
Abstract
Objective:
To evaluate the impact of acupuncture as part of a traditional Chinese medicine (TCM) treatment plan on lactation and maternal well-being in pump-dependent mothers of hospitalized neonates during the first 30 days after delivery.
Study Design:
This single-center study was conducted in a level IV regional neonatal intensive care unit with access to integrative health services. Sixty-six mothers were prospectively enrolled in two nonparallel groups: (1) Standard lactation support and (2) standard lactation support augmented with acupuncture. Daily pump volumes were documented. Participants completed a quality-of-life (QOL) survey at baseline and neonatal day of life 30. A linear model was constructed, adjusting for increased milk production over time.
Results:
Acupuncture was associated with increased milk production at all time points: Day 10 (p = 0.0002), day 14 (p < 0.0001), day 21 (p < 0.0001), and day 30 (p < 0.0001). Acupuncture was associated with an increase in three of five QOL components: psychological/child's health (p = 0.0006), family/friend relationship (p = 0.0006), and health/functioning (p = 0.02).
Conclusion:
Mothers receiving acupuncture reported enhanced milk supply and improved QOL. The limited sample size restricts the broad applicability of the results; nonetheless, this study paves the way for further research on the advantages of merging Eastern and Western treatments to enhance human lactation.
Introduction
Human milk is uniquely designed to meet infants' nutritional, biological, and immunological needs. Short-term health benefits include reduced risk for respiratory and/or gastrointestinal infection,1,2 otitis media, 2 and sudden infant death syndrome. In low-birth-weight infants, human milk is associated with lower risks of retinopathy of prematurity, 3 necrotizing enterocolitis,2,4,5 and reduced incidence of late-onset sepsis. 6 Long-term health benefits for infants include improved neurodevelopmental outcomes7–9 and lower rates of obesity and diabetes. 10 Breastfeeding also provides positive health outcomes for mothers, including reduced risks of breast and ovarian cancer11,12 and a lower incidence of hypertension, diabetes, and cardiovascular disease.12,13 Given its impact on the health outcomes of both mothers and infants, breastfeeding significantly influences health care costs. 12 For these reasons, the American Academy of Pediatrics, 14 the World Health Organization, 15 and the American College of Obstetricians and Gynecologists 16 recommend exclusive breastfeeding for the first 6 months of life.
Although the advantages of human milk are widely acknowledged, families frequently face difficulties in providing it for their infants. This struggle is particularly pronounced for parents of infants in the neonatal intensive care unit (NICU). 18 Complex barriers to lactogenesis in the NICU include separation of mother and infant, illness, poor technique, and maternal stress and anxiety.19–22 Strategies to optimize lactation involve collaborative multidisciplinary efforts, incorporating physical and emotional approaches. These include proper latch and positioning, promoting skin-to-skin contact, encouraging early and frequent milk expression, and maternal stress reduction.21–23 The Academy of Breastfeeding Medicine advises caution when prescribing pharmaceutical galactagogues due to possible side effects and advocates for nonpharmacologic methods when possible. 24
Acupuncture, an ancient practice rooted in traditional Chinese medicine (TCM), is increasingly recognized as a complementary therapy alongside conventional Western medicine. Acupuncture targets specific points on the body to trigger natural healing mechanisms, encourage relaxation, and reestablish equilibrium. 24 It can thus reduce stress levels and alleviate symptoms associated with various health conditions, such as pain, insomnia, migraines, and anxiety. 25 In TCM, the body is an interconnected system where various organs, meridians (energy pathways), and processes work together to maintain health. Imbalances or disruptions in the flow of Qi (vital energy/life force) through these meridians are believed to lead to illness. 24 TCM seeks to identify and address the underlying causes of these imbalances. Acupoints are precise targets located at superficial loci along these meridians, which can be manipulated through interventions such as acupuncture to address Qi excess or deficiency. 25
Premature birth stresses the mother's body, potentially obstructing the flow of Qi and Xue (blood), disrupting the production of prolactin and oxytocin, which can hinder milk production.25–27 The emotional stress of having a critically ill newborn further depletes the mother of the energy needed to create milk. Research has been conducted on the acupoint combination of Shao Ze (SI 1), Zusanli (ST 36), Dan Zhong (R 17), and Taichong (L 3) to enhance lactation, but the clinical results vary.28–30 A 2021 systematic review of international research concludes that, even with varied outcomes, acupuncture's ease of use, cost-effectiveness, and absence of side effects make it a promising method to enhance breast milk production. 31
The primary aim of this study was to investigate the efficacy of acupuncture in enhancing human milk production in mothers of hospitalized infants. The intended outcome was reaching a full milk volume of ∼750 mL daily, measured on days of life 14 and 30. An exploratory outcome was the impact of acupuncture on maternal quality of life (QOL). It was hypothesized that mothers receiving acupuncture would produce more milk and report enhanced QOL than those receiving standard lactation support.
Methods
Study design
This study was conducted at a children's hospital in the United States with a level IV regional NICU and access to integrative health services, including licensed TCM practitioners. Ethical approval was obtained from the hospital's institutional review board.
A nonequivalent group design was used to enroll two nonparallel treatment groups. Group A served as the control group and received the current NICU standard of care to optimize lactation. Standard of care included multidisciplinary support and lactation consultation, including a pump session with education on hand expression, access to a hospital-grade pump, and encouragement to pump at least eight times per day until breasts are empty. The experimental group (Group B) received the standard of care plus acupuncture up to three times per week over a 4-week period performed by a licensed acupuncturist. Enrollment in the treatment groups was separated by 1 month. By separating the enrollment of experimental and control groups by 30 days, researchers aimed to reduce the likelihood of communication among participating mothers, which could potentially bias study outcomes.
Study population
A convenience sample of mothers with newborns admitted to the hospital's NICU was recruited. NICU mothers were included if they were ≥18 years of age and at high risk for lactation insufficiency due to anticipated long-term pump dependency with a desire to provide human milk for their infant. Mothers were excluded if they had a history of any of the following: Could not read English; breast surgery; substance abuse; diagnosed with a clotting disorder or hemorrhagic disease; or any other contraindication to breastfeeding, such as galactosemia or human immunodeficiency virus. A power analysis estimated that a sample of 80 participants was needed to detect a significant difference in milk supply.
Group A (n = 35) was enrolled from January 2020 through March 2021 and received the current standard of care to support lactation. Group B (n = 31) was enrolled from May 2021 through February 2022 and received the standard of care supplemented with acupuncture. The difference in timeframes across the two treatment groups was attributed to disruptions caused by the COVID-19 pandemic. Lactation consultants (IBCLCs) screened potential participants for eligibility. Eligible mothers were approached for informed consent within 96 hours and enrolled within 120 hours after infant birth.
Acupuncture treatments
Participants in Group B received treatment from a licensed acupuncturist at an offsite clinic (maximum three sessions per week) within the infant's first 30 days of life. Four standard lactation acupoints (Table 1) were used, with retention times of 30 − 40 minutes. The acupuncture needles utilized were Seirin brand, single use, and sterilized. The sizes were J type 0.16 × 30 mm, 0.18 × 40 mm, 0.20 × 30 mm, and D type 0.16 × 15 mm.
Acupuncture Points Used
Qi = vital energy/life force.
Measurement
Maternal and neonatal demographic and health characteristics
Maternal age, race, ethnicity, education, and marital status were collected to ensure a multifaceted understanding of acupuncture's impact on lactation, considering the varied experiences and backgrounds of participants. Maternal health characteristics were assessed, including pregnancy and birthing history, previous experience with breastfeeding, medical history, and medications. Characteristics of the newborns, such as diagnoses, gestational age, and weight at birth, were also evaluated.
Daily pump logs
Milk volumes were recorded daily using a pump log. To estimate the amount of milk consumed, infants were weighed before and after each breastfeeding session. Infants discharged before reaching 30 days of life were given a breastfeeding scale to enable precise evaluations at home.
Maternal QOL
The Maternal Postpartum Quality of Life (MAPP-QOL) was utilized to evaluate maternal QOL. This validated self-assessment questionnaire measures the physical, emotional, psychological, and social health of mothers.37,38 The tool consists of two parts (satisfaction and importance) and was administered in paper form. In Part 1, mothers were asked to describe how satisfied they are across different aspects of their life (i.e., health, amount of sleep, pain) using a Likert scale ranging from “Very Dissatisfied” to “Very Satisfied.”
In Part 2, mothers were asked to describe how important these areas of life were to them using a Likert scale of “Very Unimportant” to “Very Important.” Scores were calculated by pairing each satisfaction response with its related importance rating. These scores depict not just satisfaction but also personal priorities, providing a more accurate reflection of QOL. Results were analyzed within the context of five QOL domains: (1) Psychological health and child's health, (2) socioeconomic status, (3) family and friend relationships, (4) spousal relationships, and (5) health and functioning. 32
Statistical analysis
The biostatistician was blinded to group assignment to reduce potential bias during analysis. Descriptive statistics were reported on the distributions of categorical and continuous variables to identify potential confounders. Data were analyzed for associations between acupuncture and milk production or maternal QOL and between milk volume and QOL. Fisher's exact test was used to detect differences in proportions of categorical variables stratified by treatment status. Shapiro's test of normality was applied to continuous variables. The distribution of expressed human milk and QOL measurements significantly differed from the normal distribution (p < 0.05). To address the non-Gaussian data distribution, the Wilcoxon rank sum test was selected to test for differences in the distribution of QOL and milk expression stratified by treatment status.
To evaluate the effect of acupuncture on milk supply, a Wilcoxon rank sum test was used to compare the distribution of milk supply between groups at various time points. The two primary comparisons were infant days of life 14 and 30. The other time points (days of life 5, 10, and 21) were secondary.
In addition to bivariate inferential statistics, linear regression models were constructed to explore associations between acupuncture and milk production and acupuncture and maternal QOL, while adjusting for confounding variables. The model predicting milk production was adjusted for study time point, infant weight, prescribed steroids, and treatment status. Models predicting each QOL component were adjusted for maternal age, education, marital status, parity, infant birth weight, and whether the infant had a respiratory diagnosis. All linear model results were reported on intercept and variable estimates, the 95% confidence interval surrounding each estimate, and the corresponding p-value. Statistical analyses were performed using R statistical programming language version 4.1.3. 33
Dose–response relationship
To examine the impact of acupuncture on maternal QOL, the 30-day pre-post MAPP-QOL change was compared between groups. The association between acupuncture dose and treatment response was assessed by comparing the distribution of QOL improvement in mothers who received less than the median number of treatments or greater than or equal to the median number of treatments. Distributions were compared using a two-sample Wilcoxon rank sum test.
Results
Of the 66 subjects enrolled, 55 completed all study procedures and were included in the analysis (Fig. 1). Demographic characteristics of mothers and infants are presented in Table 2. When stratifying by treatment status, there was a significant difference in the proportion of non-White participants receiving standard of care (26.3%) compared to those receiving acupuncture (11.5%). No other variable had significant differences in distribution when stratifying by treatment.
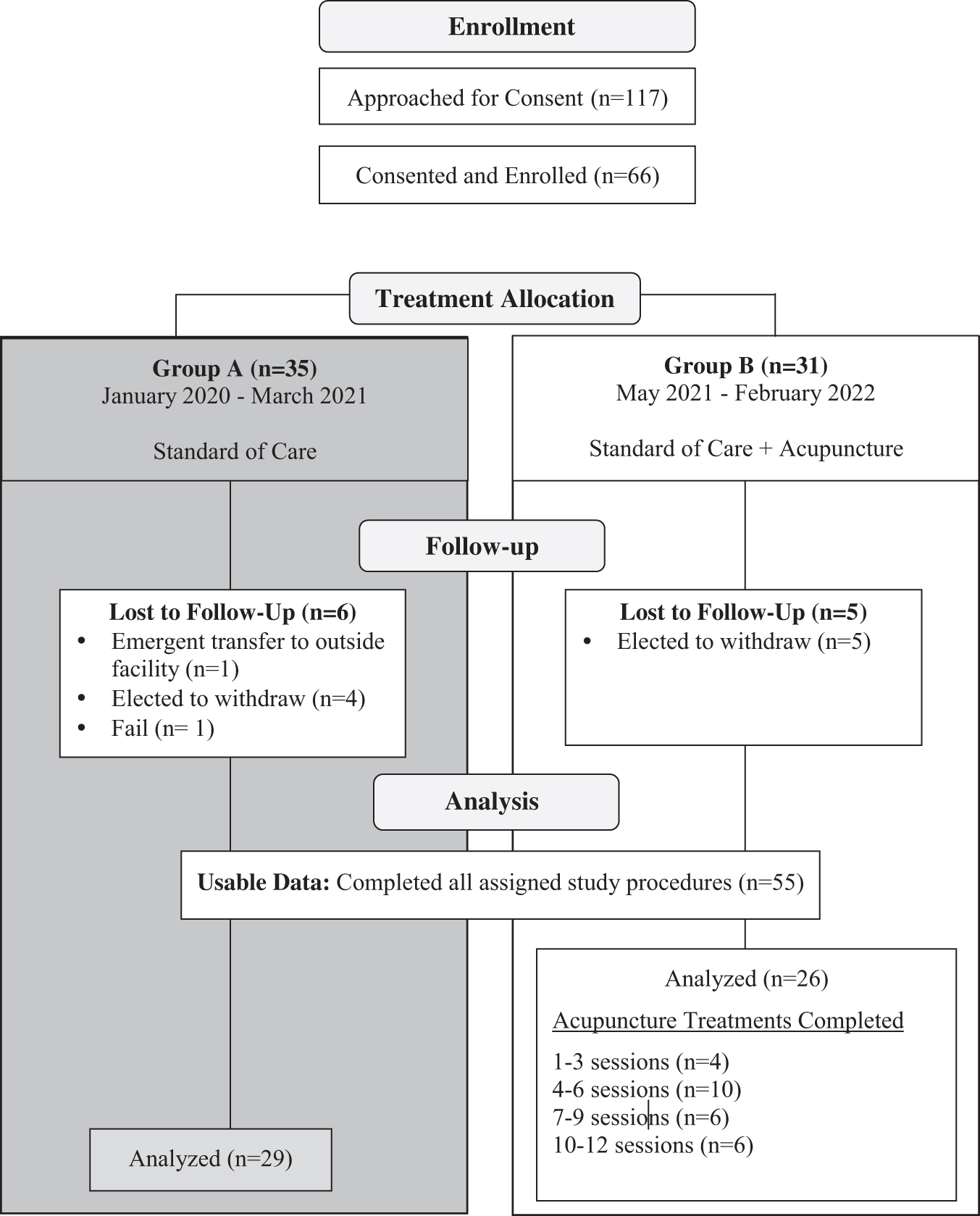
Flow chart of participant enrollment, treatment allocation, follow-up, and analysis. This flow chart illustrates the progression of participants through the study phases. It begins with the initial enrollment numbers, detailing the total number of participants approached for consent and the number of consented and enrolled. The next section of the chart shows the allocation of subjects to different treatment groups. The number and reasons for patients lost to follow-up are then detailed for both groups. The
Distribution of Maternal and Infant Demographic and Clinical Characteristics Across Groups
Calculation of the proportional increase in milk production was made by taking the median output from group B divided by the median output of group A at each time point of human milk production measurement. Median human milk production was greater in Group B compared to Group A across all time points. While conducting bivariate analysis of possible confounders, we found that mothers who received steroids at baseline had significantly less milk production than mothers who did not (median volume 472 mL versus 900 mL, respectively, p = 0.5) at 30 days (Fig. 2). Baseline steroid use was associated with a 152.5 mL estimated decrease in milk production (p = 0.03).

Distribution of human milk production across study time points. The
Steroid use impacted milk production in both groups, underscoring the need to adjust for steroid use when testing the association between acupuncture and milk production. The largest difference in distributions is between treatment and control groups that do not receive steroids, providing evidence that the observed effect is not the result of confounding by steroid prescription.
A linear model was constructed to predict milk production (Table 3). The regression model was constructed to adjust for bias that was evident based upon statistical and clinical interpretation of descriptive and bivariate inferential statistics. Data were adjusted for a marginal association observed between birth weight and milk production on day 5 (p = 0.05). All time points were associated with an increase in milk production compared to baseline (all p ≤ 0.0002), but mothers in Group B showed an additional increase of 326 mL, compared to mothers in Group A (p < 0.0001). Birth weight <1,700 g was associated with an estimated increase in milk production (277.1, 184.6–468, p < 0.0001) after adjustment for an interaction effect between birth weight and treatment (−474, −711 to −237.5, p = 0.0001) (Fig. 2 and Table 3).
Time Point-Specific Linear Models Predicting Human Milk Production (mL)
The distributions of maternal QOL components and total scores were also examined. The psychological health and child's health component of QOL increased in Group B, but decreased in Group A (mean 1.3 versus −1.8, respectively, p = 0.02). The family/friend relationship distribution was found to be significantly higher when comparing acupuncture (median difference of 0 and mean of −0.22) to the standard of care (median difference of 0.9 and mean of −1.7). No statistical significance was found in socioeconomic status, spousal relationship, and health and functioning.
Acupuncture was associated with improvement in maternal QOL: Psychological and infant health (4.4 points, p = 0.0006), health and functioning (3.2 points, p = 0.02), and family and friend relationships (3.4, p = 0.0006). The estimates produced for different treatment groups were made after adjustment for covariates that produced bias. (Table 3, Fig. 3). No other covariate within the models met criteria for statistical significance. The fact that there is no drop in the QOL measure for family and friends for Group B, but there is a drop for Group A provides evidence for a protective effect for this measure of QOL in Group B.

Distribution of QOL components between the treatment groups. The box plot on the
After mothers were stratified by acupuncture treatment and by health and functioning, the relationship between the number of acupuncture sessions and human milk production was examined. An association was found between QOL and milk production in the last two time points for those who received acupuncture, but not for those who received standard of care (p = 0.04 for both time points). There was a significant increase (p = 0.03) in maternal QOL among those receiving greater than median number of sessions (7). This provides evidence for an increase in QOL in those receiving more sessions and evidence of a link between milk production and health and functioning in those receiving acupuncture.
Discussion
Human milk provides a multitude of well-established benefits. Despite strong recommendations from health care organizations and professionals, the exclusive breastfeeding rate in the United States during the first 6 months of life remains relatively low at ∼25%. 34 Pediatricians play a vital role in promoting breastfeeding by collaborating with IBCLCs and nurses to encourage early, frequent milk expression. 17
While misconceptions about acupuncture remain, the Joint Commission on Accreditation of Healthcare Organizations has set standards that govern a well-defined system. 35 Training and credentialing of acupuncture practitioners are crucial to integrating this technique into medical practice. 36 Acupuncture is becoming increasingly popular, with over 37,000 licensed acupuncturists and over 10,000 medical acupuncturists nationwide. 37 Educational standards have been established, and a national credentialing agency is now recognized by major acupuncture organizations. Most states offer licensure or registration for those practicing acupuncture and a growing number of insurance providers provide coverage for acupuncture treatments for various health conditions. 38 Broadening this coverage would eliminate monetary obstacles, promoting more equitable access to these services for diverse patient groups, including breastfeeding mothers.
The observed correlation between QOL and milk production among participants who underwent acupuncture treatments, as opposed to standard care, at the last two time points (p = 0.04 for both time points) suggests an intriguing possibility of acupuncture offering an independent advantage for maternal well-being. This finding implies that the impact of acupuncture on maternal mental health might extend beyond the influence of improved milk production, hinting at an additional, distinct benefit of acupuncture interventions.
The relationship between maternal stress and breastfeeding is complex and likely bidirectional. While the exact physiological mechanisms are not fully understood, there is evidence to suggest that maternal stress impairs lactation outcomes, and conversely, positive breastfeeding experiences can have a calming effect on mothers. 23 Elevated stress levels can interfere with the release of oxytocin, a hormone essential for milk letdown and production. Stress hormones, such as cortisol, can inhibit the release of oxytocin, leading to difficulty with lactation and lactogenesis. In addition, stress can contribute to physical tension and discomfort, further impeding breastfeeding. 23
On the other hand, breastfeeding stimulates the release of oxytocin, which promotes relaxation, feelings of well-being, and a sense of calm in both mother and baby. 23 It is important to note that individual responses to stress and breastfeeding can vary. Some mothers may find breastfeeding a source of comfort, while others may feel additional pressure or stress related to breastfeeding challenges. Further research is needed to understand the bidirectional relationship between maternal stress and breastfeeding, including the underlying mechanisms.
The finding that maternal steroid exposure is associated with decreased milk supply aligns with previous observations regarding steroids' impacts on human milk production. 39 Steroid-treated mothers are more likely to have an earlier gestational age, as steroids aid fetal lung development in preterm births. Earlier gestational age is also associated with lower milk supply due to immature maternal breast development.
Our findings highlight the dual benefits of acupuncture in (1) increasing milk production and (2) improving QOL for mothers in the NICU. The information presented should compel physicians to consider a broader range of approaches to support lactogenesis during hospitalization. However, it is important to approach the integration of acupuncture into the multidisciplinary approach with caution. The health care team must collaborate to ensure safety monitoring and evidence-based application of acupuncture in the NICU to provide individualized care and support.
Limitations
Acupuncture studies often face various limitations, and one of the major challenges is the difficulty in establishing an appropriate control group. It is crucial to recognize alternative causal explanations for the observed effect of acupuncture on milk production and QOL. The self-selection process could have introduced a positive bias among the participants, as they may have joined the study due to their pre-existing positive attitudes or beliefs regarding holistic and integrative treatment modalities. Participants who are willing to travel to an offsite clinic might be more committed or motivated toward the treatment, which could influence adherence to treatment protocols and potentially skew results.
Traveling to an offsite clinic might enhance a placebo effect because participants might perceive treatments at these locations as more “special” or “effective.” Furthermore, the unprecedented stress of the pandemic may have affected breastfeeding patterns, well-being, and human milk production. Initially, this study intended to recruit more participants to achieve a statistical power of 85% to detect a 20% difference between groups. Due to time constraints caused by the pandemic, enrollment was discontinued before the desired participant count was reached. Interestingly, the study population was sufficient to detect a significant clinical effect. The length of the study limited the ability to see if acupuncture beyond 1 month would provide additional benefit compared to the control group.
Non-English-speaking mothers were excluded from the study due to the limitations of the MAPP-QOL instrument, which may have introduced bias and limited the generalizability of the findings. When stratifying by treatment status, the percentage of non-White participants who received standard of care (31.0%) was significantly greater than the percentage who received acupuncture (11.5%). Therefore, racial group variables were not included in the linear regression model. In addition, Group A had more mothers who were of lower education and primigravida. This could be addressed in future studies with larger samples and more robust experimental designs that block confounders within experiment and control groups.
While these limitations threaten the study's internal validity, our results serve as an impetus for future research. Larger samples will improve estimates of the effect of acupuncture on human milk production and maternal QOL.
Conclusions
Human milk is tailored for infant needs, but mothers with hospitalized newborns often face challenges in producing an adequate supply. While acupuncture is a standard therapy in many cultures, it is still emerging in Western medicine. Preliminary studies, including ours, suggest that acupuncture can enhance lactation and maternal QOL. Although our research had a limited sample size, findings validate the potential benefits of combining Eastern and Western methods to enhance maternal and infant well-being.
Footnotes
Acknowledgments
The authors express appreciation to Dr. Terrie Inder, CHOC, for her review of the article; Dr. Rachel Davis, CHOC, for editorial support; the licensed acupuncturists at Open Mind Modalities; the IBCLCs and NICU at CHOC for their participation in this study; West Coast University; and the Walden W. and Jean Young Shaw Foundation for their continued support of nursing research and TCM at CHOC.
Authors' Contributions
C.B.-F.: Conceptualization, methodology, investigation, writing—review and editing, project administration, and funding acquisition; J.H.: Conceptualization, methodology, resources, writing—original draft, visualization, supervision, project administration, and funding acquisition; R.M.: Conceptualization, methodology, investigation, resources, and writing—review and editing; M.H.: Methodology, investigation, and writing—review and editing; J.S.: Conceptualization, methodology, formal analysis, data curation, writing—original draft, and visualization; S.S.: Investigation and writing—review and editing; C.B.: Conceptualization, writing—review and editing, visualization, and supervision. All authors approved the final article as submitted and agreed to be accountable for all aspects of the work.
Disclosure Statement
The authors of this publication cite no financial disclosure related to the conduct of this study or preparation of this article.
Funding Information
This study was graciously supported by One Wish Grants, a program presented by the CHOC Foundation and its Board of Directors. One Wish Grants had no role in the design and conduct of the study.