
Abstract
Background and Objective:
Melatonin in breast milk exhibits a 24-hour circadian rhythm, present in nighttime breast milk but nearly undetectable in daytime breast milk. Shift work can disrupt the circadian timing of individuals, evident in changes in melatonin in saliva and urine samples. However, it is unknown whether these changes are also reflected in breast milk from a shift working mother. The aim of this study was to investigate whether maternal circadian rhythm disturbance from shift work impacts the melatonin concentration in breast milk.
Materials and Methods:
Breast milk and saliva samples were collected from 11 shift working mothers at four timepoints across five consecutive days. This included during their day shift or nonworkdays to act as a control, night shift, subsequent night shifts and postnight shift. Where possible, pre- and postfeed collections were also undertaken. Samples were grouped into four-time intervals: 12–6:30 am, 7–11:30 am, 12–6:30 pm, 7–11:30 pm, and melatonin levels (picogram per milliliter) in the breast milk and saliva samples were analyzed.
Results:
There was a significant decrease in breast milk melatonin (p = 0.026) at the 12–6:30 am time interval on subsequent night shifts, compared with control days. However, there was no overall time and shift type interaction effect (p = 0.70). In addition, no observed difference in melatonin levels was found in saliva samples, or when comparing pre- and postfeed breast milk. Breast milk melatonin however was found to be significantly higher compared with saliva (p > 0.001), at all but one time interval.
Conclusion:
The findings suggest that there is a potential effect of maternal circadian rhythm disruption from shift work on breast milk melatonin levels. This is an important step in exploring the role of maternal circadian timing and the effect on breast milk composition. Expansion of this research and exploration of other circadian rhythm misalignment sleep disorders on breast milk is highly recommended.
Introduction
An individual's typical melatonin production exhibits a 24-hour sleep–wake cycle, starting at around 9:00 pm and peaking at around 2–3 am in the morning, then returning to almost undetectable levels during the day.1,2 Circadian timing is important for the regulation of a person's bodily functions, including sleep and feeding patterns, core body temperature, hormone production, regulation of glucose and insulin levels, cell regeneration, and many other biological activities.3,4 Circadian misalignment can result in significant physical and mental health consequences including reduced quantity and quality of sleep, irritability, cognitive impairment, increased risk of diabetes, hypertension, high cholesterol, and cardiovascular disease.5,6
Infants are not born with a circadian sleep–wake cycle fully established, rather it is developed in early infancy.7,8 Research shows that melatonin in breast milk, of healthy nonshift working mothers, exhibits a similar circadian rhythm seen in individuals, with melatonin barely detectable in daytime breast milk but present in evening breast milk.9–11 The role of melatonin in breast milk, therefore, may be to support an infant's internal body clock, the timekeeper that allows babies to distinguish day from night.10,12,13
At least 20–30% of parents report that their infant or child has difficulty sleeping, such as difficulty falling asleep at the start of the night, frequent night waking, early morning waking, or a combination of these sometime in the first year.14–16 These sleep difficulties can persist into adolescence and adulthood, 17 with research also showing that sleep problems that arise in infancy persist for 21% of children through to 36 months of age.18,19 In addition, infants with poor sleep patterns (shorter sleep duration, onset, and awakenings) are at increased risk of obesity, 20 early onset or risk of type 2 diabetes later in life, poor mental health,21,22 behavioral problems, and impaired cognitive development outcomes including autism spectrum disorders.23,24
Shift work can cause a misalignment of a person's circadian rhythm. An indicator of circadian dysregulation is circulating melatonin levels.25–27 Melatonin is easily quantifiable in urine, blood, and saliva and is reliable as a biomarker of circadian dysregulation.28–30 Previous research shows that working night shift can cause melatonin to peak earlier or later, compared with day-only workers.5,27 At present, however, it is not known if disturbances of maternal circadian timing, such as from shift work, jet lag, or sleep disorders, impact the circadian rhythmicity of breast milk composition. 31 If hormone signals in breast milk do indeed help to calibrate infant circadian biology, infants who drink breast milk that has hormones out of sync, may experience difficulties with sleep, digestion, and development, potentially having a dramatic effect on an infant's growth and long-term health.32–34 The impact of maternal circadian disruption on breast milk hormones needs urgent attention. Thus, the objective of this study was to investigate if maternal circadian rhythm disturbance from shift work impacts the melatonin concentration in breast milk.
Materials and Methods
Study design
The study was a prospective repeated-measures design, approved by the Austin Health Human Research Ethics Committee (HREC/81999/Austin-2022). The study design involved collecting saliva and breast milk samples at periodic intervals (four times per day, 2 day/2 night) across a consecutive 5-day period. Saliva samples were used to measure maternal circadian timing. Samples were collected between September and December 2022.
Participants
Eligible participants were older than 18 years of age, currently breastfeeding, had returned to working shift work including night shifts and had capability to express 5–10 mL of breast milk within each of four time periods (12–6:30 am, 7–11 am, 12–6:30 pm, 7 pm–11:30 am) for 5 consecutive days. Participants were excluded if they were unable to express breast milk within the time periods, were taking medication or supplements to help with feeding (such as domperidone/motilium) or to aid sleep (such as melatonin or herbal tablets), and who had been diagnosed with a sleep disorder or postnatal depression. Eleven mothers participated in the study.
Measurements
Baseline questionnaire
A paper-based questionnaire was sent to participants who consented to participate. This questionnaire collected the following information: infant age, body mass index (BMI), and how long the participant had been back at shift work.
Saliva and breast milk sample collection kits
Collection of samples was performed by the participants, in their own home and/or workplace. Based on previous research indicating the peaks and troughs of melatonin in breast milk,10,31 the protocol was to collect two daytime and two nighttime samples to capture this fluctuation. Participants collected samples over a 5-day period beginning with day shifts or nonworkdays, to act as a control, followed by night shifts. If mothers were not feeding their child at the time of sample collection, it was recommended that they still collect a sample at the designated time. At each time point, mothers were asked to collect a 5–10 mL breast milk sample “prefeed” and “postfeed” where possible. That is, at the start and end of the breast milk feed or expression to investigate if melatonin concentrations vary throughout the feeding.
The timing of the samples was individualized to, where possible, align with the mother's normal feeding routine. For example, if a mother's last feed was at 9 pm at night, then on each of the five study nights that sample would be consistently collected around 9 pm. Participants stored their samples in their freezer, where they normally would store their breast milk (at home or at work). Participants labeled each sample with the date, time of collection, and if it was a pre- or postfeed sample.
Sleep diary and sample collection log
Participants were asked to keep a daily log of when they collected each breast milk and saliva sample as well as when they went to sleep, woke up, and worked.
Procedure
Participants were recruited via social media where expressions of interest were sought from mothers who had returned to work and were still breastfeeding. A research team member contacted interested individuals to detail the study and determine eligibility, and the Participant Information and Consent Form (PICF) was provided. Informed signed consent was freely given by all participants. Once consented, participants provided details of their current shift work roster to determine five consecutive days that included both day shift or nonworkdays, followed by at least one night shift, for sample collection. A sample collection kit was posted to the participant, which included all equipment and instructions needed for saliva and breast milk collection, the sample collection log to write collection date and times, a sleep diary and questionnaire administered at baseline.
After the sample collection kit was received by the participant, a virtual meeting was scheduled with a member of the research team to ensure the participant understood the sample collection instructions and equipment and to answer any questions before commencement.
At the completion of the 5 days, the samples were collected by a member of the research team or by a courier, on dry ice, and stored at a central location. All samples were later couriered via dry ice and analyzed by the Adelaide Research Assay Facility using double antibody radioimmunoassay, using standards and reagents supplied by Novolytix (RKDSM-2, Novolytix GmbH, Witterswil, Switzerland). This assay was based on the Kennaway G280 anti-melatonin antibody 28 and uses [125I] 2-iodomelatonin as the radioligand. Saliva samples were assayed according to the saliva melatonin radioimmunoassay protocol provided by Novolytix. Before assaying, breast milk samples were centrifuged (4,000 g, 4°C, 15 minutes) to separate the fatty from the nonfatty milk layer. An aliquot from the milk layer was transferred to a separate tube and used for subsequent assaying, which was performed as per the protocol provided by Novolytix.
For both saliva and milk samples, the lower limit of quantitation of the assay was 4.3 pM. Saliva and breast milk samples were assayed in duplicate. The intra-assay coefficient of variation of the assays was determined to be 8.8%. The interassay coefficient of variation at the low concentration quality control (17.9 pM) was 10.9%, and the interassay coefficient of variation at the high concentration quality control (98.7 pM) was 7.2%. Participants were compensated for their time via a $100 AUD gift voucher.
Statistical analysis
Melatonin levels (picogram per milliliter) in breast milk and saliva samples were compared across time points and shift types. Samples for both breast milk and saliva were grouped based on shift type; control (days or nonworkdays), first night shift, subsequent night shift (two or more in a row), and postnight shift. The data were then grouped into the four time intervals, based on previous studies to capture the peaks and troughs of melatonin timing in breast milk35,36: 12–6:30 am, 7–11:30 am, 12–6:30 pm, and 7–11:30 pm. One-way analysis of variance (ANOV1A) was used to explore breast milk melatonin levels across each shift type, for each time interval. A general linear model was used to determine the differences in melatonin in the breast milk across each time interval; with time as the within-subjects' factor and shift type being the between-subjects' factor.
Independent t-tests were conducted to compare saliva versus breast milk melatonin at each time interval, as well as paired t-tests to compare pre- and postfeed breast milk melatonin against each other. Statistical analyses were performed using IBM SPSS Statistics (version. 29) for Windows (SPSS Inc., Chicago, IL). A value of p < 0.05 was considered statistically significant.
Results
On average participants had returned to work, doing shift work for 4.6 months, and had an infant with a mean age of 13.5 ± 1.4 months.
Breast milk melatonin levels
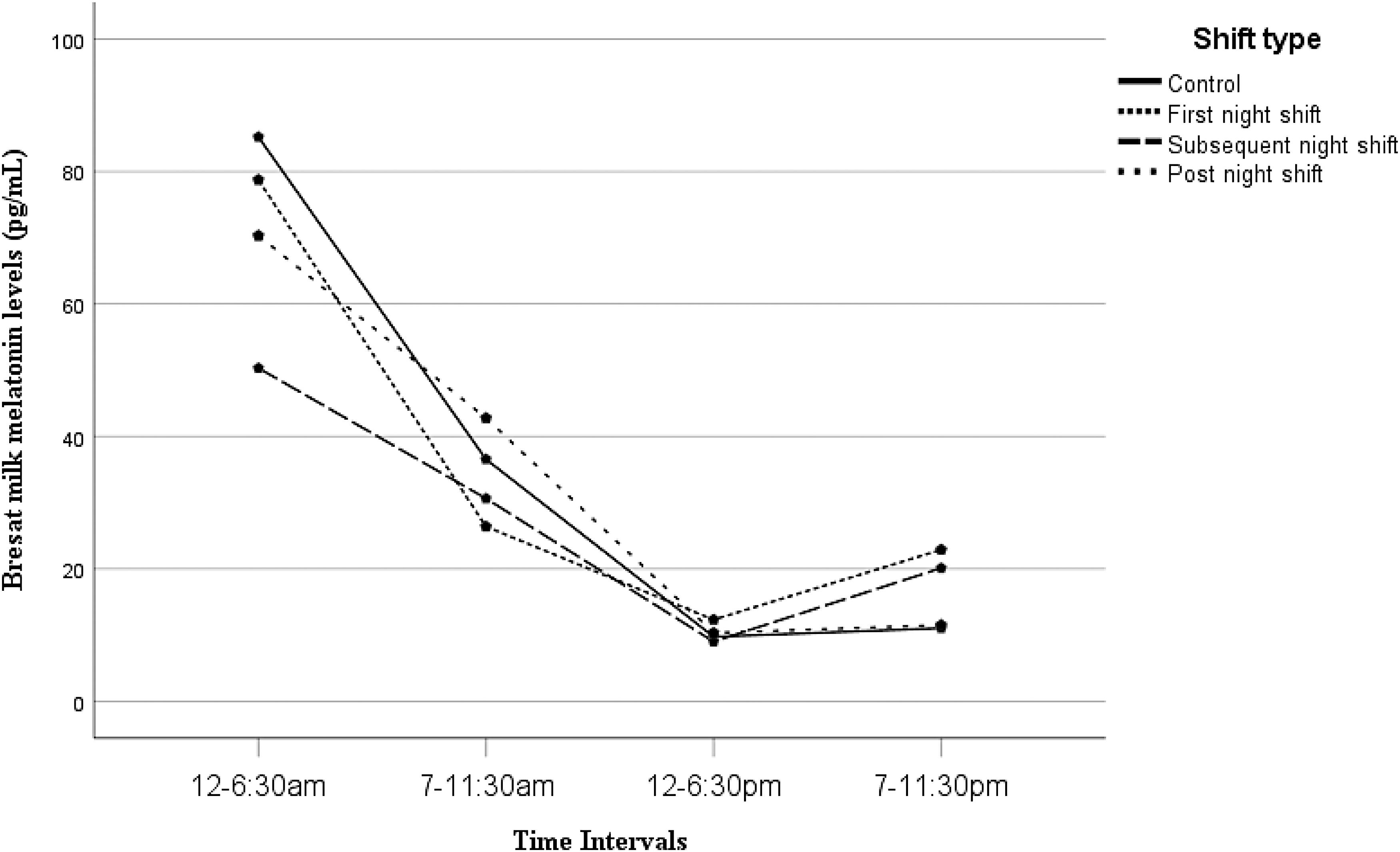
ANOVA showed that there was a significant difference in breast milk melatonin at the 12–6:30 am time interval, with melatonin levels decreasing significantly in participants on subsequent night shift (M = 38.79 ± 12.48 pg/mL), compared with control days (M = 84.17 ± 10.04 pg/mL, p = 0.026). The other time intervals remained stable across the different shift types (Fig. 1.). However, general linear modeling showed that, although there was an overall trend showing that melatonin in breast milk reduced on subsequent night shifts compared with control days, there was no interaction effect between time interval and shift type (p = 0.70) (Fig. 2). There was also no significant difference found in melatonin levels of breast milk collected at pre- versus postfeed (p = 0.91).

Mean melatonin (pg/mL) in breast milk at each time interval, across each of the different shift types. *Significant difference between the control and subsequent night shifts at the 12–6:30 am time interval. The other time intervals stayed relatively stable across shift type. pg/mL, picogram per milliliter.
Estimated margin mean from the general linear model showing the shift type changes in breast milk melatonin (pg/mL) at each of the four time intervals. There was a decline in melatonin during subsequent night shifts, compared with the control days but there was no significant time and shift interaction effect (p = 0.70).
Saliva melatonin levels
Melatonin in saliva showed a similar circadian pattern to the breast milk melatonin concentrations. At the 12–6:30 am time interval, there was an observed increase in melatonin postnight shift (M = 21.15 ± 24.53 pg/mL), compared with the control days (M = 12.97 ± 13.69 pg/mL); however, this was not significant (p > 0.05). General liner models showed there was no time and shift interaction effect (p = 0.71; Fig. 3).
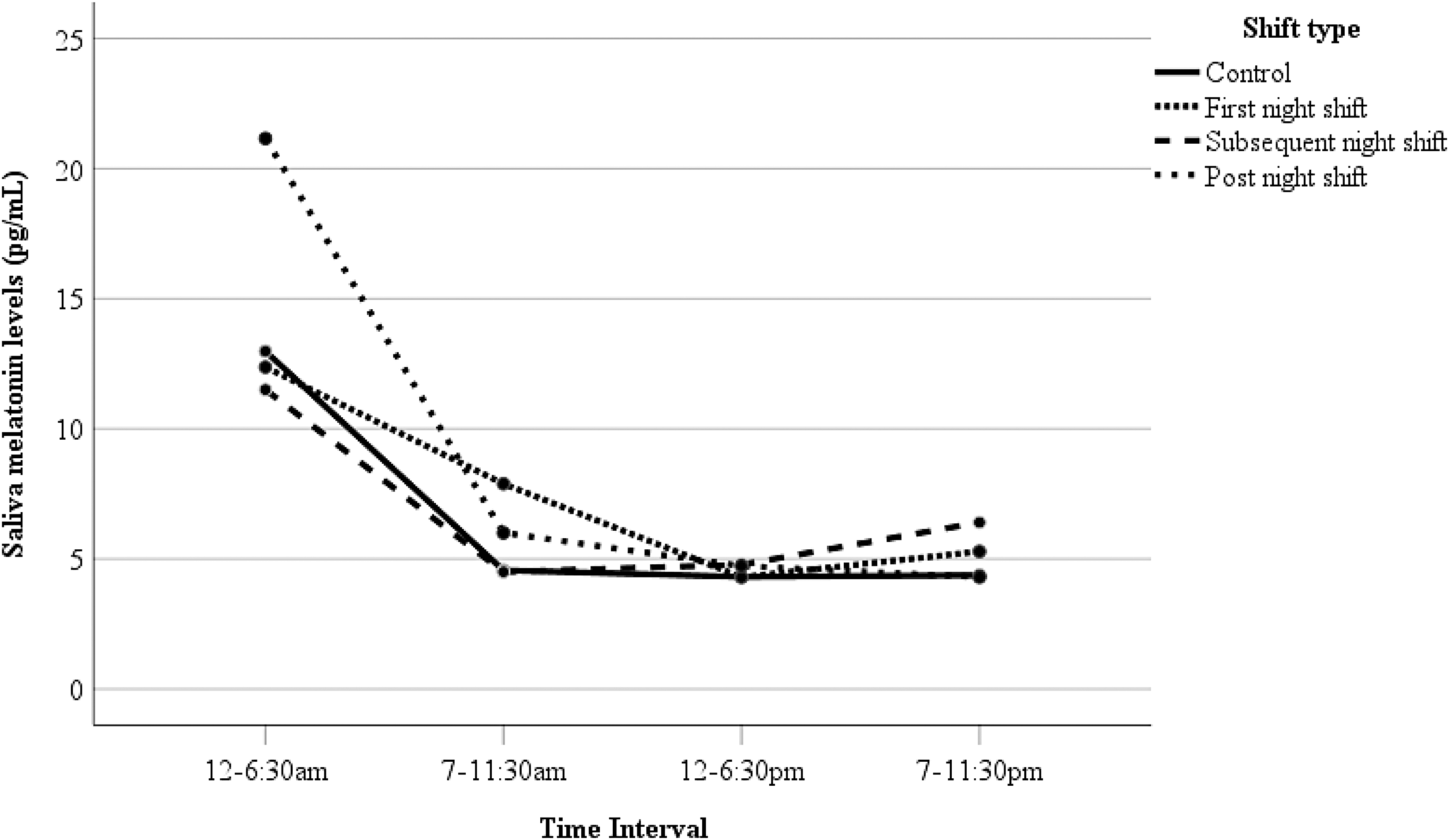
Results from the general linear model showing the shift type changes in saliva melatonin (pg/mL) at each of the four time intervals. There was a decline in melatonin during subsequent night shifts but not significantly different (p = 0.71).
Saliva versus breast milk melatonin
Table 1 shows that there was a significantly higher average level of melatonin in breast milk, across all the samples, compared with saliva samples (p < 0.001) at each observed timepoint except between 12 and 6:30 pm (p = 0.053).
Overall Melatonin Levels (Picogram Per Milliliter) in Saliva Versus Breast Milk at Each Time Interval (Mean ± Standard Deviation)
Discussion
This study aimed to investigate if maternal circadian rhythm disturbance from shift work impacted on the melatonin concentration in the mothers' breast milk. Overall, there was a trend suggestive of a possible effect of shift type, particularly early morning (12–6:30 am), where there was more melatonin evident in the control days compared with subsequent night shifts; however, there was no significant time and shift interaction effect. In addition, we found no difference in melatonin levels in maternal saliva at each time interval against shift type and no significant differences between pre- and postfeed melatonin levels in breast milk samples. Of interest, melatonin levels in breast milk were significantly higher than in maternal saliva at three of the four-time intervals.
Although not significant, results showed a possible alteration to circadian timing across shift types, with a decrease in melatonin levels in breast milk early in the morning, especially after multiple night shifts. This is still an important finding and similar to past research, which shows that there can be a reduction or delay in melatonin production when adults work night shift,5,27 and that this is noticeable either at the beginning of the night, or early in the morning.26,37 In this study, saliva melatonin showed a similar pattern to that observed in breast milk, but this was not significantly different across any time or shift types. This suggests participants may not have experienced enough of a circadian disruption from working night shift to see a change, which may explain some of the lack of changes seen in breast milk melatonin timings from certain participants.
Research shows that there is a large amount of individual variability when adapting to nightshift work, with some people exhibiting a phase delay, some a phase advance, and others may show no phase shift in the timing of melatonin. 38 However, in this study night shift, especially subsequent night shifts, still seemed to stifle early morning breast milk melatonin levels, and that even postnight shift melatonin levels did not increase to reflective control levels.
Looking at the relationship between breast milk and saliva melatonin, this study found that melatonin was significantly higher in breast milk than in saliva at three of the four time intervals. This suggests that melatonin in breast milk may indeed be providing greater circadian timing cues than first envisaged, providing an important function in infant sleep and circadian rhythm development in the first few months of life. 10 Follow-up studies are needed to explore the transfer of melatonin from breast milk to the infant and objectively measure infant serum melatonin levels in relation to consumed breast milk.
The outcomes from this project provide important evidence that further research is warranted. With the increasing demand for our society to operate 24/7, the number of people employed in shift work is increasing. Approximately a quarter of workers in Australia (1.5 million people) are employed in shift work. 39 In addition, more mothers are returning back to work when their infants are at an age when they are likely to still be receiving breast milk, with currently ∼22% of mothers in Australia returning back to work when their child reaches 6 months of age and ∼50% by the time their child is 12 months old. 40 Therefore, the results highlight the value of exploring impacts of circadian disruption, such as from shift work, on breast milk hormones as well as paves the way for future trials to explore any long-term consequences of mistimed circadian hormonal timing from breast milk on an infant.
For example, research is showing that mistimed hormonal timing in breast milk may impact on an infant's sleep. 41 Consequently, when infants are not sleeping well, parents invariably also do not sleep well, which can affect family life and risk of postnatal depression. 42 Therefore, optimizing the development of circadian rhythmicity is crucial for optimal health and wellbeing for both the infant and the parents. Larger, longitudinal projects monitoring the effect of different feeding types and hormonal timing of breast milk on objective sleep of the infant and mother would be beneficial to observe any long-term impacts.
This study is however not without limitations. The narrow criteria and protocol for the project meant that it was difficult to recruit. Initially, the original study design was to recruit mothers who were working three night shifts in a row based on past research that show two consecutive night shifts may not significantly alter the normal circadian rhythms in the body for everyone. 43 However, recruiting breastfeeding mothers with this shift schedule proved difficult. Therefore, the small sample size in this study is a limitation that may have impacted statistical power to detect a significant difference. Also, owing to the natural observational nature of this study, it was difficult to control many factors. One such factor was the collection of saliva samples, with melatonin susceptible to light exposure and the reliance on participants being able to collect samples under similar conditions each day.44,45
Another key factor was the difficulty for participants to express breast milk samples at the exact same time, as we were at the mercy of feeding and work schedules. In addition, the project had some missing sample data, because not all participants collected the total amount of samples required, 20 tubes could not be assayed because they contained insufficient volume to assay and 4 other tubes were also cracked at the bottom and leaked when thawed out, so not enough volume could be recovered to assay. Fifteen other samples only had enough volume to assay in single rather than duplicate. Future research could benefit from exploring other methods for examining maternal circadian timing and/or consider using laboratory-based studies to control for such factors.
Impact and significance
This is the first study to our knowledge that has explored the impact of disturbances of maternal circadian rhythm, such as from shift work, and consequently, the impact on the circadian rhythmicity of breast milk. Therefore, the project provides important information to help fill-in this gap in knowledge and also provides preliminary evidence that this issue warrants further exploration. If hormone signals in breast milk do indeed help to calibrate infant circadian biology, infants who drink mistimed hormonal breast milk may struggle more with sleep, 46 as well as with development, growth, and long-term health consequences. 32 As a result, larger, longitudinal studies are required and the expansion of this research to other circadian rhythm misalignment sleep disorders is highly recommended.
Conclusion
Findings from this study suggest that maternal circadian rhythm disruption from shift work has a potential effect on breast milk melatonin timing. This outcome provides an important first step in providing evidence that further investigation is both warranted and required.
Footnotes
Acknowledgments
The team thanks all the mothers who took time out to participate in the study and the team at the Adelaide Research Assay Facility, Adelaide University for facilitating the sample analysis.
Authors' Contributions
L.A.B., J.S., M.D.-C., D.W., T.C.S. were responsible for study design, data interpretation, and composing and editing the article. K.E.L. and D.W. were responsible for data collection. L.A.B., T.C.S., and C.F. performed the analysis and J.S., C.F., and D.W. contributed to the interpretation. All authors were involved in preparing the article. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Disclosure Statement
No competing financial interests exist.
Funding Information
Norman Beischer Medical Research Foundation Innovation Grant.