
Abstract
Objectives:
To evaluate the efficacy of breastfeeding or feeding of breast milk in reducing blood sampling pain in full-term neonates by comparing with other intervention measures.
Methods:
Related literature was searched from PubMed, EMBASE, Web of Science, and Cochrane Central Register of Controlled Trials (Central). Only randomized controlled trials (RCTs), which reported the effect of breastfeeding or feeding of breast milk on blood sampling pain in full-term neonates, were eligible. The primary outcome was set as pain score on scales, and the secondary outcomes as physiological and behavioral indicators. The risk of bias in included studies was assessed by the Cochrane Collaboration's tool. Data analysis was performed using RevMan 5.4.1.
Main Results:
A total of 17 RCTs were included. Breastfeeding showed a stronger effectiveness in reducing blood sampling pain, compared with nonintervention, placebo, mother's holding, breast milk odor, mother's heartbeat, music therapy, skin-to-skin, and Eutectic Mixture of Local Anesthetics ointment. However, the efficacy of glucose or sucrose (12.5%–30% concentration) seems better than breastfeeding. When compared with other interventions, feeding of breast milk yielded different results. Its effect was only stronger than placebo (sterile water or distilled water), massage, or nonintervention.
Conclusions:
Breastfeeding might be effective for alleviating blood sampling pain in full-term neonates. Its effect is second only to that of glucose/sucrose. The efficacy of feeding of breast milk in reducing blood sampling pain in full-term neonates might not be guaranteed.
Introduction
Pain is defined as an unpleasant emotional and sensory experience associated with actual or potential tissue damage. 1 Studies have demonstrated that neonates can not only feel pain, but also exhibit heightened sensitivity to painful stimuli, as their nervous systems are immature. 2 It is difficult to evaluate the pain in neonates, due to their inability to describe pain verbally. Therefore, it has suggested that the pain in neonates can be indirectly evaluated with behavioral and physiological parameters. 3 These parameters have been compiled into various scales for pain assessment.
Pain increases the risk of neurodevelopmental disorders in neonates. 4 Two methods are commonly taken to reduce the pain in neonates receiving clinical procedures, including pharmacological analgesia and nonpharmacological intervention. The former refers to the use of acetaminophen5,6 and opioid analgesics. The latter involves massage, skin-to-skin, 7 cuddling (mother's holding), oral sucrose water, breastfeeding, 8 non-nutritional sucking, 9 etc. Studies have shown that these measures could significantly alleviate pain. 10 In addition, sucrose is also effective in mitigating procedural pain in neonates. 11
Breastfeeding or feeding of breast milk is safe and accessible. However, normal breast milk contains only 7% lactose, potentially limiting its effectiveness compared with higher concentrations of glucose or sucrose. In contrast, nonpharmacological interventions such as non-nutritive sucking (NNS) or mother's holding may yield similar effects to that of breastfeeding or feeding of breast milk. Therefore, in this review, we meta-analyzed the effectiveness of breastfeeding or feeding of breast milk in reducing pain associated with blood sampling procedures in full-term neonates.
Materials and Methods
Objectives
Our overall objectives were to (1) compare breastfeeding with control interventions (placebo, nonintervention, glucose, sucrose, NNS, mother's holding, music therapy, massage, EMLA ointment, skin-to-skin, breast milk odor, and mother's heartbeat) and (2) compare feeding of breast milk with control interventions (placebo, massage, rocking, nonintervention, glucose, sucrose, NNS, breast milk odor, and mother's holding) in reducing blood sampling pain among neonates. The pain was assessed by physiological (heart rate and oxygen saturation), behavioral parameters (cry duration, proportion of time crying, and duration of the first cry), or scoring scales.
Data sources
We searched related literature from the PubMed (1946–March 2023), EMBASE (1973–March 2023), Web of Science (1928–March 2023), and Cochrane Central Register of Controlled Trials (Central) (The Cochrane Library 2023, Issue 1). Excluded were letters, editorials, reviews, lectures, and commentaries.
Study selection
Included were randomized controlled trials (RCTs) that reported the effects of breastfeeding or feeding of breast milk to alleviate procedural pain in full-term neonates undergoing blood sampling through heel lance or venipuncture.
Data extraction
Data were extracted from the eligible studies independently by two reviewers (C.P.S. and J.T.). Discrepancies were resolved by reaching a consensus or discussion with a third author (W.B.T.). The methodological quality of each included trial was assessed using the Cochrane Handbook, which encompasses seven domains: generation of randomization sequences, allocation concealment, blinding of participants and implementers, blinding of outcome assessment, incomplete outcome data, selective reporting, and other potential biases (Fig. 1).
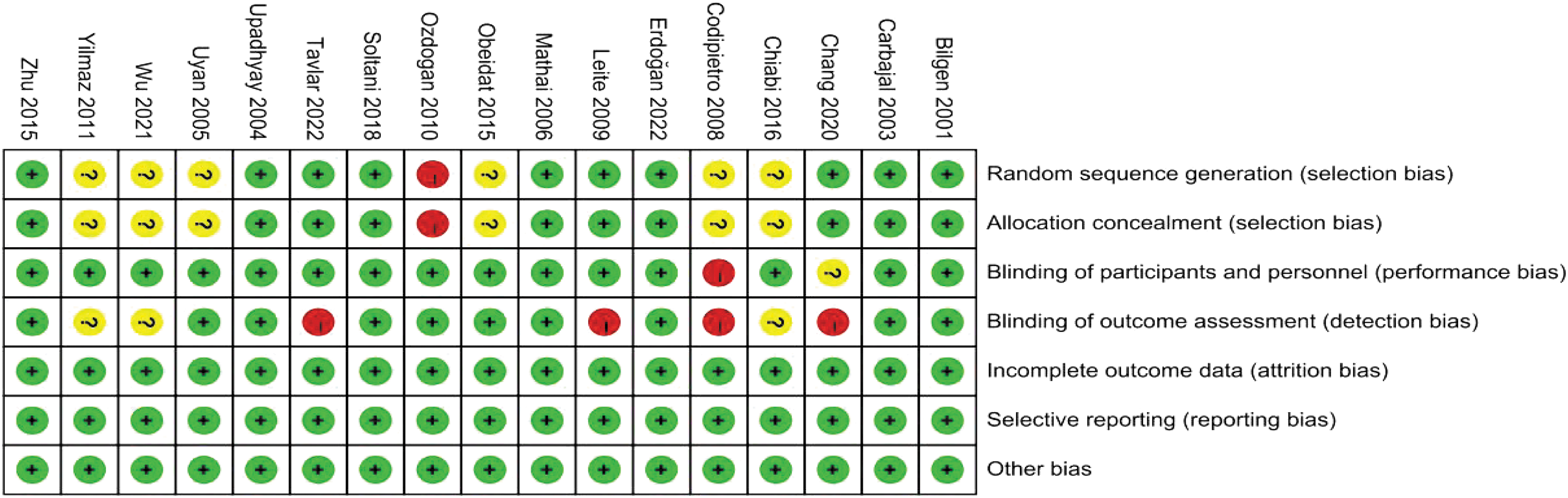
Risk of bias among the 17 included studies. The
Typical effect size was calculated as mean difference (MD) and with a 95% confidence interval (CI) as appropriate. All analyses were conducted using RevMan 5.4.1 software (Cochrane Collaboration). The I2 test for between-study heterogeneity was employed to evaluate the appropriateness of study pooling.
Results
A total of 17 studies were eligible (Fig. 2), including 10 studies about breastfeeding and 8 studies about feeding of breast milk. One of the 17 studies compared breastfeeding with feeding of breast milk. Sampling was performed through heel lance in 14 studies and venipuncture in 3 studies. The data regarding the participants, interventions, and outcomes are given in Table 1 (breastfeeding) and Table 2 (feeding of breast milk).
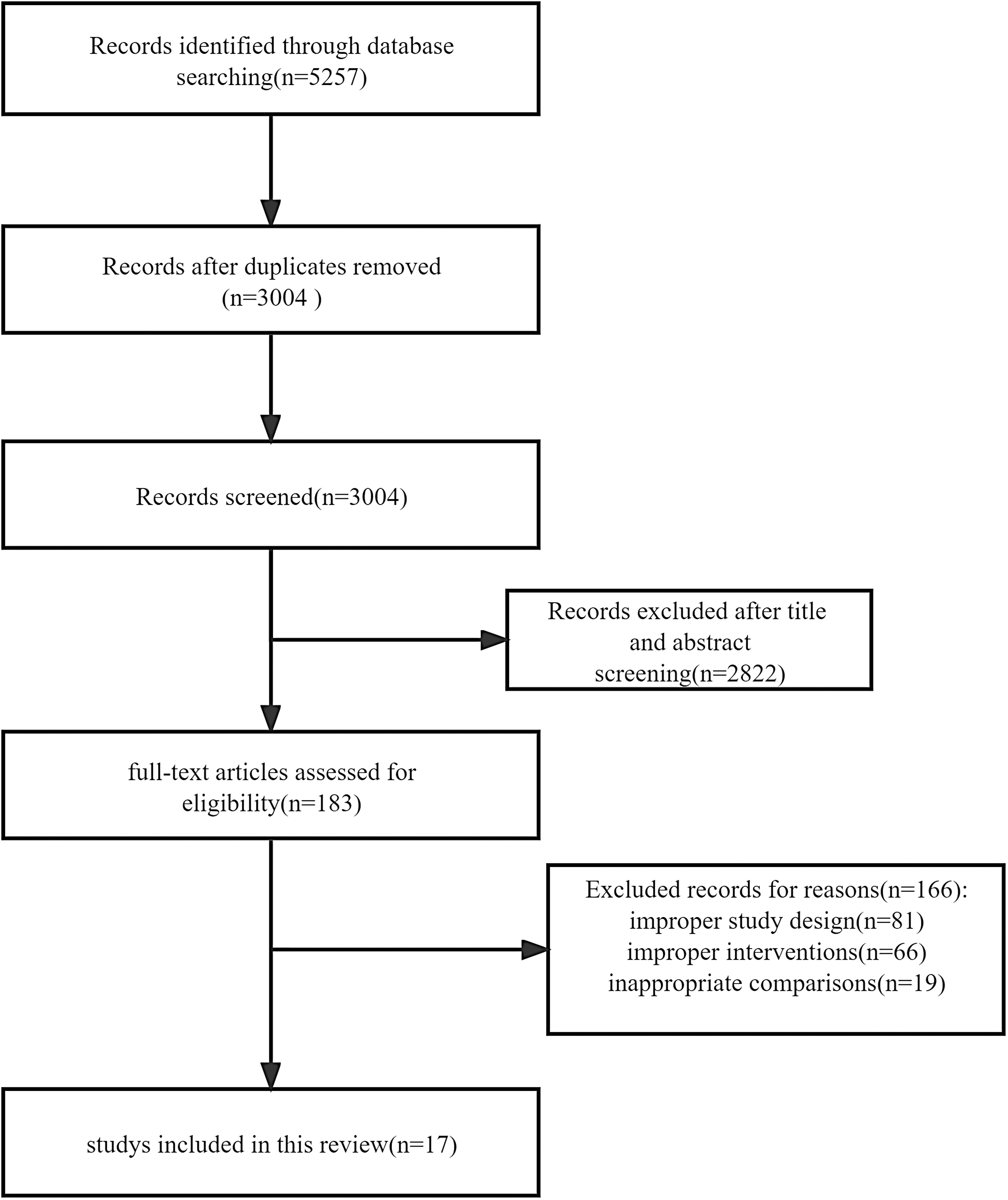
Flow chart of selection of studies.
Characteristics of Randomized Controlled Trials Evaluating the Pain-Reducing Effects of Breastfeeding
RCT, randomized controlled trial; N/A, not applicable; PIPP, premature infant pain profile; N-PASS, neonatal pain, agitation, and sedation scale; IBCS, infant body coding system; DAN, Douleur Aigue Nouveau-ne; NIPS, neonatal infant pain scale; NFCS, neonatal facial coding system.
Characteristics of Randomized Controlled Trials Evaluating the Pain-Reducing Effects of Feeding of Breast Milk
RCT, randomized controlled trial; N/A, not applicable; PIPP, premature infant pain profile; N-PASS, neonatal pain, agitation, and sedation scale; IBCS, infant body coding system; DAN, Douleur Aigue Nouveau-ne; NIPS, neonatal infant pain scale. NFCS, neonatal facial coding system.
Breastfeeding versus control
Pain scales
Douleur Aigue Nouveau-né score scale
The Douleur Aigue Nouveau-né (DAN) scale was used in only one study. 12 The score in the breastfeeding group was statistically significantly lower than those in the sterile water group (MD, −6.31; 95% CI: −8.22 to −4.40) and the mother's holding group (MD, −7.08; 95% CI: −7.92 to −6.24) (Supplementary Fig. S1A, B). The scores were not significantly different between the breastfeeding group and the 30% glucose group (MD, −0.96; 95% CI: −2.05 to 0.13) (Supplementary Fig. S1C).
Infant body coding system scale
The infant body coding system (IBCS) scale was also used in only one study. 13 The IBCS was significantly higher in the breastfeeding group than in the 25% sucrose group (p = 0.001), but showed no significant difference between those in the sterile water group (p = 0.4) and those in the feeding of breast milk group (p = 0.7).
Premature infant pain profile scale
The premature infant pain profile (PIPP) scale was utilized in three studies.12,14,15 The PIPP score was significantly higher in the breastfeeding group than in the sterile water group (MD, −5.89; 95% CI: −7.37 to −4.41) (Supplementary Fig. S2A), the be hugged group (MD, −7.35; 95% CI: −8.86 to −55.84) (Supplementary Fig. S2B), the 25% sucrose group (p < 0.001), and the nonintervention group (p < 0.001), but not significantly different from that in the 30% glucose group (MD, 1.12; 95% CI: −0.42 to 2.66) (Supplementary Fig. S2C).
Neonatal pain, agitation, and sedation scale
One study reported the application of Neonatal Pain, Agitation, and Sedation Scale (N-PASS). 16 The N-PASS score was statistically significantly lower in the breastfeeding group than in the nonintervention group (p < 0.01), but not significantly different from those in the 25% sucrose group (p = 0.24), the skin-to-skin group (p = 0.1), and the NNS group (p = 0.74).
Neonatal infant pain score
The pain was evaluated with neonatal infant pain score (NIPS) in three studies.17–19 The NIPS during sampling procedures was significantly lower in the breastfeeding group than in the 30% glucose group (p < 0.001), but there was no significant between-group difference at 2 minutes after the procedure (p = 0.87). 18 The NIPSs were significantly higher in the nonintervention and music therapy groups than in the breastfeeding group during and at 1 minute after the procedure (p < 0.001), but there was no significant between-group difference at 5 minutes after the procedure (p = 0.065). 17 The NIPS score in the breastfeeding group was significantly lower than that in the skin-to-skin group, the EMLA ointment group, or in the 25% sucrose group (p < 0.001). 19
Neonatal facial coding system
One study reported the analysis of Neonatal Facial Coding System (NFCS) scores. 20 The score was statistically significantly lower in the breastfeeding group than in the mother's holding group (p < 0.001).
ALPS-Neo pain score
One study reported the analysis of ALPS-Neo scores. 21 The ALPS-Neo pain score was significantly lower in the breastfeeding group than in the breast milk odor or mother's heartbeat group during or after the sampling procedure (p < 0.001).
Physiological parameters
Heart rate (beats per minute)
In two studies,13,14 heart rate was adopted to evaluate the pain during or after the heel lance. The heart rate increased in every group at 1 minute after the procedure, more significantly in the breastfeeding group than in the 25% sucrose group (MD, 19.9; 95% CI: 8.75–31.05) (Supplementary Fig. S3A), but there was no significant difference between the breastfeeding and sterile water groups (MD, 5.31; 95% CI: −11 to 21.62) 13 (Supplementary Fig. S3B). Codipietro et al. reported that at 30 seconds after the procedure, the increase of heart rate was significantly higher in the breastfeeding group than in the 25% sucrose group (p = 0.005).
Oxygen saturation
One study reported the changes in oxygen saturation during heel lance. 14 Oxygen saturation decreased in both the breastfeeding group and the 25% sucrose group, less significantly in the former (p = 0.001).
Heart rate recovery time
One study 13 reported that after heel lance, the heart rate recovery time (in seconds) was significantly longer in the breastfeeding group than in the 25% sucrose group (p = 0.02). But there was no significant difference between the breastfeeding and the placebo groups (sterile water) (p = 0.44).
Cry variables
Percentage of crying time
Codipietro et al. reported that during heel lance, the percentage of crying time decreased significantly in the breastfeeding group, compared with that in the oral 25% sucrose group (p < 0.001). 14
Crying duration
Three studies13,16,21 reported no statistically significant difference in the crying duration (in seconds) (MD, 42.31; 95% CI −3.54 to 88.16) between the breastfeeding group and the 25% sucrose group13,16 (Supplementary Fig. S4A), but the crying duration was reduced in the breastfeeding group, compared with that in the sterile water group (p < 0.008). 13 The breastfeeding group demonstrated a significant reduction in the crying duration, compared with nonintervention group (MD, −203.4; 95% CI: −279.88 to −126.92) 16 (Supplementary Fig. S4B).
Meanwhile, there was no significant difference in the crying duration between the breastfeeding group and the NNS group (MD, 7.8; 95% CI: −63.74 to 79.34) or the skin-to-skin group (MD, −9.00; 95% CI: −71.82 to 53.82) 16 (Supplementary Fig. S4C, D). Crying duration was reduced in the breastfeeding group during or after the heel lance, compared with that in the breast milk odor group or mother's heartbeat group (p < 0.001). 21
First cry duration
Two studies14,17 reported the duration (in seconds) of the first cry. Codipietro et al. reported that the first cry duration was reduced in the breastfeeding group, compared with that in the 25% sucrose group (p < 0.001).14,17 Zhu et al. reported a significantly shorter first cry in the breastfeeding group than in the nonintervention group and the music therapy group (p < 0.001).14,17
Feeding of breast milk versus control
Pain scales
IBCS score
One study 13 reported the analysis of IBCS score. The IBCS score was significantly higher in the feeding of breast milk group than in the 25% sucrose group (p = 0.001), but not significantly different from that in the sterile water group (p = 0.24).
Neonatal facial coding system
The pain was evaluated with NFCS in three studies.22–24 No significant difference was found between the feeding of breast milk group and the placebo group immediately (MD, −0.45; 95% CI: −1.00 to 0.11)22,23 or 1 minute (MD, −0.72; 95% CI: −1.67 to 0.24)22–24 after the sampling procedure, but there was a significant reduction in the NFCS in the feeding of breast milk group when compared with the placebo group at 2 minutes (MD, −0.80; 95% CI: −1.16 to −0.43)23,24 or 3 minutes (MD, −1.20; 95% CI: −1.58 to −0.83)22–24 after the procedure (Fig. 3).
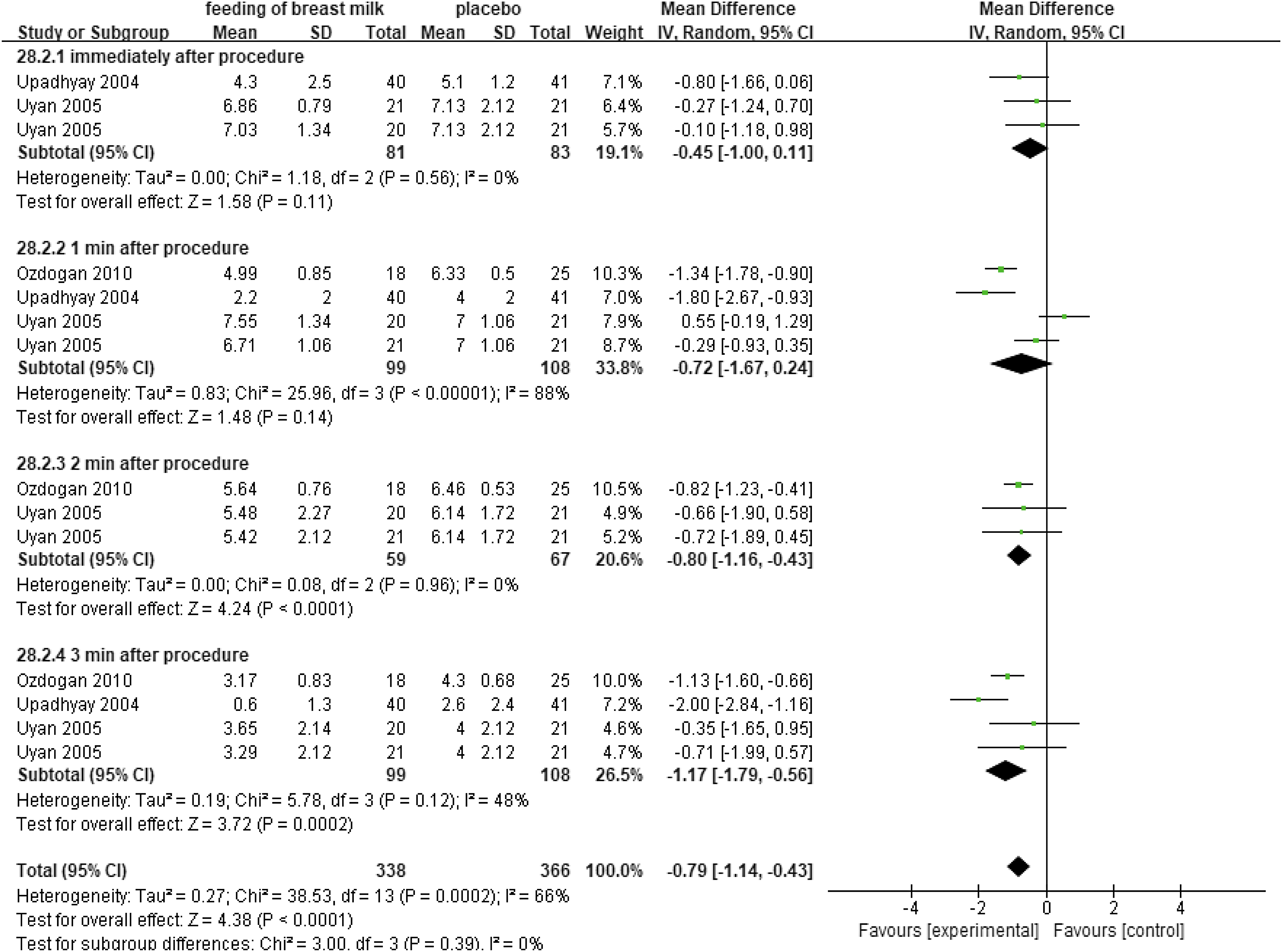
Subgroup analysis: feeding of breast milk versus control. Comparison of feeding of breast milk group and placebo group immediately, 1 minute, 2 minutes, and 3 minutes after the blood sampling by using NFCS. NFCS, neonatal facial coding system.
Ozdogan et al. reported that the NFCS scores were significantly higher in the feeding of breast milk group at 1 minute (MD, 0.94; 95% CI: 0.50 to 1.38) (Supplementary Fig. S5 A), 2 minutes (MD, 0.92; 95% CI: 0.49 to 1.35) (Supplementary Fig. S5B), and 3 minutes (MD, 1.43; 95% CI: 0.98–1.88) (Supplementary Fig. S5C) after the procedure, when compared with those in the 12.5% sucrose group. 24
DAN score
One study reported the DAN scores at 2 minutes. 25 The DAN score dropped significantly in the feeding of breast milk group, compared with the distilled water group (MD, −1.10; 95% CI: −1.65 to −0.55) (Supplementary Fig. S6A) and the massage group (MD, −0.50; 95% CI: −0.91 to −0.09) (Supplementary Fig. S6B). There was no significant difference between the feeding of breast milk group and the 20% sucrose group (MD, 0.10; 95% CI: −0.30 to 0.50) (Supplementary Fig. S6C). The DAN score was significantly higher in the feeding of breast milk group than in the NNS group (MD, 0.80; 95% CI: 0.40–1.20) (Supplementary Fig. S6D), and in the rocking group (MD, 1.10; 95% CI: 0.65–1.55) (Supplementary Fig. S6E).
Neonatal infant pain score
The pain was measured by NIPS in two studies.26,27 No significant difference was found between the feeding of breast milk group and the 20% sucrose group during the procedure (p > 0.05), but the NIPS was significantly higher in the feeding of breast milk group after the procedure (p < 0.05). No statistical difference was found between the feeding of breast milk group and the nonintervention group (MD, −1.23; 95% CI: −3.53 to 1.07) (Supplementary Fig. S7), or the NNS (pacifier) group during the procedure (p > 0.05).
Neonatal pain, agitation, and sedation scale
Only one study reported the assessment with this index. 28 Erdogan et al. reported a statistically significant reduction in the N-PASS score in the feeding of breast milk group, compared with the nonintervention group and the breast milk odor group during or after the procedure (p < 0.001).
Physiological parameters
Heart rate (beats per minute)
Heart rate was adopted to evaluate the pain in two studies.13,26 Bilgen et al. reported a significantly higher increase in the heart rate in the feeding of breast milk group than in the 25% sucrose group (MD, 13.95; 95% CI: 4.06–22.78) (Supplementary Fig. S8A). But there was no significant difference between the feeding of breast milk group and the sterile water group during (MD, −3.15; 95% CI: −10.91 to 4.61) (Supplementary Fig. S8B) or 1 minute after the procedure (MD, −1.14; 95% CI: −14.70 to 12.42) (Supplementary Fig. S8C). 13 Yilmaz et al. also showed no difference between the feeding of breast milk group, the 20% sucrose group, the NNS group, or the nonintervention group (p > 0.05). 26
Heart rate recovery time
Two studies13,22 reported the analysis of this index. The heart rate recovery time (in seconds) was significantly higher in the feeding of breast milk group, compared with the 25% sucrose (p = 0.007), but no significant difference was found between the feeding of breast milk group and the sterile water group (MD, −46.93; 95% CI: −122.84 to 28.97) (Supplementary Fig. S9).
Cry variables
Crying duration
Seven studies13,22–27 reported the duration (in seconds) of crying. The data from five studies revealed a statistically significant reduction in the crying duration in the feeding of breast milk, compared with the one dose of the placebo group (MD, −10.06; 95% CI: −19.24 to −0.88)13,22–25 (Fig. 4A). When comparing feeding of breast milk with two doses of placebo, no statistical difference was identified (MD, −2.80; 95% CI: −19.22 to 13.62) 24 (Supplementary Fig. S10A).
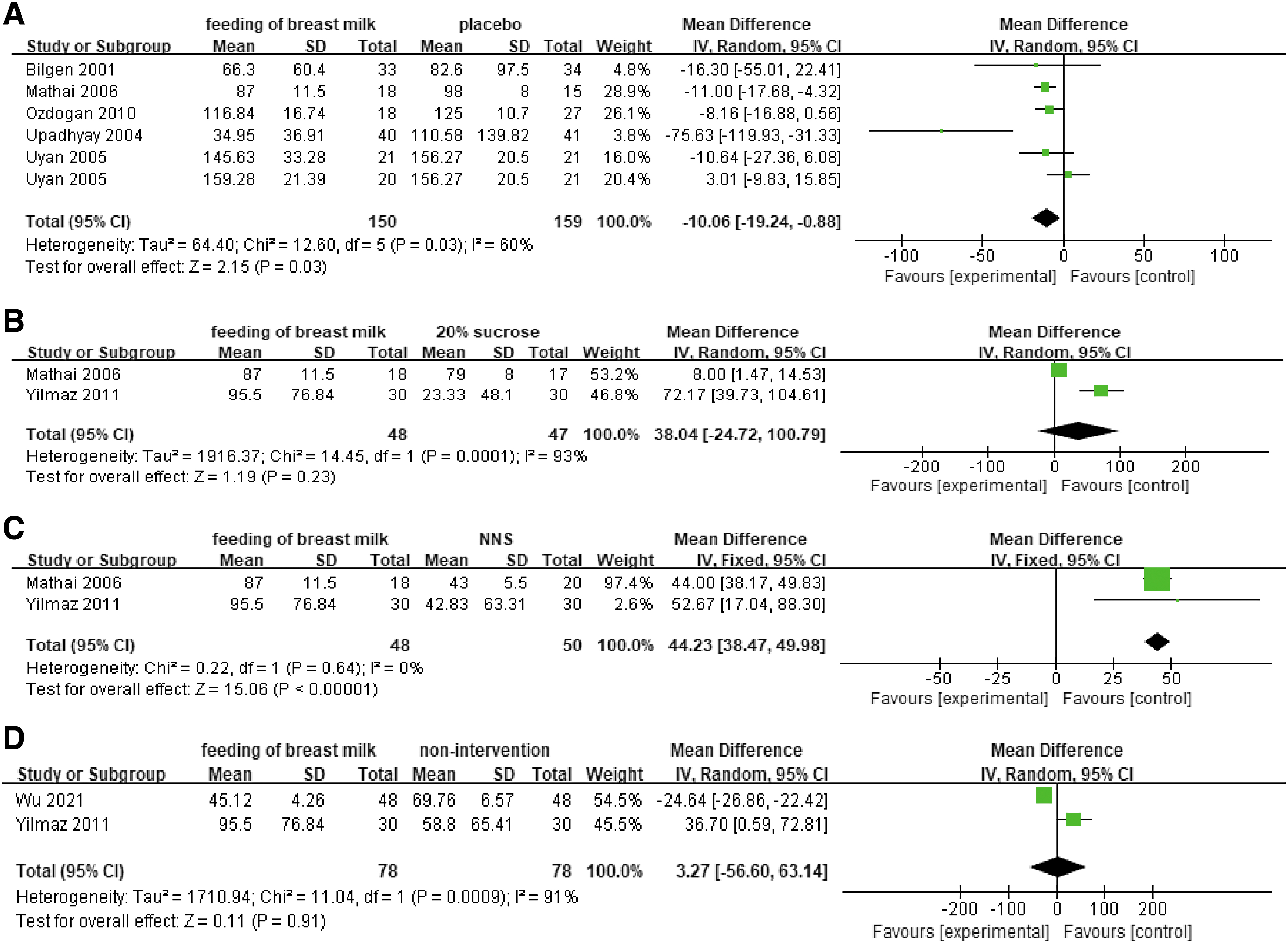
Effect of feeding of breast milk versus control on crying duration (in seconds). Comparison between feeding of breast milk group and placebo group
Bilgen et al. observed a significant increase in the crying duration between the feeding of breast milk and the 25% sucrose group (p = 0.01), 12 but not between the feeding of breast milk group and the 20% sucrose group (MD, 38.04; 95% CI: −24.72 to 100.79)25,26 (Fig. 4B). Mathai et al. reported a reduction in crying duration in the feeding of breast milk group, compared with the massage group (MD, −9.00; 95% CI: −16.97 to −1.03) 25 (Supplementary Fig. S10B).
The crying duration increased in the feeding of breast milk group, compared with the NNS group (MD, 44.23; 95% CI: 38.47–49.98) (Fig. 4C),25,26 the rocking group 25 (MD, 31.00; 95% CI: 24.47–37.53) (Supplementary Fig. S10C), the single-dose 12.5% sucrose group (MD, 34.84; 95% CI: 25.30–44 38) (Supplementary Fig. S10D), 24 and the two-dose 12.5% sucrose group (MD, 30.80; 95% CI: 16.72–44.88) 25 (Supplementary Fig. S10E).
There was no difference in the crying duration between the single-dose feeding of breast milk group and the two-dose feeding of breast milk group (MD, 2.77; 95% CI: −13.30 to 18.84) 24 (Supplementary Fig. S10 F). No statistical difference was identified between the feeding of breast milk and the nonintervention group (MD, 3.27; 95% CI: −56.60 to 63.14)26,27 (Fig. 4D).
First cry duration
Only two studies23,25 assessed the duration (in seconds) of the first cry. No significant difference was found between the feeding of breast milk group and the placebo group (MD, 0.95; 95% CI: −4.85 to 6.74)23,25 (Supplementary Fig. S11A), the massage group (MD, −6.00; 95% CI: −12.34 to 0.34) (Supplementary Fig. S11B), or the rocking group (MD, −0.43; 95% CI: −0.24 to 1.10) 25 (Supplementary Fig. S11C). The first cry duration was significantly higher in the feeding of breast milk group than in the 20% sucrose group (MD, 6.00; 95% CI: 2.50 to 9.50) (Supplementary Fig. S11D) or the NNS (pacifier) group (MD, 4.00; 95% CI: 0.18–7.82) 25 (Supplementary Fig. S11E).
Discussion
All studies included in this review evaluated the effects of breastfeeding or feeding of breast milk on the pain during a single blood sampling. Breastfeeding was associated with a reduction in pain scores (DAN, PIPP, N-PASS, NIPS, NFCS, and ALPS-Neo), the crying duration, and the first cry duration, when compared with nonintervention, placebo, mother's holding, breast milk odor, mother's heartbeat, music therapy, skin-to-skin, and EMLA ointment. Breastfeeding showed no advantages in reducing four types of pain scores (DAN, IBCS, N-PASS, and PIPP), heart rate change, and heart rate recovery time, when compared with higher concentrations of glucose/sucrose. However, it was more effective in reducing NIPS scores, oxygen saturation fluctuation, percentage of crying time, and duration of the first cry.
Based on the above results, we recommend that breastfeeding, or its alternatives (such as sucrose or glucose), should be provided to neonates undergoing a single blood sampling for relieving pain. Feeding of breast milk produced different results, suggesting that its efficacy in relieving pain is not well established. Its outcomes were only superior to those of the placebo (sterile water or distilled water), massage, or nonintervention. Nevertheless, in blood sampling, breastfeeding or feeding of breast milk could encourage mothers to breastfeed their babies, promote their bonding, and relieve the psychological burden on mothers.
Our recommendations may be applicable to a large population, because most full-term babies need venipuncture or heel puncture in the first few days of life. In many countries, all newborns undergo heel lance for metabolic screening in the first week of life. Even in countries where metabolic screening is not yet compulsory, healthy full-term newborns often need heel lance or venipuncture for other simple testings. 29 Therefore, our findings in this study have provided reliable advice for pain relief in children who require heel lance or venipuncture.
The eligible studies in this review only included healthy full-term neonates. However, a different population of infants, such as premature infants and sick full-term newborns, has to undergo repeated blood samplings during hospitalization.30,31 The optimal analgesics for them have not yet been found. One trial 32 reported that preterm infants (<31 weeks gestational age), who received repeated sucrose administration before painful procedures, exhibited poorer neurological development, compared with those receiving fewer sucrose doses. Therefore, breastfeeding or feeding of breast milk, due to their safety, may be introduced to replace sucrose.
Several limitations are evident in this review. First, there was heterogeneity in the tools used to evaluate pain across studies. This issue has also been encountered in a previous review on using sucrose to reduce procedural pain in neonates. 11 Various physiological, behavioral parameters, and pain scales were randomly chosen to assess pain in previous studies. A unified and reliable tool should be designed in the future. Second, we only analyzed the effects of breastfeeding or feeding of breast milk on the pain from a single blood sampling.
However, many preterm or sick full-term neonates experience repeated blood sampling during hospitalization. Therefore, future studies should focus on the effects of breastfeeding or feeding of breast milk on recurrent procedural pain. Moreover, it is imperative to clarify the long-term impact of repeated breastfeeding or feeding of breast milk on the acceptance of infants, especially preterm neonates, toward breastfeeding at a later stage. Only one study, 12 which assessed the maternal perception of sucking during breastfeeding after a single blood sampling, reported no significant changes in this acceptance.
However, the impact of repeated exposure remains to be further explored. Finally, the included studies demonstrated a marked heterogeneity in the duration and quantity of prior exposure to breastfeeding or feeding of breast milk, as well as control interventions.
Conclusion
Breastfeeding is recommended for alleviating procedural pain in full-term neonates undergoing a single blood sampling. Its effect is second only to that of glucose/sucrose (12.5%–30% concentration). Feeding of breast milk might not be as effective as breastfeeding or glucose/sucrose in reducing blood sampling pain in full-term neonates. The safety or effectiveness of breastfeeding or feeding of breast milk on the pain from repeated blood sampling remains uncertain, necessitating the conduction of better designed RCTs, particularly those based on preterm neonates.
Authors' Contribution
W.B.T., J.T., and C.P.S. contributed to the conception and design. C.P.S. and J.T. contributed to data acquisition or analysis and interpretation of data. C.P.S. and J.T. were involved in drafting the article. W.B.T. and W.L. revised the article critically for important intellectual content. All authors have given final approval for the version to be published.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.