
Abstract
Background:
Mother’s own milk (MOM) provides health benefits for infants with very low birth weight (VLBW). This study aimed to describe the incidence and factors associated with low volumes of MOM (<50% of total diet volume) at discharge for VLBW infants.
Methods:
A prospective cohort study of infants with VLBW and gestational age of <30 weeks, who survived to discharge and had no contraindication to MOM. We conducted bivariate analyses to investigate associations with the volume of MOM at discharge, using chi-square, t, and Mann–Whitney tests. All p-value analyses were two-tailed. The variables significantly associated with “low volumes of MOM” entered the multivariable analysis. Univariate and multivariate relative risk (confidence interval [CI] 95%) estimates were obtained from Poisson regression with a robust estimate of variance and controlled by the length of hospital stay.
Results:
Of 414 infants included and followed until discharge, 32.9% (n = 136) received less than 50% of the total daily volume of MOM. This outcome was associated with gestational age <28 weeks, lower birth weight, multiple births, developing bronchopulmonary dysplasia, and longer lengths of stay. After Poisson regression, low volumes of MOM at discharge were associated only with being born multiples (RR 2.01; CI 95% 1.53–2.64, p < 0.001) and with longer length of stay (RR 1.07; CI 95% 1.01–1.14, p = 0.01).
Conclusions:
Most VLBW infants were discharged home receiving predominantly MOM. Each neonatal intensive care unit (NICU) should acknowledge which clinical characteristics of mothers and VLBW infants are associated with difficulties maintaining MOM volumes until discharge.
Background
Human milk is the best nutrition for preterm infants, especially in middle- and low-income countries. 1 If mother’s own milk (MOM) is the best choice for all infants, this is especially true for the most vulnerable ones: preterm infants in the neonatal intensive care unit (NICU). 2 Very low birth weight (VLBW) infants who receive higher volumes of MOM might have a reduction in both morbidity and mortality. 3 Human milk has many properties that balance the VLBW response to oxidative stress4,5 and modulate immune response,6,7 especially when unpasteurized. Most of those benefits depend on the volume offered 8 and the longer duration that MOM is available. Therefore, it is essential to offer MOM to preterm infants and increase the proportion and time it is offered.
Mothers of preterm infants face many challenges initiating and maintaining lactation for extended periods. Extremely preterm infants cannot directly breastfeed for a long time, and as a result, their mothers depend on artificial means of milk expression to provide feedings for their infants. Other factors, such as biological difficulties, socioeconomic determinants of health (years of education and income), and prenatal and neonatal morbidities have been reported.9,10
According to the data published in the “Born Too Soon” report, 1 Brazil is one of the ten countries that accounts for 60% of the world’s preterm births by rank. In Brazil, breastfeeding is a part of the Brazilian culture, and breastfeeding occurs for the first time in the delivery room for most infants. 11 An extensive report that comprehended a national collection database 12 showed that exclusive breastfeeding rates among children younger than 6 months increased from less than 30% to 45.7%. All those studies report breastfeeding rates regardless of gestational age. A previous study conducted in our NICU showed a high prevalence (93.4%) of VLBW breastfed at least once a day at discharge. 13 No data report breastfeeding rates and factors associated with this outcome at NICU discharge in Brazil’s VLBW infants.
Methods
Aim
This study aimed to describe the incidence and factors associated with low volumes of MOM (<50% of total diet volume) at discharge for VLBW infants in a private NICU in southern Brazil.
Design
We conducted a prospective cohort study in a 27-bed level III private NICU at Porto Alegre, Rio Grande do Sul, Brazil. This study design was appropriate for investigating factors associated with low volumes of MOM rates at NICU discharge in VLBW infants.
Setting
The study was carried out at a private level-III NICU in the southern region of Brazil. According to the most recent data, breastfeeding rates vary from 86.8% at 30 days to 69.7% at 6 months in the city where the study was conducted. 14 The hospital is a private nonprofit institution that cares for patients with private insurance, representing 43% of the city’s population. 15
An annual average of 4,500 births occurred throughout the study period, with 500 infants requiring admission to the NICU per year. Among these admissions, approximately 60 infants fell into the VLBW category. All decisions concerning infant nutrition, including initiation, progression, fortification, and the cessation of fortification, adhered to the established guidelines of the unit, which remained constant throughout the study. MOM was the primary choice for all premature infants upon admission. When MOM was unavailable, preterm formula was made available as an alternative. The hospital does not provide pasteurized human milk; therefore, donor human milk was unavailable.
Enteral feedings commenced as soon as MOM became accessible, and for VLBW infants, milk fortifier was routinely incorporated into their feedings when daily volumes reached 100 ml/kg/day and parenteral nutrition was interrupted. The NICU provided comprehensive support for lactation, educational resources, and equipment for milk expression. A schedule was implemented, allowing mothers to access five hospital-grade breast expression devices conveniently located in a shared lactation room. NICU staff overviewed mothers during expression time. All mothers were thoroughly informed about the significance of MOM for their infants. Trained staff closely supervised the operation of expression devices and the proper handling and storage of expressed milk. Mothers were allowed in the NICU 24/7 but were encouraged to go home during nighttime for proper rest.
When infants complete 34 weeks postmenstrual age, mothers are invited to initiate direct breastfeeding during daytime hours, under health care professionals' guidance, according to clinical stability on a case-to-case basis. During the absence of mothers, when MOM was available, it was administered through bottle. Preterm formulas were offered only when there were no alternatives.
Characteristics of participants
Consecutive new admissions of preterm infants with birth weight ≤1,500 g and/or gestational age ≤30 weeks, absence of MOM contraindications or any major congenital malformation, and survival to discharge were considered eligible for the study. Patients receiving exclusively formula or those who did not have volumes of diet registered at discharge were excluded. A total of 505 infants were eligible. Of those, 46 (9.1%) died and 45 (8.9%) were excluded (Fig. 1). A total of 414 (81.9%) preterm infants completed the study.
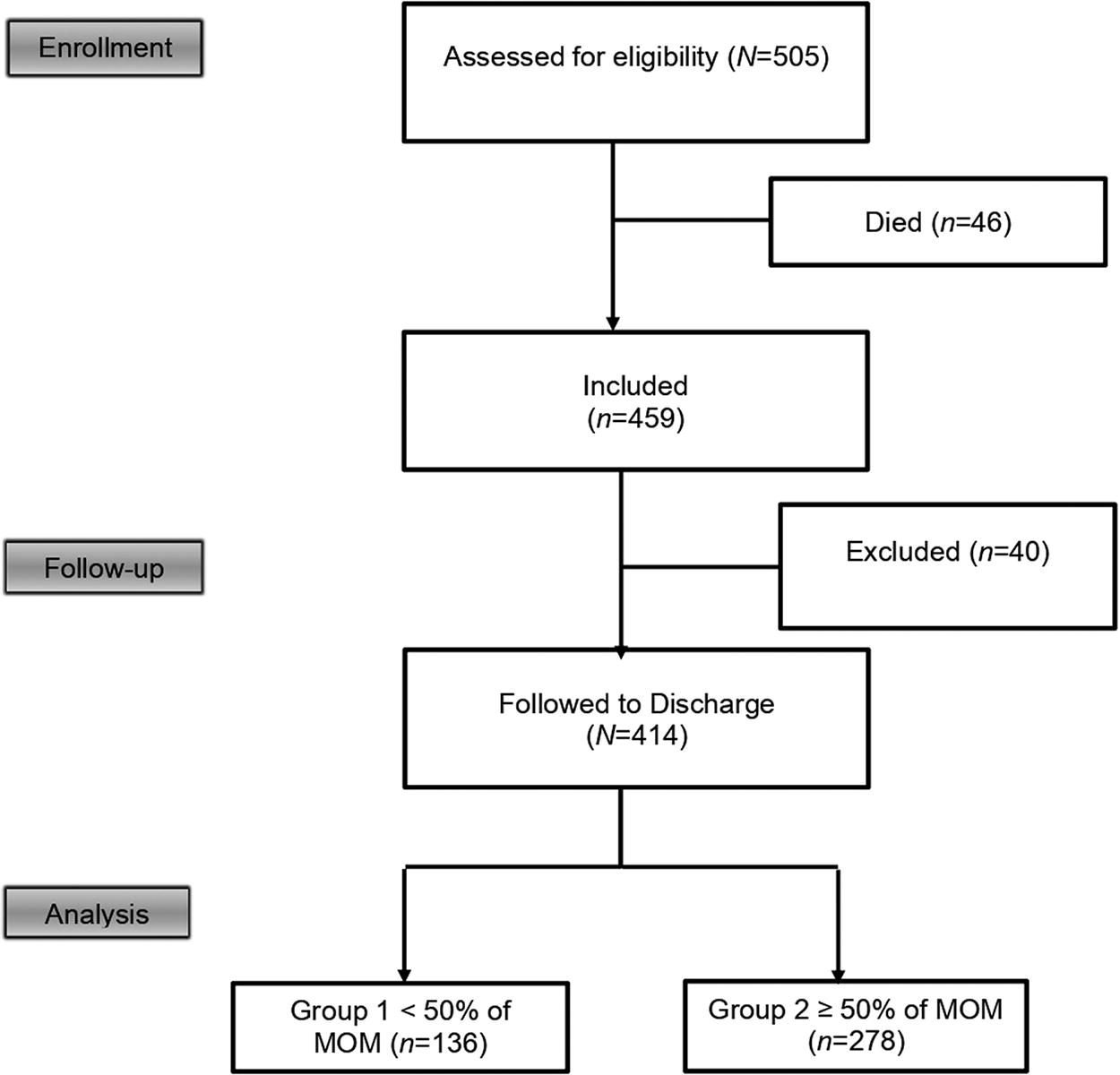
Flowchart of participants.
Measurement
Maternal and infant data included the mother’s education level (in years), mode of delivery, multiples, antenatal steroid administration, gestational age (weeks), birth weight (grams), gender, and Score for Neonatal Acute Physiology with Perinatal Extension (SNAPPE-II). 16 Neonatal morbidities, including necrotizing enterocolitis, intraventricular hemorrhage, and bronchopulmonary dysplasia (BPD), as well as the length of stay (LOS), postmenstrual age, and weight on discharge, were collected. All maternal and infant demographic and medical data were collected following the definitions of the Vermont–Oxford Network database. 17
To define “low volumes of MOM,” we calculated the proportion of MOM volume (expressed in mL/kg/day) in relation to the total volume of milk (MOM + formula) received by the infant on the day of discharge. We used the weight on the day of discharge to calculate the volume of milk received in mL/kg/day.
We considered an infant to have received “low volumes of MOM” if they received less than 50% of their total milk volume as MOM on the day of discharge. The volume of MOM was measured by the nurse’s report, and the total volume of milk received (MOM + formula) was measured by the NICU’s feeding charts. The nursing staff filled the feeding charts, weighed, and recorded the volume of milk given to each infant every day. We chose a cutoff of 50% because infants receiving volumes higher than 50% would be considered to be predominantly breastfed, according to WHO definitions. 1
Data were collected from January 2012 to January 2020. After identifying eligible patients, two neonatologists invited parents or legal guardians to participate in the study. If consent was obtained from parents or legal guardians, clinical data were collected from medical records. All patients included were followed weekly until NICU discharge, and all maternal and infant demographic and medical data were collected prospectively. Participants’ confidentiality was maintained, deidentifying all data collected and using password-protected files.
Data analysis
Software R, version 4.0.3, 18 was used to perform all statistical analyses. All p values < 0.05 were considered statistically significant and used a 95% confidence interval (CI) level. Descriptive statistics (medians, 25th and 75th percentiles, means, standard deviations, counts, and percentages) summarized data. The participant infants were divided into two groups according to the MOM volume they received at discharge (primary outcome). Group 1 consisted of infants who received less than 50% of their total daily volume of MOM, and Group 2 participant infants received ≥50% of their total daily volume of MOM.
Bivariate analyses were conducted to investigate associations with the volume of MOM at discharge, using chi-square, t, and Mann–Whitney tests. We compared antenatal and clinical characteristics between the groups. All p-value analyses were two-tailed. The variables significantly associated with “Low Volumes of MOM” entered the multivariable analysis. Univariate and multivariate relative risk (CI 95%) estimates were obtained from Poisson regression with a robust estimate of variance and controlled by length of hospital stay. The assumption of linearity of regression coefficients for continuous independent variables was satisfied according to the evaluation proposed by Collet D. 19
Results
Characteristics of the sample
In total, 505 VLBW infants were eligible for the study, and 459 (90.9%) survived to discharge. The total number of patients followed is presented in Figure 1.
The mean birth weight was 1108 g (standard deviation [SD] 306), and the median SNAPPE-II was 10 (interquartile [IQR] 0–24). The mean gestational age of all participant infants was 28 weeks (SD 2.8), and all participant mothers received antenatal care. The median LOS was 56 days (IQR 40–80). The antenatal and clinical characteristics of all participant mothers and infants followed to discharge are presented in Table 1.
Antenatal and Clinical Characteristics of Participants Followed to Discharge (n = 414)
BPD, bronchopulmonary dysplasia; GA, gestational age; IVH, intraventricular hemorrhage; MOM, mother’s own milk; NEC, necrotizing enterocolitis; PMA, postmenstrual age; ROP, retinopathy of prematurity.
After dividing patients according to the volume of MOM related to total daily diet volume (n = 414), there were 136 (32.9%) in Group 1 (<50% of MOM) and 278 (67.1%) in Group 2 (≥50% of MOM at discharge). The groups had no difference in the participant mother’s years of education, prenatal characteristics, or the score used to assess clinical gravity (SNAPPE-II). The mean birth weight of participant infants in Group 1 (1115 g, SD 286) was significantly lower than that of Group 2 (1181 g, SD 255), t = −2.29, p = 0.02. Clinical characteristics are described in Table 2.
Comparisons of Categorical Variables Grouped According to the Proportion of MOM Feedings at Discharge (n = 414)
p derived from chi-squared test.
BPD, bronchopulmonary dysplasia; GA, gestational age; IVH, intraventricular hemorrhage; MOM, mother’s own milk; NEC, necrotizing enterocolitis; PMA, postmenstrual age; df, degree of freedom.
Most VLBW infants (n = 278; 67.1%) received more than 50% of their daily enteral diet consisting of MOM at discharge. The median weight at discharge was 2310 g (IQR 2,016–2,679). The median postmenstrual age at discharge was 37 weeks (IQR 36–39). The LOS had a median time of 56 days (IQR 40–80). Lower gestational age, lower birth weight, being born a multiple, developing BPD, and longer LOS were associated with receiving lower volumes of MOM at discharge.
After Poisson regression with a robust estimate of variance, lower volumes of MOM at discharge were associated only with being born a multiple and longer LOS (Table 3).
Univariate and Adjusted Analysis of Factors Associated with Low Proportion (<50%) of MOM at Discharge
p derived from Poisson regression with robust estimate of variance.
BPD, bronchopulmonary dysplasia; BW, birth weight; GA, gestational age; LOS, length of stay; RR, relative risk.
Discussion
In this study, most VLBW infants received a high proportion of MOM volume at hospital discharge. This finding is relevant because no milk bank is available in the NICU where the study was carried out. Therefore, all VLBW participant infants prescribed human milk received only their mother’s milk. This finding shows that mothers can maintain a significant amount of milk production during extended NICU stays, independent of gestational age or morbidities related to preterm birth. After adjustment of confounding variables, being born a multiple and longer LOS were the main risk factors associated with receiving low volumes of MOM at discharge.
Studies on predictive factors of breastfeeding duration in preterm twins have conflicting results. Some studies have found it associated with lower rates and shorter durations.20,21 Others have reported no difference in any breastfeeding rate at discharge.22,23 More recently, a study addressing the association of multiples and breastfeeding rates in VLBW infants at discharge found a statistically significant but small effect on cessation of breastfeeding. 24 Our results show that preterm multiples can be breastfed until discharge but receive a lower MOM volume than single ones.
Our unit has designated health care professionals to support lactating mothers at all times. This fact may have been determinant to the finding that so many mothers in our study succeeded in maintaining their milk provision, even during prolonged hospitalization. These mothers stay long with their infants in the NICU, facing considerable stress. On the other side, longer NICU stays also pose an opportunity to maintain specific and targeted advice by NICU staff and to help support them until transitioning to direct breastfeeding.
Other studies have reported lower gestational age and birth weight as predictors of lower breastfeeding rates.3,25 Romaine et al. 26 described a 49% breastfeeding rate at discharge in a large cohort study, including only VLBW infants. Similar to our findings, longer length of hospital stay increased the risk of VLBW infants receiving fewer volumes of MOM at discharge. Nevertheless, different from their findings, in which sepsis was associated with lower volumes of MOM, in our study, most VLBW infants received predominantly MOM at discharge, independent of their clinical characteristics.
Because our NICU is in a private hospital, all participant mothers had private health insurance. Being able to pay for private insurance is an indicator of high income, different from the reality of most Brazilian people. 27 All mothers in this study had access to quality prenatal care. The NICU offered specific breastfeeding education and equipment, postpartum support, and resources for mothers to stay at the hospital during the daytime. Most mothers had high education levels, which is a factor associated with better jobs that provide access to maternity leave. Brazilian legislation grants 4–6 months of paid maternity leave and facilitates the mother’s presence at the NICU.
Longer LOS was associated with lower volumes of MOM at discharge more frequently, and every 10 days of hospitalization increased the risk of receiving low volumes of MOM by 7%. This percentage might sound like nothing, but one needs to consider that the median hospitalization time was about 60 days. Of note, the extended hospitalization might have more effect on infants with lower gestational age and complications during the neonatal course. One of the most significant challenges mothers of preterm infants face is maintaining lactation for long periods without directly putting the infant at the breast. Extraction devices to express milk are less effective than direct infant stimulation, and longtime device dependence is described as a cause for interrupting milk production. 28
We speculate that understanding which factors are associated with decreasing the volume of MOM during NICU stay may help develop individualized interventions to support these mothers. Even hospitals that do not have access to donor human milk or milk banks can improve MOM volumes offered to this highly vulnerable population. Increasing MOM volumes is a crucial investment, given the growing number of studies showing that human milk has dose-dependent positive effects on reducing preterm-related morbidities.28–30 Evidence shows reductions in health costs when providing MOM because its costs are lower than donor human milk or commercial formulas.31–33 Investing in hospital-branded pumps and NICU lactation specialists would be necessary, but these costs are lower than complications associated with prematurity. This finding is essential for developing or underdeveloped countries like Brazil, especially those with significant differences in private and public health systems.
Also, maternal milk dose appears to be associated with improved neurodevelopmental scores, a finding that has not yet been clearly associated with donor human milk. 34 A recent brain magnetic resonance imaging study also demonstrated these effects to be long-lasting and related to the number of days preterm infants received predominantly breast milk. 35 Although we did not measure the total volume of MOM received, we might hypothesize that preterm infants receiving more than 50% of their daily volume of MOM at discharge probably received high volumes during NICU stay.
This study has some limitations: (1) The study was conducted in a private hospital, and the epidemiological profile may be different from public hospitals and (2) the total volume of MOM received was not measured, in addition to the fact that only the day of hospital discharge was evaluated, a point that could bias the clinical history of study participants. However, to the best of our knowledge, this is the first study that described the factors associated with receiving low volumes of MOM/breastfeeding until discharge in VLBW preterm infants in Brazil.
Although conducted in a private NICU, which may not reflect the reality of the average health services in the country, it showed that it is possible to support mothers and maintain lactation for preterm mothers during hospitalization. Human milk consumption does not demand major financial investments but may result in long-lasting benefits, including reduction of prematurity-related complications and health system resources after hospital discharge. We intend to quantify the duration of breastfeeding after NICU discharge in future studies.
Conclusions
Most VLBW infants were discharged home, receiving predominantly MOM. Each NICU should acknowledge which clinical characteristics of mothers and VLBW infants are associated with difficulties maintaining MOM volumes until discharge. Identifying these factors may help to develop tailored strategies to increase MOM volumes for this vulnerable population. Maternal milk is a low-cost and powerful intervention to improve preterm infants’ outcomes. Understanding the factors associated with low volumes of MOM at discharge can help NICUs acknowledge which clinical characteristics of mothers and VLBW infants are associated with difficulties maintaining MOM volumes until discharge. This information can help NICUs develop strategies to support and encourage breastfeeding and MOM use, which may improve outcomes for VLBW infants.
Footnotes
Acknowledgments
We thank the medical and nursing staff, patients, and their parents at Moinhos de Vento for their cooperation. Thanks to the Research Support Division for their epidemiological and statistics contribution. Everyone’s collaboration was essential for the construction of the summary presented at the 7th International Conference on Nutrition and Growth (Oliveira, M.G. Factors associated with volume of MOM at discharge in VLBW infants—a cohort study. In: 7th International Conference on Nutrition and Growth, 2020, Londres. NGC 2020: Book of Abstracts on Oral Presentations, 2020) and for this article.
Authors’ Contributions
M.G.D.O. and M.F.D.C.S. have contributed to the conception, acquisition, analysis, and interpretation of data and drafted and revised this article. D.D.F.V.V. and J.W. have contributed to the conception and revision of this article. All authors read and approved the final article.
Ethical Approval and Consent to Participate
The protection of human subjects was guaranteed by approval by the Moinhos de Vento Hospital Institutional Ethics Review Board.
Availability of Data and Materials
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was received for this article.