
Abstract
Background:
Obesity is characterized as a low-grade chronic inflammatory state, marked by elevated inflammatory biomarkers. Breast milk (BM) is rich in nutritional elements, vitamins, minerals, immunological factors, and bioactive components. These bioactive components, capable of influencing biological processes, may vary in concentration based on maternal body composition.
Research Aim/Question(s):
This study aimed to explore the association between pro-inflammatory cytokine levels (interleukin-1 beta [IL-1β], interleukin-6 [IL-6], and tumor necrosis factor-alpha [TNF-α]) in human colostrum and maternal body composition, as analyzed through bioelectrical impedance vector analysis (BIVA).
Method:
In this cross-sectional study, 117 healthy postpartum participants were included, with each group (normal weight, overweight, and obese) comprising 39 individuals, as classified by BIVA. Colostrum samples were collected within the first 24 hours postpartum.
Results:
IL-1β levels did not significantly differ across the groups, with concentrations of 69.5 ± 103 pg/mL in normal-weight, 79.7 ± 97.9 pg/mL in overweight, and 68.7 ± 108 pg/mL in obese women. IL-6 levels were significantly higher in the overweight group (55 ± 72.4 pg/mL) than in the normal-weight (48.1 ± 74.1 pg/mL) and obese groups (28.9 ± 36.2 pg/mL) (p = 0.02). Similarly, TNF-α levels were higher in the overweight group, with concentrations of 58.7 ± 74.9 pg/mL, than in the normal-weight group, with concentrations of 38.6 ± 95.4 pg/mL, and 52.6 ± 115 pg/mL in obese women (p = 0.02).
Conclusion:
This study shows that IL-6 and TNF-α concentrations were statistically higher in the colostrum of overweight women, suggesting that maternal body composition may influence the inflammatory profile of BM.
Background
Overweight and obesity are defined by the World Health Organization as excessive or abnormal accumulation of fatty tissue that can be detrimental to health. 1 The body mass index (BMI) is suggested as a simple indicator to identify overweight; however, this index does not reflect changes in body composition. 2 The high prevalence of obesity and overweight in women of childbearing age has made these a common problem during pregnancy that impacts the incidence of maternal–fetal complications. 3
In pregnancy, there are both physiological and body composition changes to support fetal growth and development. These changes lead to an increase in body weight. 4 Therefore, it is difficult to assess body composition in pregnancy with commonly used indicators, as these are based on assumptions about body composition. The gold standard, which is dual X-ray absorptiometry, cannot be used during this period. 5
The use of bioelectrical impedance vector analysis (BIVA) has been proposed during pregnancy as a semiquantitative, noninvasive method for assessing cell mass and body water content. 6 It has the advantage that it does not rely on predictive equations or assumptions about body composition, as they are modified during this period, and it is a valid and safe method for pregnant women.7,8
Obesity mimics a low-grade chronic inflammatory disease. It has been associated with elevated serum levels of inflammation markers, such as C-reactive protein (CRP), an acute-phase protein; interleukin 6 (IL-6), interleukin 1β (IL-1β), and tumor necrosis factor α (TNF-α), which are pro-inflammatory cytokines.9,10
The initial phases of human development, encompassing the intrauterine period and infancy (the initial two years of life), play a crucial role in determining health outcomes in later stages. 11 According to the theory of metabolic programming, alterations in metabolism during these periods heighten the risk of various diseases in subsequent life stages. 12 During intrauterine growth, the fetus is vulnerable to different factors that depend on maternal tissues.13,14 During lactation, the infant is exposed to different factors that influence metabolic programming. 15 Postnatal changes interact with those occurring during fetal development to increase the risk of disease. 16
Breast milk (BM) comprises nutrients and various bioactive components essential for supporting infant development. 17 Its composition is dynamic and complex, and it is influenced by physiological, infant, and maternal factors. 18 Bioactive components in BM are elements capable of influencing biological processes or substrates, with some playing a key role in the maturation of the immune and gastrointestinal systems, as well as possessing immunomodulatory functions. 19 Through these mechanisms, bioactive compounds in BM can enter the infant’s bloodstream and significantly impact development. 20 One of the bioactive components of BM are cytokines, which have a role in the inflammatory response, as pro- or anti-inflammatory agents, acting as hormones in tissues through autocrine and paracrine mechanisms, or facilitating maturation. 21 The cytokines IL-6, TNF-α, and IL-1β have been associated with a pro-inflammatory state caused by obesity, and they are also among the cytokines that have been found in higher concentrations in human milk (HM).10,21
The impact of nutritional status on HM cytokine content has been a topic of interest; however, it remains poorly characterized. Several studies have been carried out in which the concentrations of IL-6, IL8, IL-10, and TNF-α have been measured, and no significant differences between groups according to maternal BMI in the crude or adjusted model were found; however, differences between CRP were found.11,20,22
Fujimori and colleagues assessed cytokines (IL-6, IL-10, and TNF-α) in both serum and colostrum across a group of 45 women categorized as normal weight, overweight, and obese. They reported that the highest serum concentrations of IL-6 and TNF-α were found in obese mothers, whereas the variations in colostrum did not reach statistical significance. 23
Maternal body composition may influence the variability in proinflammatory cytokine levels in colostrum, which initially plays roles in signaling and inflammation. These cytokines can impact the development of an infant’s immune and gastrointestinal systems, influence nutrient utilization, and affect genetic, metabolic, and epigenetic processes, potentially leading to changes in the infant’s health both in the short and long term.24,25
Despite studies aiming to establish a connection between maternal BMI and cytokine content in HM, encompassing various cytokines, no definitive correlation has been identified between maternal nutritional status and cytokine levels.11,20,22,23,26
Aim
This study aimed to explore the association between pro-inflammatory cytokine levels (IL-1β, IL-6, and TNF-α) in human colostrum and maternal body composition, as analyzed through BIVA.
Method
Study design
In this cross-sectional study, 117 healthy postpartum women were categorized into three groups based on their body composition determined by bioelectrical impedance vectors: normal weight (n = 39), overweight, and obese. Colostrum samples were collected within the first 24 hours postpartum.
Setting
Data collection for the study occurred from July 2021 to February 2022, at the gynecology department of a secondary care hospital and the University’s Laboratory of Molecular Biology and Epigenetics.
Sample
The study population comprised postpartum women of age 18–35 years who had experienced a full-term, normal delivery from 37 to 42 weeks of gestation. Exclusion criteria included individuals with preexisting chronic conditions (such as chronic kidney disease, arterial hypertension, rheumatologic, oncologic, autoimmune diseases, asthma, and diabetes mellitus), those with multiple pregnancies, individuals with substance use disorders, and those with any diseases associated with pregnancy. Participants from whom insufficient samples were obtained or who fell outside the 75th percentile tolerance ellipse for cachexia and malnutrition according to BIVA were also excluded. The study received ethical approval and was registered with COFEPRIS (Comision Federal para la Protección contra Riesgos Sanitarios) under number 17 CI 24 028 093. All participants were informed about the study details and provided their consent by signing an informed consent form.
Measurement
Each participant’s profile, including age, body composition, gestational frequency, duration of gestation, BMI, resistance, reactance, phase angle, and cytokine levels (IL-1β, IL-6, TNF-α), was comprehensively recorded. The categorization of BMI for pregnant women was determined by their pregestational BMI, using the classification criteria set by WHO or similar guidelines. 27 Although this methodology offers a standardized approach for classification, it is critical to recognize its constraints, especially during pregnancy. Pregnancy is characterized by distinctive physiological changes, such as weight gain and body composition shifts, which pregestational BMI may not comprehensively account for. Unlike BMI, BIVA relies on direct bioelectrical impedance measurements, avoiding the use of assumptions, or predictive formulas to evaluate body composition and fluid distribution.
BIVA uses directly measured resistance (R) and reactance (Xc), plotting these measurements onto a vector graph within reference ellipses for comparison with a standard population. Body composition evaluation was conducted using the Quantum X body composition analyzer (RJL, Clinton Township, Michigan, USA), BIVA, at a frequency of 50 kHz. The protocol involved arranging participants in a supine position on an insulated surface, with arms angled 30 degrees from the torso and legs separated. Electrodes were affixed to the cleaned skin of participants’ hands and feet. Assessment cables were color-coded: red for proximal and black for distal connections. The analyzer, once activated, recorded resistance and reactance values. Calibration of the RJL Quantum X device was performed with a resistance standard between 495–505 ohms to verify measurement accuracy.
Participant classification into categories (normal weight, overweight, obese) was achieved through the following specific steps: Collected data were processed in an Excel application featuring a macro designed for plotting against tolerance ellipses, based on the Mexican reference population (Espinosa et al. 28 ). The application adjusted resistance and reactance measurements according to height, producing plots for each individual. Classification criteria were dependent on the participants’ placements within percentile-defined ellipses: normal weight (p50 to p75), overweight (p75 to p95 on the left), and obese (beyond p95 on the left).
Data collection
Colostrum sampling was performed in the postprandial period, 30–90 minutes after breakfast, within the first 24 hours postpartum. Participants received verbal instructions regarding the procedure before the collection of colostrum samples into 50-mL tubes, with an optimal sample volume identified as 2–5 mL per tube.
Colostrum samples were initially frozen and stored at −80°C for subsequent analysis. The frozen samples were thawed at room temperature to prepare them for analysis. The lipid fraction of the milk was isolated from the aqueous phase by centrifugation at 3990 g for 10 minutes at 4°C. The aqueous phase of the samples (referred to as skimmed milk) was exclusively collected, with uniformity ensured by gentle agitation during pipetting.
For cytokine analysis, 200 µL of the aqueous phase was transferred into flow cytometry tubes. Samples were labeled with specific antibodies and incubated for 40 minutes in an environment protected from light. The “‘Human Premixed Multi-Analyte’ commercial kit (R&D Systems, Bio-Techne, Minneapolis, Minnesota, USA) was used for the simultaneous detection of the three cytokines, namely, IL-1β, IL-6, and TNF-α”. Samples were analyzed using a Luminex plate reader (R&D Systems), with a minimum of 100,000 events counted.
Subsequently, the samples were processed, and the analysis was performed using a multiplex bead-based fluorometric assay (Luminex plate reader) counting at least 100,000 events with a Human Premixed Multi-Analyte commercial kit (R&D systems) which detects the cytokines of interest simultaneously.
Sample size
Using the power formula for analysis of variance (ANOVA) across three groups, a significance level of 0.05 and a statistical power of 0.8 were set. An effect size of f = 0.347 for TNF-α required a total of 28 patients, and an effect size of f = 0.29 for IL-6 required 39 patients, in alignment with the findings of Fujimori et al. 23
Statistical analysis
The data were analyzed using R software, version 4.02, for MacOS. To ascertain the measurement accuracy of the outcome variables, concordance analysis for anthropometric variables, including maternal weight, height, and bioimpedance, was conducted between the principal and collaborating investigators. The agreement was evaluated using the Portable Skinfold Thickness Measurement System with 12 volunteers (7 from the practical workshop and 5 additional volunteers), whose weight, height, and bioimpedance were measured with the same equipment used for all participants.
This analysis was performed using a two-factor repeated-measures ANOVA with a mixed-effects model using Lin’s intraclass correlation coefficient (ICC3), presupposing that the ‘n’ subjects represent a random sample and the ‘k’ assessors embody the complete set of assessors. Results revealed an ICC of 0.9999 for weight (95% CI: [0.9996, 0.9999]), 0.986 for height (95% CI: [0.962, 0.995]), 0.997 for resistance (95% CI: [0.993, 0.999]), and 0.964 for reactance (95% CI: [0.904, 0.987]). For each of the variables, an ICC greater than 0.95 was obtained.
The normality of the continuous variables was assessed with the Shapiro–Wilk test and corroborated via QQ-plot graphs, while the homogeneity of variances was examined using the Levene test. Given the non-normal distribution of both IL-6 and TNF-α levels, the analysis of cytokine associations was conducted using the Kruskal–Wallis test, followed by the Siegel & Castellan post hoc multiple-comparison test. 29
Multivariate linear regression was then applied to each response variable, namely, IL-1β, IL-6, and TNF-α levels, with resistance, reactance, phase angle, age, and gestation serving as the explanatory variables. This approach was intended to explore the degree to which these variables may explain the observed cytokine-level variations.
Results
A total of 317 patients were assessed for eligibility. After applying our inclusion and exclusion criteria, 170 women were excluded, primarily because of chronic conditions such as hypertension, rheumatologic diseases, diabetes mellitus, and pregnancy-related conditions including gestational diabetes and preeclampsia, in addition to a history of tobacco use (at least one cigarette per day). Consequently, 30 participants were excluded from the study upon reaching the targeted recruitment numbers for their respective groups. A total of 117 participants were included in the study, with each group (normal weight, overweight, and obese) comprising 39 individuals, classified by BIVA.
The enrollment target for the obese group was achieved last, attributable to a comparatively smaller pool of pregnant women with uncomplicated pregnancies qualifying for this specific classification according to BIVA criteria. Except for three individuals who declined to participate, all prospective participants provided informed consent willingly.
The mean age of the participants was 25.3 ± 5.1 years. The classification was achieved by plotting resistance and reactance values, adjusting for height from bioimpedance measurements, on tolerance ellipses, and categorizing participants according to their percentile on the body tissue axis (Fig. 1). The mean ages were 23 ± 4.36 years for the normal weight group, 24.7 ± 5.29 years for the overweight group, and 28.1 ± 4.49 years for the obese group, with a significant difference observed between groups (p < 0.0001).
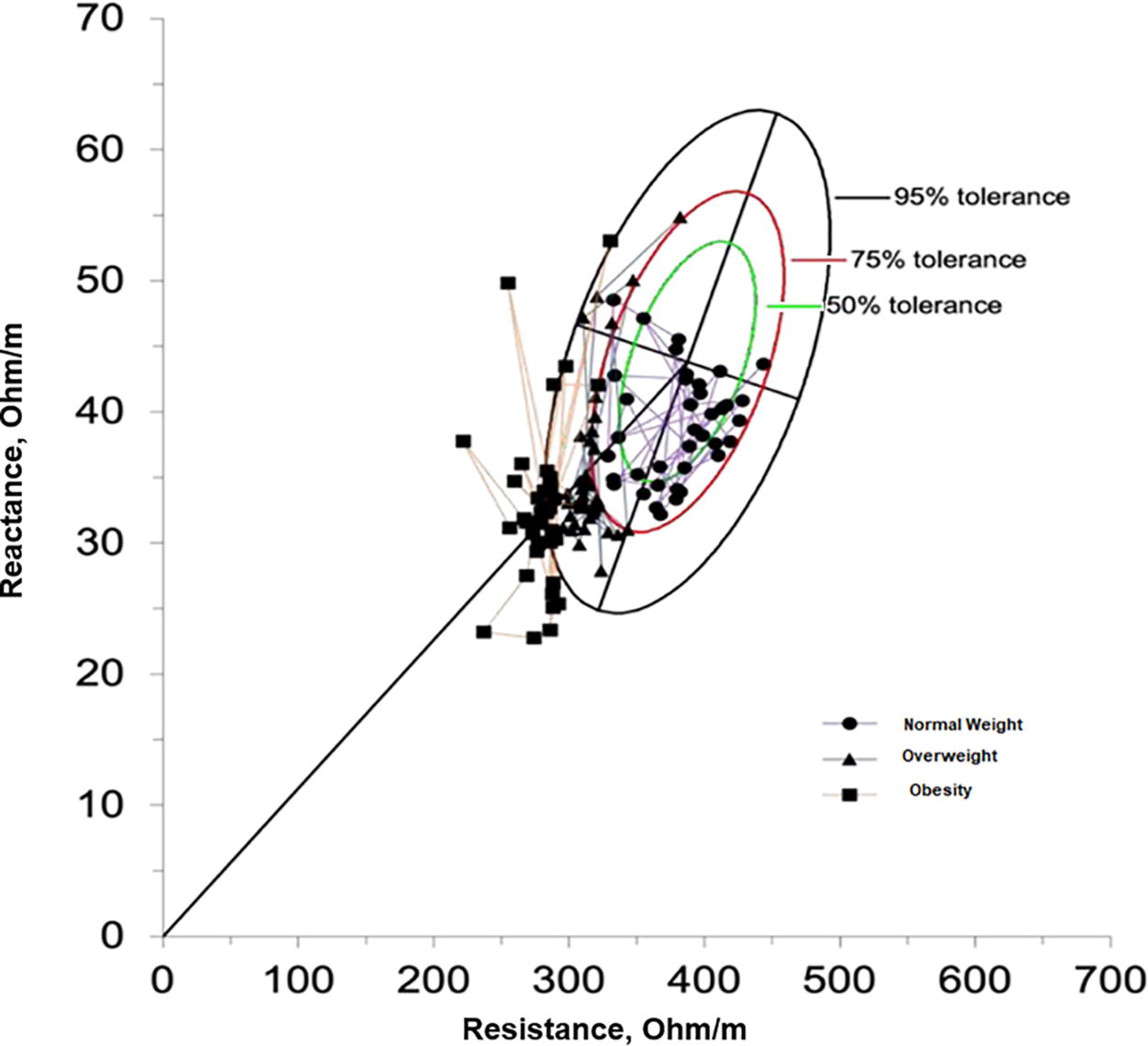
Analysis of bioimpedance vectors of participants. Xc/H: reactance; R/H: resistance.
The median number of deliveries was one for the normal-weight group and two for both the overweight and obese groups, with no significant differences identified. Regarding the number of gestations, the median was two for both the normal-weight and overweight groups, and three for the obese group (Table 1), with a significant difference (p < 0.005) observed among groups.
Basal Participant Characteristics
ANOVA.
Kruskal–Wallis test.
Furthermore, the mean pregestational BMI, calculated using the weight reported by the participants before pregnancy, was found to be 22.5 ± 2.99 kg/m2 for the normal-weight group, 28.7 ± 3.89 kg/m2 for the overweight group, and 29.5 ± 4.99 kg/m2 for the obese group, with significant differences noted between these groups.
Significant differences were identified among the three groups in variables indicative of maternal nutritional status, including pregestational BMI, postpartum BMI, and bioimpedance measurements of resistance and reactance, with a p value < 0.0001 (Table 1 and Fig. 2).
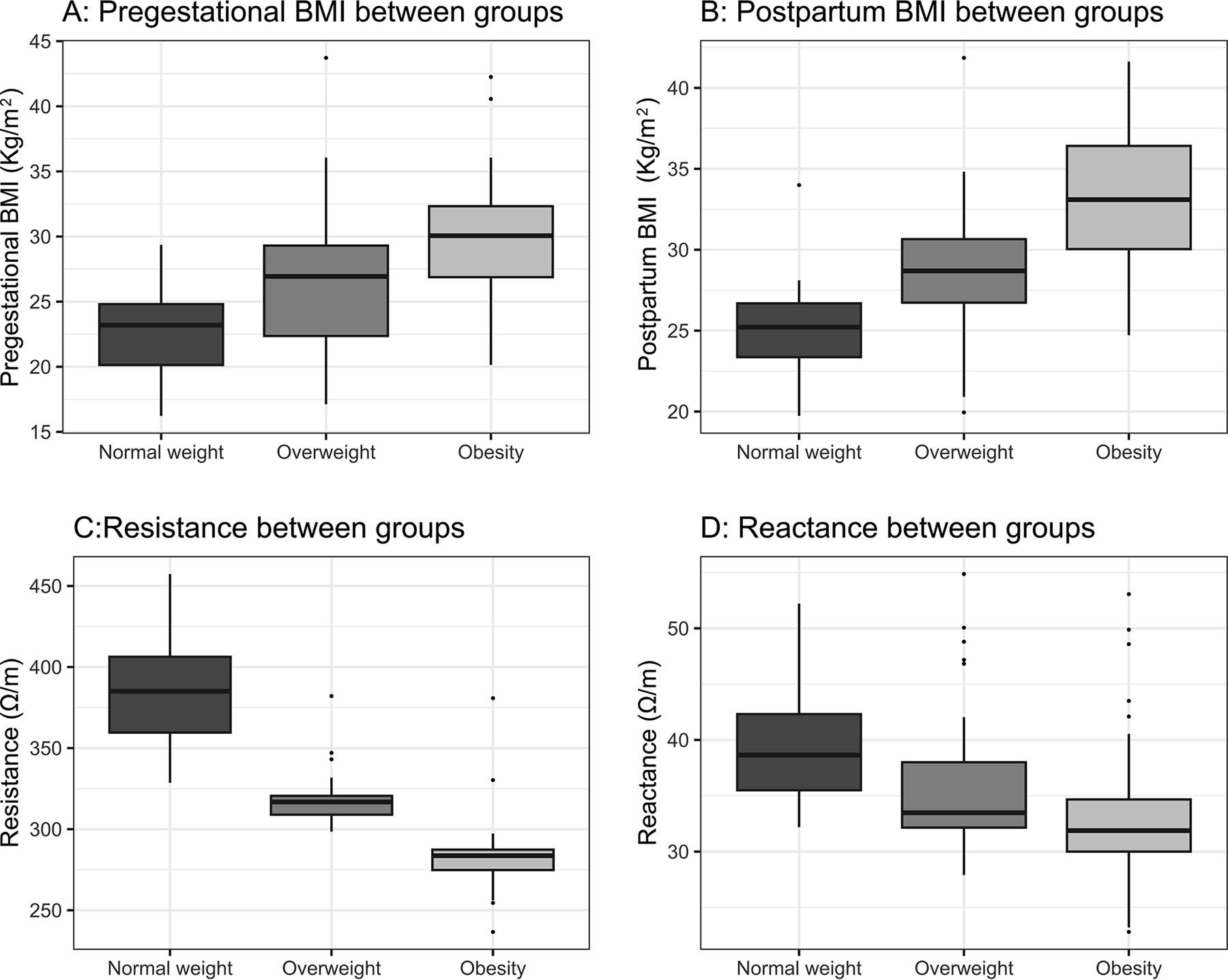
Differences in nutritional state between groups.
Regarding IL-1β concentration in maternal colostrum, average levels were measured at 69.5 ± 103 pg/mL for the normal-weight group (n = 39), 79.7 ± 97.9 pg/mL for the overweight group (n = 38), and 68.7 ± 108 pg/mL for the obese group (n = 37). Our analysis revealed no significant difference in IL-1β concentrations across the groups (p = 0.11), yet a trend toward elevated levels in the overweight group was noted (Fig. 3), with an effect size of η2 = 0.021 documented (Table 2).

Differences between pro-inflammatory cytokine groups.
Differences in Cytokine Concentration in Human Colostrum
Kruskal–Wallis test.
p < 0.05 in post hoc test (Siegel and Castellan).
In the analysis of IL-6 concentrations in colostrum, mean values were recorded as 48.1 ± 74.1 pg/mL for the normal-weight group, 55 ± 72.4 pg/mL for the overweight group, and 28.9 ± 36.2 pg/mL for the obese group. The overweight group had highest significant difference among groups (p = 0.02), with an effect size of η2 = 0.05. The Siegel and Castellan post hoc comparison analysis revealed significant differences in IL-6 levels between the overweight and obese groups (p < 0.05; Table 2).
For TNF-α concentrations in colostrum, mean value was 38.6 ± 95.4 pg/mL for the normal-weight group, 58.7 ± 74.9 pg/mL for the overweight group, and 52.6 ± 115 pg/mL for the obese group, with a statistically significant difference observed across the groups (p = 0.02; Fig. 3). The effect size was small, with an η2 = 0.04. Subsequent post hoc analysis identified a significant difference in TNF-α concentrations, where the overweight group had a higher level than normal-weight (p < 0.05; Table 2).
When comparing TNF-α levels between the normal-weight and overweight groups, a significant mean difference of −9.81 (95% CI: [−24.6 to −2.9]) was identified (p = 0.003), with the overweight group exhibiting higher levels than the normal-weight group. This finding indicates a greater significance relative to the analysis involving all three groups (Table 3).
Differences in Cytokine Concentration in Colostrum among Normal-Weight and Overweight Groups
Mann–Whitney U test.
A regression analysis was conducted to examine the relationship between various factors (resistance, reactance, phase angle, age) and cytokine concentrations. After assessing for multicollinearity, the backward stepwise method was applied to simplify three statistical models. Despite these efforts, no significant predictors were identified in either the preliminary or refined models. Furthermore, a comparison of the simplified model to its initial version revealed no substantial differences.
Discussion
This study aimed to explore the relationship between the concentrations of pro-inflammatory cytokines (TNF-α, IL-1β, and IL-6) in human colostrum during the first 24 hours postpartum and maternal body composition. Our findings indicated no linear correlation between the levels of these cytokines and maternal body composition components. However, variations in the TNF-α and IL-6 concentrations were observed among the groups studied owing to a significant increment in the overweight group. This outcome suggests the possibility of a nonlinear association between the groups, potentially attributable to individual differences among mothers.
Regarding our primary aim, there was no observed direct or proportional relationship between cytokine levels and maternal body composition components. This observation may be attributed to the fact that cytokine levels were lower in the obesity group than in other study groups. A distinct trend emerged, showing the most pronounced pro-inflammatory state in the overweight group, in contrast to colostrum from normal-weight mothers. In samples from mothers classified as obese, cytokines were present in reduced concentrations, showing no significant difference from those of normal weight. Previous reports have indicated that the most significant changes in inflammatory and metabolic parameters occur during the overweight stage. Upon reaching obesity, adaptive processes ensue, including tolerance and a diminished response to inflammatory stimuli, attributed to the exhaustion from a sustained chronic low-grade inflammatory state. 30
TNF-α was the sole cytokine to exhibit a significant difference between the normal-weight and overweight groups. This discrepancy might suggest that TNF-α acts as a catalyst contributing to divergent responses to the pro-inflammatory state encountered during pregnancy among participants of normal-weight and those overweight; alternatively, it might reflect an adaptive feedback mechanism beneficial for the newborn.
Contrary to our initial hypothesis, a reduction in cytokine levels within the obese group was observed, deviating from the anticipated linear relationship. This finding is particularly unexpected given that physiological conditions typically prompt an increase in IL-6 levels throughout pregnancy. 31 In the overweight group, unidentified biochemical factors seemingly contribute to an acute pro-inflammatory state.
Strength and limitations
One strength of this study is its classification of participants using bioimpedance analysis at the time of admission, rather than pregestational BMI. Another benefit includes the standardized criteria for sampling, which helps to minimize variations in BM composition that might occur because of time of day or differences between feedings. The study also exclusively involved healthy women who experienced no complications during pregnancy or delivery, had no infections in the last trimester, and were recruited in the postpartum period within the first 24 hours, reducing certain factors that could affect cytokine concentration.
However, the current study had certain limitations, notably the potential that, despite performing a sample size calculation informed by prior research, the sample power may have been insufficient to discern differences between groups with adequate precision. Nevertheless, a trend was noted indicating elevated proinflammatory cytokine levels progressing from the normal-weight group to the overweight group, which then appeared to decline from the overweight to the obese group.
Conclusions
This study shows that IL-6 and TNF-α concentrations were statistically higher in the colostrum of overweight women, suggesting that maternal body composition may influence the inflammatory profile of BM. This study serves as an initial exploration into the concentrations of pro-inflammatory cytokines (TNF-α, IL-6, and IL-1β) within the colostrum of healthy women across various body compositions. However, additional research is necessary to enhance our comprehension of the inflammatory milieu associated with breastfeeding and pregnancy, along with the potential effects these variations might exert on neonatal health.
Footnotes
Authorship Contribution Statement
M.V.M.: Conceptualization, methodology, investigation, formal analysis. S.B.M.: Conceptualization, methodology, supervision. L.R.M.V.: Investigation, supervision, project administration. F.G.J.A.: Formal analysis, data curation, writing original draft. P.P.M.: Conceptualization, methodology, supervision, writing original draft.
Disclosure Statement
All authors declare that they have no conflicts of interest.
Funding Information
No funding was received for this article.