
Abstract
Objective:
To assess the effects of prenatal counseling about the maternal health benefits of lactation on postpartum knowledge, breastfeeding intentions, and infant feeding behaviors.
Materials and Methods:
We conducted a randomized trial with 411 nulliparous U.S.-born women carrying a singleton gestation. Participants were recruited online; after completing a baseline survey that assessed breastfeeding knowledge and intentions, participants were randomized to receive a 10-minute virtual counseling session about the benefits of breastfeeding or attention-control counseling about smoke-free homes. We collected data on breastfeeding knowledge, intentions, and infant feeding behaviors through 12 months postpartum and conducted an intention-to-treat analysis.
Results:
On enrollment, awareness of the maternal health benefits of lactation was similarly low in both study groups. Postpartum, participants who received this prenatal counseling intervention had significantly greater awareness that breastfeeding decreases maternal risk of breast cancer, ovarian cancer, diabetes, heart disease, and rheumatoid arthritis (p < 0.001 for all). On enrollment, intended duration of breastfeeding was similar between groups (10.1 months versus 9.7 months, p = 0.41). At 1-month postpartum, intended duration of breastfeeding had increased from baseline among those who received this counseling (+0.7 months versus −0.7 months among controls, p = 0.004); among intervention participants intended duration of breastfeeding decreased less at 3 (−0.8 versus −1.6, p = 0.18), 6 (−2.0 versus −3.0, p = 0.06), 9 (−2.8 versus −4.2, p = 0.03), and 12 months postpartum (−4.8 versus −6.2, p = 0.09). Rates of exclusive breastfeeding and any breastfeeding were similar between groups.
Conclusion:
Prenatal counseling on the maternal health benefits of lactation increases awareness of these maternal health benefits and extends intended duration of breastfeeding.
ClinicalTrials.gov Identifier:
NCT04601987.
Introduction
Breastfeeding has important long-term health benefits for both mothers and children. 1 As such, the U.S. Centers for Disease Control and Prevention, the American Academy of Pediatrics, the American College of Obstetricians and Gynecologists, and the World Health Organization all recommend that mothers exclusively breastfeed for the first 6 months of their infant's life and continue breastfeeding for at least 1 or 2 years after birth.1–4 However, only 84% of U.S. mothers initiate breastfeeding, 58% breastfeed for 6 months, and only 26% exclusively breastfeed for 6 months. 3 Suboptimal breastfeeding results in an estimated 3,340 preventable U.S. deaths each year, the large majority of which are due to maternal heart disease, breast cancer, and diabetes. 5
Although research has shown for decades that mothers who do not breastfeed are more likely to develop breast cancer, it is estimated that only 28% to 39% of U.S. women are aware that breastfeeding lowers maternal risk of breast cancer.6–9 Breastfeeding has also been shown to lower maternal risk of developing rheumatoid arthritis. 10 Premature discontinuation of lactation also increases maternal risk of type 2 diabetes, hypertension, hyperlipidemia, and cardiovascular disease.11–16 Unfortunately, only 16% of U.S. women are aware that breastfeeding impacts maternal risk of hypertension and only 17% are aware that breastfeeding reduces rates of diabetes. 8 Furthermore, awareness of the maternal health benefits of lactation varies significantly by race/ethnicity and education. 8
Awareness of the benefits of breastfeeding has been associated with prenatal breastfeeding intentions.17,18 Furthermore, in a prior observational study, maternal knowledge that breastfeeding reduces risks of breast cancer was associated with breastfeeding exclusivity and duration. 9 Hypothesizing that mothers with greater awareness of the maternal health benefits of lactation will have stronger and longer intentions to breastfeed and that this may impact duration of breastfeeding, we conducted a trial to evaluate the effects of prenatal counseling about the maternal health benefits of lactation on maternal knowledge, breastfeeding intentions, and infant feeding behaviors. 3
Materials and Methods
We conducted an individual-level randomized attention-controlled trial of a prenatal counseling intervention (Supplementary Appendix SA1) that was delivered using the Zoom videoconferencing platform (Zoom Video Communications, Inc., 2016). We used online advertisements that we paid to display on Facebook and Instagram to recruit nulliparous U.S.-born women carrying a singleton gestation of at least 28 weeks gestation for a study of “prenatal counseling for postpartum health.”
We included English-speaking pregnant individuals currently living in the United States who expected to raise their baby; we excluded those who had previously given birth, those who might be advised against breastfeeding due to HIV infection, or at risk for low milk supply due to a history of breast surgery or in vitro fertilization. From March 2021 to February 2022, we invited qualifying participants to complete a 79-item web-based survey.
Participants were allocated to study groups using a computer-generated random sequence implemented using REDCap software. Each participant then received a 10-minute virtual scripted counseling session (through Zoom) addressing either the maternal health benefits of breastfeeding (written at Flesch-Kincaid Seventh Grade Level) or a 10-minute attention-control counseling session on the benefits of smoke-free homes.
We compensated participants with a $10 gift card for notifying the study team that their baby had been born; participants who experienced a pregnancy loss or still birth were excluded from follow-up. Participants were invited to complete web-based follow-up surveys at 1, 3, 6, 9, and 12 months postpartum by research staff blinded to study group allocation; participants were compensated with a $20 gift card for every survey completed.
We assessed participant sociodemographic characteristics, health-related behaviors, and knowledge of the maternal health benefits of lactation using items adapted from prior work. 17 Using response options of “true,” “false,” and “I don't know,” respondents indicated their opinions regarding whether, “Breastfeeding will lower my risk of breast cancer”; similar questions were posed regarding ovarian cancer, arthritis, diabetes, blood pressure, and heart disease. We dichotomized responses to these questions, comparing correct answers to those who stated they did not know or gave an incorrect response to items assessing the maternal health benefits of lactation. We also asked participants how strongly they agreed or disagreed that “my family members think that I should breastfeed.”
We measured breastfeeding intentions by asking participants how many months they planned to breastfeed or pump milk for their baby at enrollment. On follow-up surveys, we asked until what age in months they planned to continue breastfeeding their baby. We calculated changes in intended duration of breastfeeding from baseline to each follow-up assessment. We measured exclusive breastfeeding by asking, “Has your baby ever been fed or received anything other than your milk to drink?” Those who responded “Yes” were then asked “How old was your baby when s/he was first given something other than your milk? (in weeks)” We measured total duration of breastfeeding in weeks, by asking on all follow-up surveys, “When did you last breastfeed or pump milk for your baby? (mm/dd/yyyy).”
We conducted an intention-to-treat analysis, focused on all participants randomized who reported a live birth, assuming all those lost to follow-up had no breastfeeding knowledge and stopped breastfeeding. We calculated changes in intended duration of breastfeeding by comparing the number of months each participant stated they currently intended to breastfeed for with the number of months that participant reported on enrollment. We then calculated the average change in intended duration of breastfeeding for participants in each group. We used chi-square tests to determine the significance of differences between study groups in categorical variables and t-tests when comparing means.
We used Cox proportional hazard models to examine differences between study groups in duration of exclusive and any breastfeeding controlling for variables associated in prior studies with duration of breastfeeding including sociodemographic characteristics, family support for breastfeeding, hours worked outside the home, obesity, difficulties breastfeeding, and prenatal intentions to breastfeed. Statistical significance was defined as p < 0.05. All statistical analyses were conducted using SAS Enterprise Guide, Version 7.1. Copyright 2017 SAS Institute, Inc., Cary, NC. This study was determined to be exempt (category 2) by the institutional review boards of the University of California at Davis (No. 1623168-1) and San Francisco (No. 21-35243).
Results
After screening 760 individuals, we invited 675 to participate. We randomized and counseled 417 individuals; 411 reported a live birth and were eligible for planned follow-up. Most (94%) completed 12-month follow-up; lost to follow-up did not differ by study group (Fig. 1).
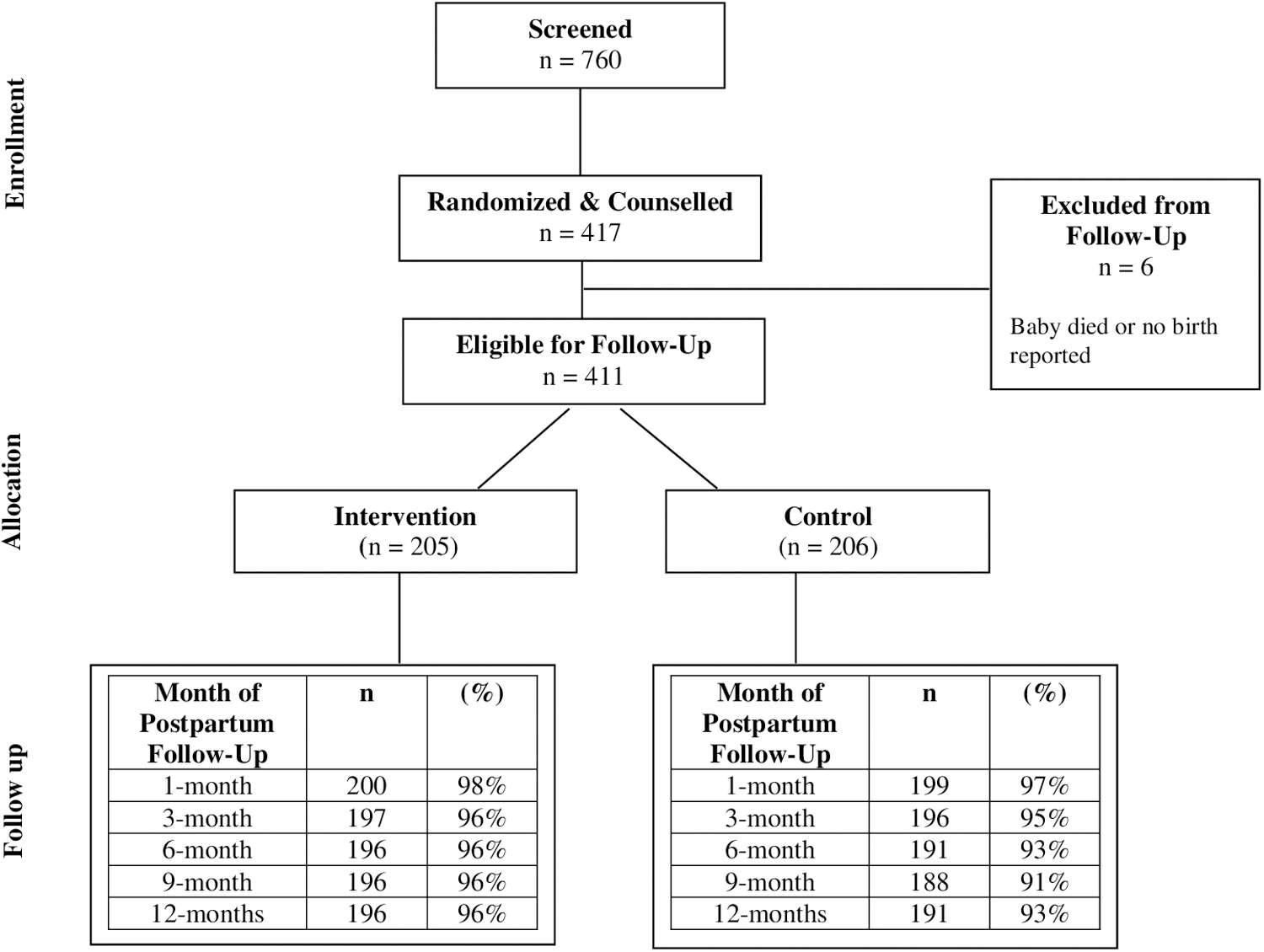
Flow diagram of trial enrollment, allocation, and follow-up through 12 months postpartum.
The sociodemographic, personal health, and family health characteristics of participants in the two study groups were similar (Table 1). The average age of participants was 32 ± 5 years. Participants were racially diverse: 19.7% were African American/Black, 6.1% were Asian, 4.9% were Hispanic or Latina, and 59.6% were White. Most participants (83%) were college educated; 15% were students (Table 1).
Demographic Characteristics of Responding Nulliparous U.S. Pregnant Women (n = 411)
No significant differences between groups; data missing on age for 1, race/ethnicity for 7, geographic region for 20, education for 1, and health insurance for 0 participants, without differences between groups.
Geographic regions defined as follows: northeast (Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island, Vermont, New Jersey, New York, Pennsylvania), midwest (Illinois, Indiana, Michigan, Ohio, and Wisconsin, Iowa, Kansas, Minnesota, Missouri, Nebraska, North Dakota, South Dakota), south (Delaware; Florida; Georgia; Maryland; North Carolina; South Carolina; Virginia; Washington, D.C., West Virginia, Alabama, Kentucky, Mississippi, and Tennessee, Arkansas, Louisiana, Oklahoma, Texas), and west (Arizona, Colorado, Idaho, Montana, Nevada, New Mexico, Utah, and Wyoming, Alaska, California, Hawaii, Oregon, Washington).
Other includes answer responses of “Military Insurance,” “Other,” or “I Don't Know.”
SD, standard deviation.
Before becoming pregnant, participants reported a mean body mass index of 25 ± 5. Relatively few participants had been diagnosed with gestational diabetes (3.7%) or gestational hypertension (0.98%) on enrollment; by 1-month postpartum, 7.6% reported gestational diabetes and 10.7% reported gestational hypertension. Rates of pregnancy complications including cesarean section, need for maternal or neonatal intensive care, readmission, and postpartum anxiety and depression were similar between groups.
On enrollment, participants in both groups had similarly positive attitudes toward breastfeeding (Table 2). Most (92%) participants in both study groups agreed that breastfeeding their baby was important, 96% wanted to breastfeed their baby and 97% indicated it was likely that they would try to breastfeed their baby. However, on enrollment, awareness of the maternal health benefits of breastfeeding was similarly low in both study groups (Table 3).
Attitudes on Enrollment Toward Breastfeeding Among Participating Nulliparous U.S. Pregnant Women
Participants who indicated they strongly agree, agree, or somewhat agree with these statements.
SD, standard deviation.
Effects of Prenatal Counseling on Awareness of the Maternal Health Benefits of Lactation Among Trial Participants
Postpartum awareness of the maternal health benefits of lactation significantly increased among participants who received prenatal counseling about the maternal health benefits of breastfeeding with differences between groups sustained through 12 months postpartum (Table 3). Participants who received this prenatal counseling intervention had significantly greater awareness that breastfeeding delays return of menses and decreases maternal risk of breast cancer, ovarian cancer, diabetes, heart disease, and rheumatoid arthritis to 12 months postpartum.
On enrollment, intended duration of breastfeeding was similar between groups (10.1 months versus 9.7 months, p = 0.41); only 56.4% of participants intended to breastfeed as recommended for at least 12 months, and 8 participants (1.9%) did not intend to breastfeed at all. At 1-month postpartum, intended duration of breastfeeding increased from baseline among those who received this counseling (+0.7 month versus −0.7 month in the control group, p = 0.004).
Over the following months, intended duration of breastfeeding decreased less among participants counseled about the maternal health benefits of lactation than controls (Table 4). Although on enrollment, participants worked similar number of hours each week outside the home (25 versus 27, p = 0.16) at 3 months postpartum, mothers who were counseled about the maternal health benefits of lactation tended to be working fewer hours outside the home each week (10 versus 13, p = 0.07), with no significant differences between groups at 6 (19 versus 20, p = 0.46), 9 (21 versus 23, p = 0.36), or 12 months postpartum (22 versus 25, p = 0.19).
Effects of Prenatal Counseling on the Maternal Health Benefits of Lactation on Change in Intended Duration of Breastfeeding Among Trial Participants
Rates of breastfeeding initiation (90% versus 88%, p = 0.46) and milk expression (89% versus 84%, p = 0.22) were similar at 1 month postpartum. Rates of exclusive breastfeeding at 6 months (26% versus 29%, p = 0.54) and any breastfeeding at 12 months (56% versus 58%, p = 0.69) were similar between groups. In a multivariable model, adjusting for study group, race/ethnicity, college education, family support for breastfeeding, and obesity (Table 5), the variables that significantly predicted discontinuation of breastfeeding by 12 months postpartum were intended duration of breastfeeding on enrollment (hazard ratio [HR] 0.89, 95% confidence interval [CI] 0.85–0.93), any difficulties with breastfeeding (HR 0.42, 95% CI 0.28–0.63), and hours worked outside the home at 12 months (HR 1.01, 95% CI 1.004–1.02).
Effect of Prenatal Counseling on Hazards of Discontinuation of Breastfeeding Before 12 Months Postpartum
Multivariable model includes all variables shown in table; we found no significant associations between breastfeeding at 12 months and participant age, geographic region of residence, health insurance, personal health history, family health history; bold font indicates relationships that are significant with a p < 0.05.
Hours per week reported at 12 months.
Intended duration of breastfeeding measured in months.
HR, hazard ratio; CI, confidence interval.
Discussion
In this randomized trial, we found that brief structured prenatal counseling about the maternal health benefits of lactation resulted in increased awareness of these health benefits through 1 year postpartum. Furthermore, we found that this counseling increased participants' intended duration of lactation. However, we were not able to demonstrate differences in infant feeding behaviors, as rates of breastfeeding were higher at 1 year in both study groups than the 36% of U.S. women who continued breastfeeding at 12 months in 2019. 3
We recognize that knowledge of associated health outcomes must be combined with breastfeeding skills, hospital practices that support breastfeeding, and awareness of how to obtain prompt support when facing breastfeeding challenges, as participants with difficulties breastfeeding had shorter durations of breastfeeding, regardless of their awareness of the health benefits of lactation.
Although awareness of the benefits of lactation in reducing risk of breast cancer was greater in this highly educated sample than previously reported among the larger U.S. population, on enrollment, only half were aware of this potentially modifiable risk factor for breast cancer that afflicts one of eight U.S. women across their life course.9,19 Similarly, although cardiovascular disease is the leading cause of death among American women, few participants were aware that breastfeeding may lower risk of hypertension and improve cardiovascular health in later life.13,15,20
Our findings are supported by prior studies that have also found that U.S. women have limited awareness of the maternal health benefits of lactation.9,17 Prior studies have also found that mothers with greater knowledge of the maternal health benefits of breastfeeding were more likely to express a desire to breastfeed. 17
Our finding that intentions to breastfeed were highly correlated with breastfeeding at 12 months is also supported by prior work, and highlights the importance of addressing the maternal health benefits of lactation when providing prenatal counseling. 21 Notably in this study, although Black women were less likely to breastfeed for 12+ months than non-Hispanic White women, after controlling for breastfeeding intentions and difficulties breastfeeding this was no longer a significant association, highlighting the need for targeted interventions to address racial inequities in breastfeeding.22,23
Limitations of this study include the generalizability of our findings since these participants were more educated (81% of participants were college-educated compared with 39% of U.S. women overall and older than the average first-time mother in the United States [32 years versus 30 years]).24,25 Furthermore, surveys were only distributed in English. Intentions to breastfeed and breastfeeding rates tend to be higher among more educated U.S. women, implying that awareness of the maternal health benefits of lactation is likely even lower among less educated pregnant women in the United States. 26
We did not measure other factors that can influence breastfeeding intentions, such as social or cultural norms, and media representations of breastfeeding. 27 We recognize that not all pregnant individuals identify as women, which was the term used when recruiting participants for this study; further research is needed to understand how to best support informed decisions regarding infant feeding among pregnant individuals who do not identify as women.28,29
In conclusion, prenatal counseling about the maternal health benefits of lactation increases maternal awareness of these benefits and intended duration of breastfeeding through 1 year postpartum. Multiple factors influence the ability to breastfeed as recommended, including paid parental leave, baby-friendly maternity care, prompt lactation consultation, and community and postpartum clinical support 30 ; however, the low levels of awareness of the maternal health benefits of breastfeeding, even among a highly educated sample of pregnant women, indicate that prenatal counseling about the maternal health benefits of lactation is needed to ensure that U.S. families make informed decisions about infant feeding.
Footnotes
Disclaimer
The contents of this publication are solely the responsibility of the authors and do not represent the official views of Health Resources and Services Administration or the National Institutes of Health.
Authors' Contributions
E.B.S. contributed to conceptualization (lead), methodology, investigation, resources, supervision, funding acquisition, and writing—original draft (lead); A.H.-A. was involved in conceptualization, review, and editing (equal); M.F. carried out methodology, software, formal analysis (lead), and data curation; L.R.K. carried out conceptualization and writing—review and editing (equal); C.I. performed the experimental counseling, review, and editing; M.J.C. took charge of conceptualization and writing—review and editing (equal).
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the HRSA R40MC35364 (PI: E.B.S.). A.H.-A. is supported by the National Institutes of Health (NOSI supplement to K23HD101550). A.H.-A. and L.R.K.'s work is supported by the National Center for Advancing Translational Sciences, National Institutes of Health (UL1 TR001860). L.R.K.'s effort was also supported by a Building Interdisciplinary Research Careers in Women's Health award, National Institutes of Health (K12 HD051958, PI: Nancy Lane, MD).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.