a rural or suburban population or in a region without the concerted, community-based efforts being undertaken in our area, but may offer evidence to support the work being done to promote and support breastfeeding among urban Cincinnati families.
This study also has several strengths. The random forest approach allowed for an unbiased assessment of how established risk factors performed relative to each other and identified possible foci for future research and public health interventions. The prenatal collection of intention data removed the potential for biased recall of intentions after breastfeeding has ceased and the prospective and regular collection of breastfeeding exclusivity and duration data allowed for accurate estimates of the timing of these events. Our finding of the persistence of breastfeeding disparities in women with elevated BMIs, despite strong prenatal intentions, is a novel finding and a call to identify unique barriers faced by these mothers to develop interventions tailored to their specific needs.
Conclusion
In the PREVAIL cohort, mothers with a healthy BMI and a strong prenatal intention were far more likely to meet breastfeeding exclusivity and duration recommendations, and a lack of either of these factors explained over 73% of the risk of not meeting either guideline. While strong prenatal intention significantly improved odds of achieving breastfeeding recommendations in mothers with a healthy pre-pregnancy BMI, our findings suggest mothers with an elevated BMI face barriers to achieving their breastfeeding goals independent of their prenatal intention to breastfeed. Studies focused on barriers that mothers with an elevated BMI face to meet their own breastfeeding goals are urgently needed.
Footnotes
Acknowledgments
We gratefully acknowledge the participation of the PREVAIL birth cohort families and the hard work of the dedicated PREVAIL and Schubert Research Center staff. We would especially like to thank Dr. Dan Payne and Claire Mattison at the CDC for providing support and guidance during the study.
Authors' Contribution
S.C.C. conceived and designed the project, completed the data analysis, and was the primary author of all drafts. L.N.-R. and A.L.M. contributed to the conceptualization and design of the study, the acquisition of data, and interpretation of analysis, and wrote significant portions of the initial draft. M.A.S. and A.R.B. contributed to study design and acquisition of data. D.H.T. and D.M.W. contributed to the analysis and interpretation of data and to writing the ![]() section. All authors participated in the revision of drafts and approved the final article. All authors agree to be accountable for all aspects of the work.
section. All authors participated in the revision of drafts and approved the final article. All authors agree to be accountable for all aspects of the work.
Disclosure Statement
The authors have no conflicts of interest relevant to this article to disclose.
Funding Information
The PREVAIL Cohort was funded by a cooperative agreement from the U.S. Centers for Disease Control and Prevention (IP16-004), with additional support provided by the Molecular Epidemiology in Children's Environmental Health Training program (5 T32 ES 10957-18) and the National Center for Advancing Translational Sciences of the National Institutes of Health, under Award Number UL1TR001425. Data analysis and article preparation were funded by the MOM2CHild study (R01HD109915, Morrow, PI). The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the U.S. Centers for Disease Control and Prevention or National Institutes of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.