
Abstract
Objectives:
To investigate SARS-CoV-2 specific immunoglobulin A (sIgA) in breast milk of Thai mothers post COVID-19 vaccination and/or SARS-CoV-2 infection, and to compare the sIgA among lactating mothers with varying COVID-19 vaccination regimes.
Materials and Methods:
A longitudinal study was conducted in lactating mothers receiving ≥2 doses of COVID-19 vaccine or confirming SARS-CoV-2–positive test as a part of an infant feeding survey. Vaccination and infection details were collected through questionnaires and interviews. Self-collected breast milk samples (15 mL) at 1, 3, and 6 months postvaccination or infection were analyzed for sIgA through enzyme-linked immunosorbent assay (ELISA).
Results:
Eighty-eight lactating mothers (152 milk samples), average age of 30.7 ± 6.2 years, were recruited. Fifty-five percent of milk samples were from lactating mothers with both SARS-CoV-2 infection and vaccination (hybrid immunity); 40% were from those with vaccination alone (COVID naïve). Sixty percent of lactating mothers received mixed types of vaccines. Median sIgA ratio in breast milk was 2.67 (0.82–7.85). Breast milk sIgA at 1, 3, and 6 months were higher in mothers with hybrid immunity than in COVID naïve (geometric mean [95% confidence interval]: 3.30 [2.06–5.29] versus 1.04 [0.52–2.04], 3.39 [2.24–5.13] versus 1.26 [0.77–2.06], 4.29 [3.04–6.06] versus 1.33 [0.74–2.42], respectively). No significant differences were observed among various vaccination regimes.
Conclusion:
sIgA against SARS-CoV-2 was detected in breast milk for up to 6 months after immunization together with infection at a greater level than after immunization or infection alone. This immunity could be transferred and protective against SARS-CoV-2 infection. Discontinuation of breastfeeding among mothers who received COVID vaccination or experienced infection should be discouraged. Clinical Trial Registration number: TCTR20220215012.
Introduction
An outbreak of COVID-19 caused by a novel coronavirus, namely SARS-CoV-2, started at the end of 2019. This pandemic resulted in a disruption of daily-life activities and impacted the global health care system. Furthermore, COVID-19 has had a significant effect on peripartum and postpartum clinical practice, especially breastfeeding. Previous studies found that the exclusive breastfeeding rate significantly decreased during the lockdown period.1,2 This might result from concerns about viral transmission through breastfeeding as well as the lack of health personnel support.
Previous evidence has established that immunoglobulin A (IgA) in human milk can protect an infant from invading pathogens by preventing pathogen adherence and penetration into the epithelium without causing harmful inflammation. 3 Lactating mother can secrete IgA specific to an antigen when she is infected or immuned by vaccination, and then transfer it to an infant through breast milk. Data from an earlier study suggested that lactating mothers with history of pertussis and influenza vaccination during pregnancy could produce specific IgA (sIgA) against these specific pathogens and protect their breastfed infants from these respiratory diseases. 4 Similarly, sIgA against the SARS-CoV-2 virus can be identified in the breast milk of mothers who recovered from COVID-19 or received the COVID-19 vaccination.5–8
Globally, >700 million people were infected with the SARS-CoV-2 virus. 9 Likewise, Thailand has experienced the COVID-19 pandemic; there have been ∼5 million Thai people, including pregnant women and lactating mothers, confirmed cases of COVID-19. 9 Since the end of December 2020, several types of COVID-19 vaccines were gradually approved and administered globally. Nevertheless, Thailand's COVID-19 national vaccination program differed from Western countries due to the vaccine shortage.
Thai people, including lactating mothers, were recommended to receive either 2 doses of killed vaccine, 1 dose of killed vaccine plus 1 dose of viral vector vaccine, or 2 doses of messenger RNA (mRNA) vaccine as the primary series of the COVID vaccine. The booster consisted of either the mRNA vaccine or viral vector vaccine. These vaccination programs might bring forth some differences in the level of sIgA antibodies in both serum and breast milk. Moreover, some lactating mothers were infected with SARS-COV-2 and received the COVID-19 vaccination, which may alter the sIgA level in human milk.
Therefore, this study aimed to investigate the level of sIgA against SARS-CoV-2 in the breast milk of Thai mothers who received different regimes of COVID-19 vaccination as well as the mothers who were proven or suspected to be infected with the SARS-CoV-2. A better understanding of breast milk immunity against SARS-CoV-2 could possibly reassure the mothers and health care professionals regarding the benefit of breastfeeding during this difficult situation.
Materials and Methods
Study design and study population
This observational study is a part of the ongoing study entitled “Infant feeding survey during COVID-19 pandemic (TCTR20220215012).” The data were collected between March and December 2022.
Thai lactating mothers were enrolled from postpartum wards of the King Chulalongkorn Memorial Hospital, Bangkok, Thailand and several social networks. The inclusion criteria included lactating Thai mothers of healthy, singleton-born infants and those who either received at least 2 doses of COVID-19 vaccination, or those who had a positive test for SARS-CoV-2 detection by polymerase chain reaction (PCR) test or antigen test kit (ATK) within 6 months before breast milk sample collection. We excluded mothers of any infants born preterm or having congenital diseases.
This study was approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University, IRB number 956/64.
Data collection
Demographic data and history of COVID-19 vaccination and/or infection
Demographic data, including maternal age, prepregnancy body mass index, gestational age, parity, pregnancy complication, family income as well as infant data, including gender, birth weight, and mode of delivery, were gathered by a recruitment nurse. The types, frequency, and timing of COVID-19 vaccination or documented history of SARS-CoV-2 infection were collected using a self-administered questionnaire. All answers were verified through interviews by phone with research assistants.
sIgA against SARS-CoV-2 in human milk
Human milk samples were collected to assess the sIgA against SARS-CoV-2 at 1, 3, and 6 months after the mothers receiving the last doses of COVID-19 vaccination or being infected with SARS-CoV-2. The mothers were instructed to pump 15 mL of breast milk into a provided sterile container and store in the home freezer. The specimens were then picked up by the research team in an insulated box and kept at −20°C until analysis.
The sIgA to SARS-CoV-2 in human milk was analyzed by semiquantitative enzyme-linked immunosorbent assay (ELISA) using the anti-SARS-CoV-2 ELISA test kit (EUROIMMUN, Lübeck, Germany). First, breast milk samples were centrifuged for 10 minutes at 800g and 4°C, to remove fat from the milk. Then, the skimmed breast milk samples were diluted 1:25 and mixed with peroxidase-labeled anti-SARS-CoV-2 sIgA antibody using automated ELISA processing (EUROIMMUN Analyzer I-2P).
The color from the binding between the antibody and enzyme is directly proportional to the sIgA concentration in the samples. The outcomes of the quantitative measurement were transformed into standardized binding antibody units (BAU/mL). According to the manufacturer's instructions, semiquantitative test results were expressed as a ratio of the extinction of test sample and calibrator. The manufacturer's guidelines did not provide cutoff values for breast milk samples.
Statistical analysis
The statistical analyses were performed using Stata 17.0 (StataCorp., College Station, TX). Normality was checked before analysis using histogram and the Kolmogorov test. The categorical data including parity, pregnancy complication, family income, mode of delivery, infant gender, details of COVID-19 vaccination and infection, as well as the proportion of samples tested positive for sIgA against SARS-CoV-2 were shown as a number and percentage. The continuous data, including maternal age, gestation, and infant birth weight, were presented as the mean with standard deviation. The differences in mean and proportion between groups were obtained by analysis of variance and chi-square test or Fisher's exact test, respectively.
The geometric mean and geometric mean ratios (GMRs) with 95% confidence interval of sIgA were calculated by two independent sample t tests. All statistical tests were two sided, and p < 0.05 was considered statistically significant.
Results
A total of 162 lactating mothers met the inclusion criteria, but 74 participants were excluded due to reported low breast milk supply (58%), inconvenience in collecting breast milk samples (32%), and loss to follow-up (10%). Therefore, 88 lactating mothers participated in this study, and 152 milk samples were available for analysis (Fig. 1). Notably, half of the participants received the complete primary series of COVID-19 vaccination and had history of SARS-CoV-2 infection, whereas ∼40% of the lactating mothers in this study received the COVID-19 vaccination without any SARS-CoV-2 infection.
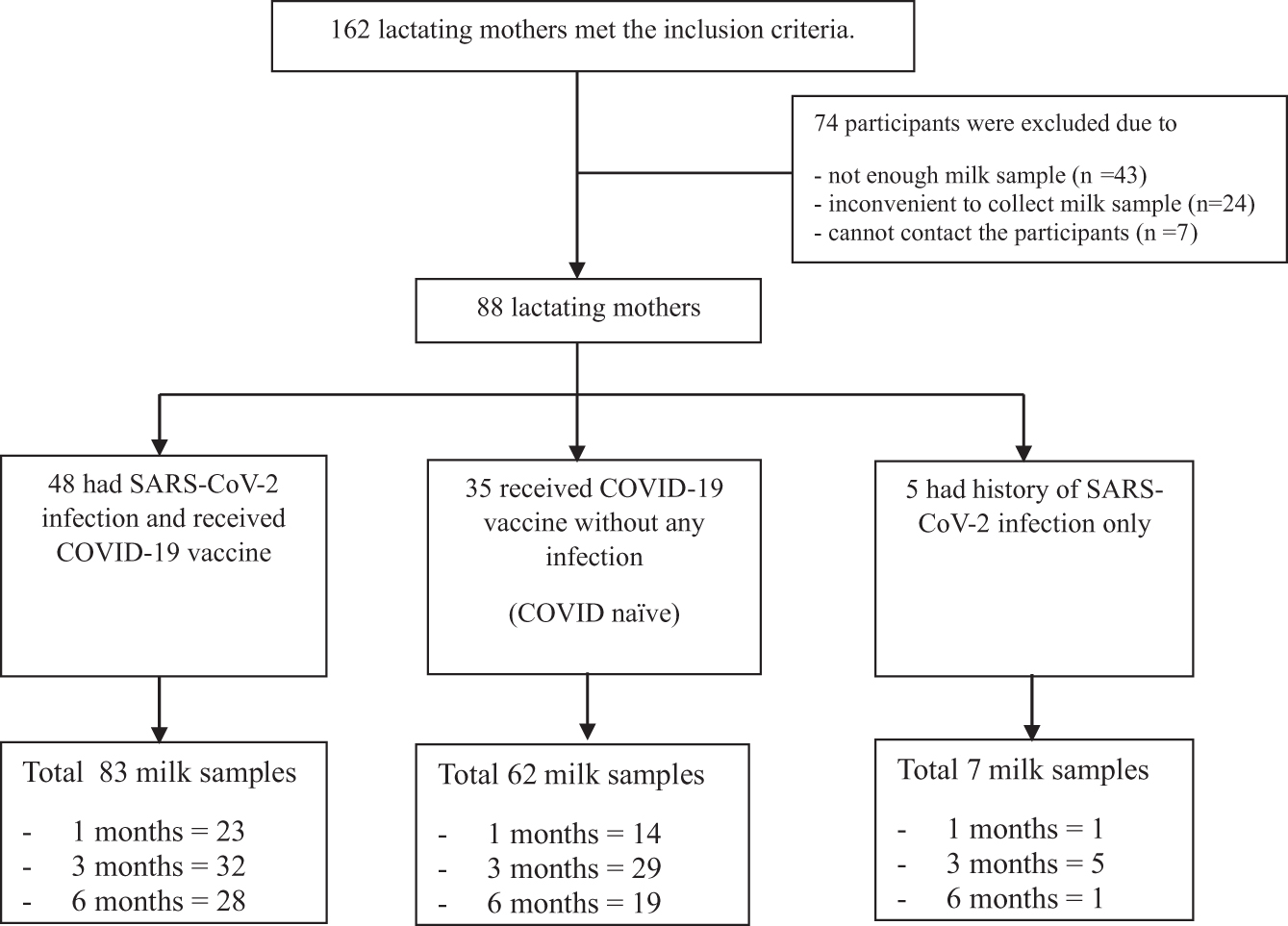
Details of participants and milk samples.
Demographic data and history of COVID vaccination or infection
Table 1 shows the baseline characteristics of lactating mothers and their infants. The average age of lactating mothers was 30.7 ± 6.2 years. Around half of lactating mothers were from low and middle socioeconomic statuses. A significantly higher number of mothers, who received COVID-19 immunization without experiencing infection, belonged to middle-to-high income families. There were no differences in the prevalence of pregnancy complications, lactation period, infants' birth weight, and mode of delivery between the groups.
Comparison of Clinical Characteristics Between the Three Groups of Participants
Values are presented as mean ± SD for continuous variables. Categorical variables were expressed as n (%). Differences in mean and proportion were obtained by ANOVA and chi-square test or Fisher's exact test, respectively.
ANOVA, analysis of variance; BMI, body mass index; SD, standard deviation.
The history of COVID-19 vaccination of the lactating mothers in this study is presented in Table 2. Eighty-one participants (92%) received complete primary series of COVID-19 vaccination. However, five participants did not receive any COVID-19 vaccine, while two received only 1 dose of the vaccine and were infected with SARS-CoV-2. Nearly 60% received mixed types of vaccines (51% mRNA vaccine+vector-based vaccine, 32% mRNA vaccine+killed virus vaccine, 15% all types of vaccines, and 2% vector-based vaccine+killed virus vaccine).
History of COVID-19 Vaccination and SARS-CoV-2 Infection
Details of mixed types of vaccinations: mRNA+vector based (n = 24); mRNA+killed virus based (n = 15); vector+killed vaccine (n = 1), all types (n = 7).
Method of detecting SARS-CoV-2 infection: ATK (n = 44); PCR (n = 9).
ATK, antigen test kit; mRNA, messenger RNA; PCR, polymerase chain reaction.
Around half of them received
sIgA against the SARS-CoV-2 in human milk after the vaccination and/or infection
Overall, the median sIgA ratio in the breast milk of lactating mothers was 2.67 (0.82–7.85). After comparing the sIgA between lactating mothers who received the COVID-19 vaccination and those who had a history of SARS-CoV-2 infection, the result revealed that sIgA at 1, 3, and 6 months of lactating mothers who received the immunization and had a history of the infection (hybrid immunity) was significantly higher than those who received the COVID vaccines without a history of SARS-CoV-2 infection (COVID naïve) (Table 3 and Fig. 2).
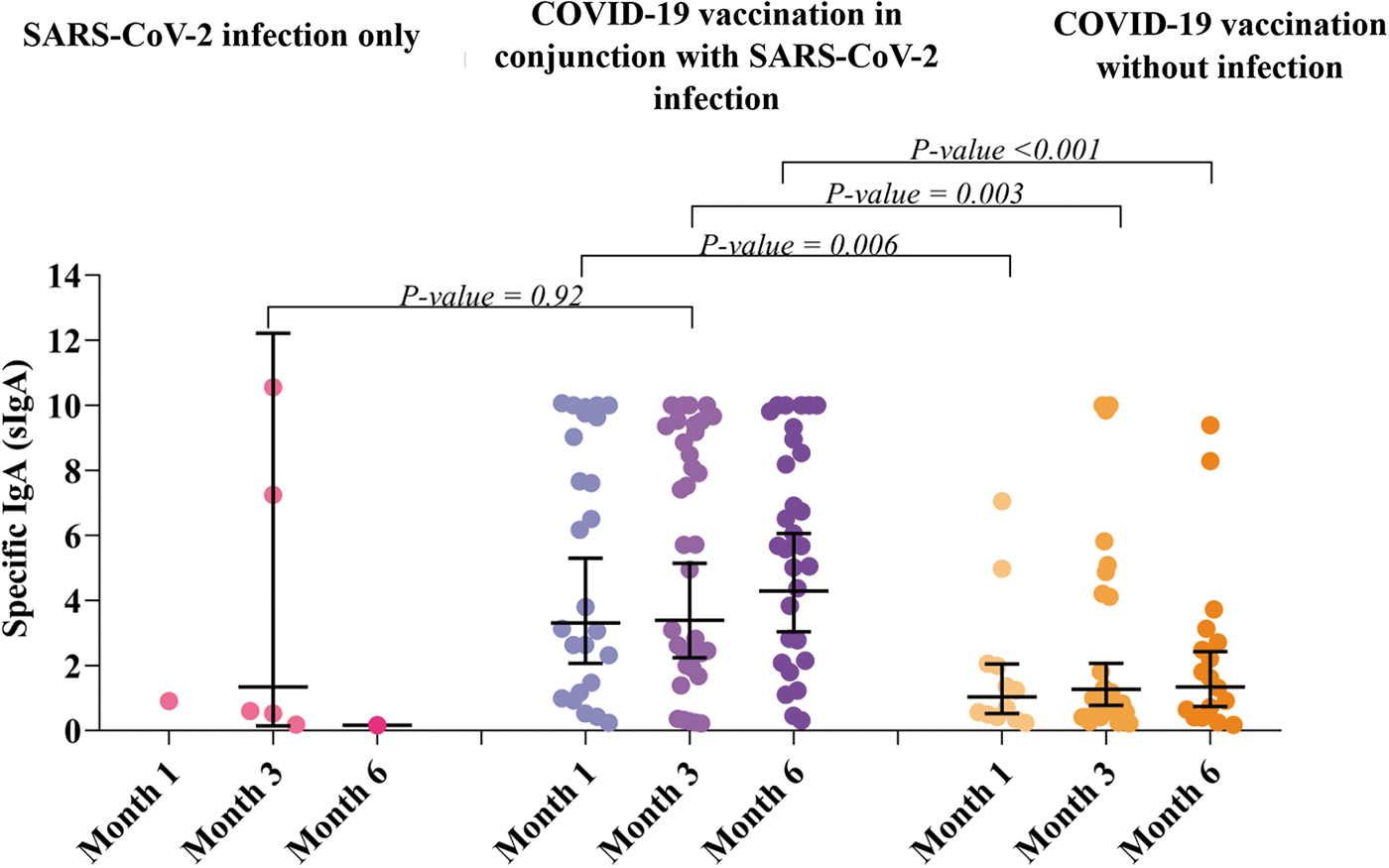
Scatter plot and geometric mean and 95% CI for sIgA against SAR-CoV-2a by period of breast milk collection and the groups. The differences in sIgA were obtained by independent t test. asIgA against SAR-CoV-2 was expressed as a ratio of the extinction of test sample and calibrator. 95% CI, 95% confidence interval; sIgA, specific immunoglobulin A.
Comparison of sIgA Against SARS-CoV-2 in Human Milk Between Participants Who Received COVID-19 Vaccination in Conjunction with SAR-CoV-2 Infection, and COVID-19 Vaccination Without Infection and SARS-CoV-2 Infection Only
Values are presented as GM (95% CI).
sIgA was expressed as a ratio of the extinction of test sample and calibrator.
Since there was only one milk sample, the data were not shown as a GM.
95% CI, 95% confidence interval; GM, geometric mean; sIgA, specific immunoglobulin A.
Subgroup analysis
Comparison of sIgA in breast milk between mothers who had vaccination in conjunction with SARS-Co-V-2 infection and without infection, according to the number of doses
Compared with the COVID-naïve group, mothers who received 2 doses of the COVID-19 vaccination concurrently with the infection exhibited a tendency toward higher sIgA levels at 1, 3, and 6 months. Furthermore, lactating mothers who received 3 doses of the vaccination alongside the infection demonstrated a sIgA level four times higher than that of the COVID-naive group at 1 month. However, no differences of sIgA between the groups were found among the participants receiving
Comparison of sIgA Against SARS-CoV-2 in Human Milk Between COVID-Naïve Lactating Mothers Who Received the COVID-19 Immunization and Those Who Had a History of SARS-CoV-2 Infection in Addition to Receiving the Vaccination
Values are presented as GM (95% CI) and GMR (95% CI) using COVID naïve as the reference group.
sIgA was expressed as a ratio of the extinction of test sample and calibrator.
The differences between the groups were obtained by independent t test.
n = 3.
There was no milk sample of lactation mothers who receive
95% CI, 95% confidence interval; GM, geometric mean; GMR, geometric mean ratio; sIgA, specific immunoglobulin A.
Table 5 compares the sIgA in breast milk of the mothers who received different doses of vaccine. The results revealed no significant differences in sIgA in breast milk between lactating mothers who received 2, 3, and
Comparison of the sIgA Against SARS-CoV-2 in Breast Milk Between Mothers Who Received 2, 3, and >3 Doses of COVID-19 Immunization
Values are presented as GM (95% CI) and GMR (95% CI) using lactating mothers who received the 2 doses of COVID vaccination as the reference.
sIgA was expressed as a ratio of the extinction of test sample and calibrator.
There was no milk sample of lactation mothers who receive
95% CI, 95% confidence interval; GM, geometric mean; GMR, geometric mean ratio; sIgA, specific immunoglobulin A.
Comparison of sIgA between lactating mothers who received various types of COVID immunization and between those who had symptomatic versus asymptomatic COVID infection
There were no differences of sIgA in human milk between lactating mothers who received mRNA, viral-based and mixed type of the COVID vaccines. Also, there was no demonstrable difference of sIgA between lactating mothers who had symptomatic COVID illness and those who were asymptomatic (data not shown).
Discussion
The COVID-19 pandemic led to a disruption of daily-life activities of global population, including lactating mothers. Previous studies reported a decline in the rate of exclusive breastfeeding, possibly due to the concern of viral transmission through breast milk. 10 However, our result shows the lasting presence of sIgA in breast milk among lactating mothers with a history of SARS-CoV-2 infection and/or receiving ∼2 doses of the COVID-19 vaccination. This immunity could be transferred to their infants, protecting them from SARS-CoV-2 infections.
This study found that the sIgA against SAR-CoV-2 in the breast milk of lactating mothers who had a history of COVID-19 illness or received COVID-19 immunization can be detected for up to 6 months after the vaccination and/or infection. Juncker et al. also reported a similar finding: sIgA was present in breast milk after 330 days from PCR-confirmed COVID-19 infection. 5 Likewise, the research conducted in Poland by Szczygioł et al. demonstrated the persistence of sIgA antibodies in the breast milk samples of mothers who had previously been infected with COVID-19, extending up to 229 days postinfection. Notably, the study established a strong positive correlation between the antibody levels found in both serum and breast milk samples. 11
Although the method of sIgA detection remained consistent with our study, there existed a slight disparity in the sIgA levels observed in breast milk. One plausible explanation for this discrepancy could be attributed to genetic variations influencing individual responses to the infection. Moreover, Perl et al. found that sIgA in breast milk could be detected ∼6 weeks after receiving 2 doses of mRNA-based COVID vaccination. 12 These findings supported the recommendation to promote breastfeeding after COVID illness or immunization since sIgA in breast milk may transfer to newborns and protect them from SARS-CoV-2 infections, particularly during the first 6 months of life when COVID vaccines are not available.
Furthermore, the results showed that lactating mothers who had a history of SARS-CoV-2 infection and received ∼2 doses of a COVID vaccine had higher levels of sIgA against SAR-CoV-2 in their breast milk than those who received the vaccination without infection. In accordance with our results, previous studies that explore the level of serum antibody against SARS-CoV-2 also demonstrated that the infection before or after the COVID-19 vaccination dramatically increases the serum-neutralizing antibody response, compared with 2 doses of the vaccine alone.13–15 For example, Bates et al. found that serum immunoglobulin G and A antibodies specific to spike receptor-binding domain protein were significantly elevated among individuals who had a history of COVID-19 illness and received the vaccination. 13
This finding suggests that hybrid immunity, which is the immunity derived from a combination of infection and vaccination, may offer superior protection than either infection- or vaccination-specific immunity alone. There are several possible explanations for this result. First, most individuals with hybrid immunity had been exposed to SARS-CoV-2 antigens more repeatedly than individuals who were only immunized or infected. Moreover, there are differences in the quality of immune responses since the body is exposed to various antigens during infection, whereas mRNA and virus-vectored vaccines only express spike protein antigens. In addition, the infection with the recent variant SARS-CoV-2 and the vaccination may stimulate and expand the body immune response. 16 To the best of our knowledge, this is the first study that explored the effect of hybrid immunity on sIgA in human milk.
The subgroup analysis found no differences in sIgA against SAR-CoV-2 in human milk between lactating mothers who received 2 doses of COVID vaccination and
Similarly, a study from Israel showed that the rate of confirmed infection and the rate of severe illness from SARS-CoV-2 infection were significantly lower in the booster group than in the nonbooster group. However, the study failed to demonstrate the efficacy of the third dose on individuals who had breakthrough infection after receiving a complete primary course of the COVID-19 vaccine. 20 Nevertheless, it is important to note that previous studies have primarily focused on measuring antibody levels in blood, which might not accurately reflect the levels of sIgA against SAR-CoV-2 presented in breast milk.
The WHO's Strategic Advisory Group of Experts on Immunization also recommends an additional booster of COVID-19 vaccine, especially for children ≥6 months, individuals with immunocompromising status or significant comorbidities, pregnant women and health care professionals.
21
Although our study is unable to demonstrate a higher sIgA level in breast milk after receiving
In addition, there is a lack of data regarding the comparison of mortality and morbidity of the breastfed infants whose mothers received 2 doses and
Our study failed to demonstrate the differences in sIgA in breast milk among different types of vaccines. This finding is contrary to previous studies, which have suggested that mRNA-based vaccines provided higher titer of sIgA than viral-based or killed vaccines. For instance, the cohort study from the Netherlands compared human milk antibody response after vaccination with four types of COVID-19 vaccines, including Pfizer-BioNTech (BNT162b2), Moderna (mRNA-1273), Oxford/AstraZeneca (AZD1222), and Johnson & Johnson (Ad26.COV2.S). 22 The result found that sIgA levels peaked on the 15th day after vaccination, with mRNA-1273 showing the highest peak.
After the second dose, all vaccines elicited a stronger response but 2 months later, BNT162b2 and mRNA-1273 groups had significantly elevated IgA levels, with only mRNA-1273 maintaining milk conversion. Similarly, the study by Selma-Royo et al. 23 revealed that the presence and persistence of specific SARS-CoV-2 antibodies in breast milk varied depending on the type of vaccine, suggesting that mRNA-based vaccines showed higher levels of IgG and IgA compared with viral vector vaccines. Our results contradict previous studies, which could potentially be attributed to the limited sample size of the study.
The key strength of our study was as follows: this is the first longitudinal study exploring the effect of hybrid immunity on sIgA against SAR-CoV-2 in human milk in Thailand where vaccination regimen may be different from western countries, as well as the first study to compare breast milk immunity between COVID naïve and those who had a history of SARS-CoV-2 infection in addition to the immunization.
On the contrary, there were some limitations. First, it is important to note that our study did not measure COVID-19–neutralizing antibodies in breast milk. As a result, the presence of sIgA detected in the milk samples from our study does not guarantee protection against SARS-CoV-2 infection for infants. Besides, the limited sample size in our study may have reduced the power to detect differences in the level of immunity between different types or doses of the vaccine. Further studies should be conducted on a larger scale, including the measurement of neutralizing antibodies against SARS-CoV-2 in breast milk.
Conclusion
sIgA against SAR-CoV-2 in breast milk can be detected up to 6 months after the COVID vaccination and/or SARS-CoV-2 infection. This indicates that the presence of sIgA in breast milk could be passed on to breastfed infants, offering protection against SARS-CoV-2 infections for up to 6 months. Discontinuation of breastfeeding among mothers who have had COVID infection or have received vaccination should be discouraged.
Informed Consent Statement
Informed consent was obtained from the legal guardians of the infants involved in this study after the researcher had explained all the study procedures in detail.
Data Availability
Data described in the article, codebook, and analytic code will be made available upon request in a deidentified form.
Footnotes
Acknowledgments
We express our sincere gratitude to Prof. Chitsanu Pancharoen and the dedicated staff of Chula Kids Club for their invaluable assistance and unwavering support. We extend our sincere gratitude to Dr. Sophie Gallier for English editing our article and providing valuable scientific advice. Also, we deeply appreciate Ms. Siriluck Poonkatkij and Ms. Nathawan Khunsri for their administrative assistance and data collection. In addition, we thank Ms. Jiratchaya Sophonphan, The HIV Netherlands Australia Thailand Research Collaboration (HIV-NAT), the Thai Red Cross AIDS Research Centre for the statistical analysis. Finally, we extend our heartfelt gratitude to all the children and their families who willingly participated in this research.
Authors' Contributions
O.S. and S.C. conceived and designed the study. O.S., E.M., P.A., D.M., R.T., and S.K. were involved in data collection. O.S., E.M., S.K., P.S., and N.H. analyzed the data. O.S. and S.C. interpreted the data. O.S., N.H., and S.C. revised the article and all authors jointly approved the final draft.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This study was funded by the Ratchadapiseksompotch Fund, Faculty of Medicine, Chulalongkorn University, grant number RA2565-019, and Dairy Goat Co-operative (N.Z.) Limited and the New Zealand Ministry for Primary Industries (as part of Caprine Innovations NZ Sustainable Food & Fibre Futures Partnership program).