
Abstract
Background:
Breastfeeding and Lactation Medicine (BFLM) programs at academic medical centers are uncommon but expanding. Our academic medical center, with a long legacy of leadership in BFLM, established a BFLM program in 2016 and launched a dedicated division in 2022.
Objectives:
To describe the strategy, services, measures, and challenges facing our multidisciplinary academic BFLM program in its first 8 years.
Methods:
To support the development of the Division, we proved clinical need, built capacity, and determined key outcomes. We organized partnerships across clinical and research programs and developed leadership and reporting structures. These services and programs coalesced to form the first Division of Breastfeeding and Lactation Medicine in 2022, including multiple specialties (pediatrics, obstetrics, family medicine, nutrition research, toxicology, public health, dentistry) and provider types (nursing, lactation consultants, physicians, midwife, nurse practitioner, PhD, dentist). Challenges included variable buy-in, staff training, reimbursement, medical record infrastructure, and data reports. Challenges to research included funding and clinical integration.
Conclusion:
A multidisciplinary BFLM Division at a large academic medical center was formed, spanning our clinical, research, and educational missions. Integration into traditional academic structures brings essential resources, enables participation in medical center leadership, and promotes the sustainability of divisional activities.
Background
Breastfeeding and Lactation Medicine (BFLM) programs at academic medical centers are uncommon but expanding. A review of medical directors of such programs in 2016 found that 75% of the 32 positions had been created in the preceding 10 years. 1 Such programs support lactation by providing expertise for complex cases, directing quality improvement, training health care providers, and expanding institutional research. The work of Dr. Ruth Lawrence provided a strong foundation in the science and clinical care of breastfeeding and lactation at the University of Rochester. Building on this, our hospital system at the University of Rochester initiated a formal BFLM program in 2016, which was institutionalized as a stand-alone division under the Department of Pediatrics in 2022. To our knowledge, this is the first and only academic division dedicated exclusively to BFLM. The Division of Breast Health and Breastfeeding Medicine under the Department of Obstetrics and Gynecology (OBGYN) at State University of New York Upstate in Syracuse, NY is the only other division that encompasses BFLM work in its mission.
We seek here to describe the development of this division across clinical, research, and educational settings, with a special focus on our history, strategy, and challenges.
Methods
Settings
The University of Rochester Medical Center is an academic not-for-profit institution in western New York that operates as its regional perinatal center. It includes a Level IV neonatal intensive care unit (NICU) with 68 beds, a Maternal Fetal Medicine program, and just under 3,000 deliveries per year. 2 The BFLM Division also serves the broader community through local and regional referrals and telehealth. Rochester, NY, has a population of just over 210,0003 with approximately 10,000 births per year. Of note, Rochester suffers from a history of redlining and economic recession, has a 29.3% poverty rate, 3 and suffers from significant disparities in health outcomes by race and ethnicity. It was therefore central to our program to ensure equal access to care, train our staff in equity skills, reach out to community partners, develop research that is congruent with community goals and needs, and track our outcomes by patient race/ethnicity.
History
The Division of BFLM at the University of Rochester owes its founding to the energy and expertise of Dr. Ruth Lawrence, Professor Emerita of Pediatrics. Dr. Lawrence was a pioneer for women in medicine, due to both her stalwart refusal to succumb to obstacles and her innovation in the care of mothers and children. She graduated from the University of Rochester School of Medicine and Dentistry in 1949 and pursued a residency at the Yale New Haven Hospital. At Yale, she was inspired by the work of her attending physician, Dr. Edith Banfield Jackson (“Edie” Jackson), who brought “rooming-in” to the delivery rooms of the United States after studying psychoanalysis in Austria under Dr. Sigmund Freud. 4 Dr. Lawrence was the first woman to graduate from Yale residency and the first to then be hired as medical faculty at the University of Rochester. As a neonatologist and mother of nine, she developed a passion for the benefits of breastfeeding as a unique gift to the next generation. Human lactation had suffered from considerable neglect by the medical community and was just beginning to be studied. A traveling file cabinet on wheels allowed her to collect and distribute articles to reference when educating fellow physicians. This file later developed into her classical textbook, “Breastfeeding: A Guide for the Medical Profession,” now in its 9th Edition. 5 As director of one of the first Poison Control Centers, Dr. Lawrence saw an opportunity to provide access to breastfeeding expertise by telephone and, in 1981, founded the National Lactation Study Center to meet this need. Her collaborative research endeavors furthered our understanding of breastfeeding, in topics ranging from the investigation of best practices in breastfeeding support to the passage of vitamin D into breast milk.6,7 Dr. Lawrence trained many physicians in the care of breastfeeding families, and several of her former students now occupy senior positions across the University, improving the institutional understanding of the importance of breastfeeding and human milk. She established a formal fellowship in BFLM before retiring in 2019. Her last fellow now serves as Division Chief and carries on her legacy.
Strategy
In the United States, academic medical centers function as sites of training, innovation, and mission-based sustainability for core medical needs that may be unmet in a reimbursement-based model. In doing so, they support specialized medical fields, while also serving as an essential component of the health care safety net in a nation lacking universal health insurance and universal access to primary care. Clinical care in academic medical centers is divided into core departments (e.g., medicine, pediatrics, OBGYN), which are then subdivided into divisions representing subspecialties (e.g., adult or pediatric infectious disease, rheumatology, endocrinology). Collections of faculty and staff may collaborate on projects surrounding a particular disease state or population need, such as a diabetes management program nestled within endocrinology. This is a common organizational structure for breastfeeding and lactation programming. Without designation as a division, however, these programs are subject to dissolution in times of low reimbursement or leadership change. In a strategic pursuit of sustainability, we therefore developed the infrastructure to transition our program into a division. Moreover, divisions participate in the leadership structures and decision-making of their respective departments, affording opportunities to guide the medical mission and highlight the needs of patients, faculty, and learners at a higher level and University wide. The evolution of our division was shaped in parallel with the clinical, educational, and research priorities of the University and the wider community.
Mission, values, plans, and reach
Being responsive to the needs of the community has been critical to the mission of the division, and we work with community partners for goal setting, program evaluation, at events, and in our teaching. Our Division’s faculty represent a range of specialties, including pediatrics, obstetrics, family medicine, nutrition research, toxicology, public health, and dentistry, alongside diverse provider types such as nurses, lactation consultants, physicians, midwives, nurse practitioners, PhDs, and dentists. We believe that this multidisciplinary approach is essential to capture the complexity of lactation physiology and to bring the necessary expertise to bridge the gaps in both scientific knowledge and care provision.
Our mission statement, detailed in Table 1, was designed to align with the core values of the University, including equity, leadership, integrity, openness, respect, and accountability, while also reflecting the visions of Golisano and Strong Memorial Hospitals. By doing this, we embedded our efforts within the broader framework of the University and provide patients with a clear expectation of the care they will receive from us. Most recently, a strategic planning process has allowed us to gain input from 23 internal and community partners, which enabled us to create a community-responsive 5-year vision and plan. Figure 1 demonstrates our multiple service lines and efforts across foundational priority areas such as clinical, educational, research, and community. Current goals include expanding telelactation services, creating a new clinic location in a low resource area, seeking grants to promote research (below) and successful care management programs, and improving our access to high-quality breastfeeding data across the community. A website, video series, and social media marketing have enhanced the transparency of our broader mission and expanded our reach.
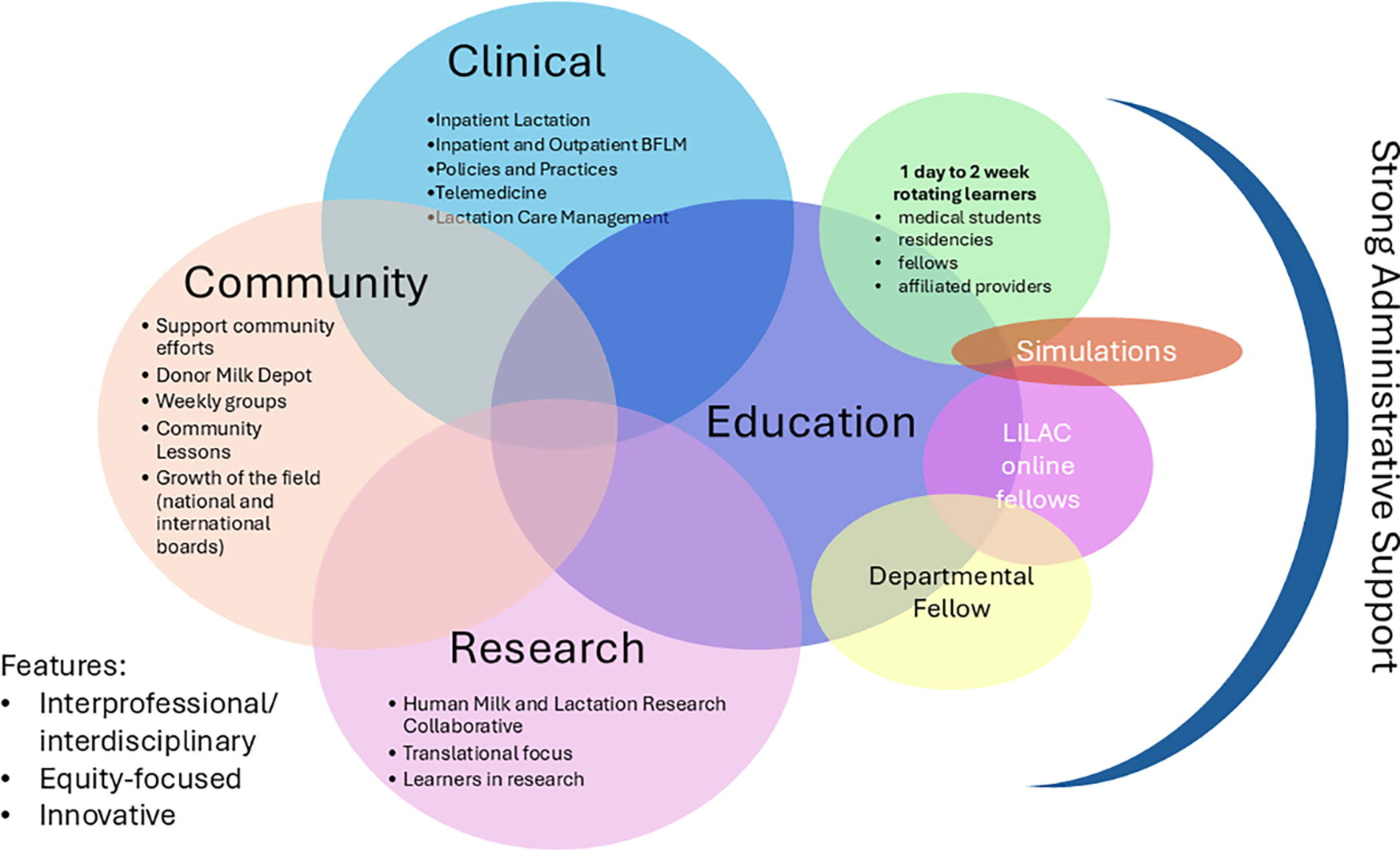
Service Lines and Efforts of the Division of Breastfeeding and Lactation Medicine Across Priority Areas: Clinical, Educational, Research, and Community.
Mission Statement of the Division of Breastfeeding and Lactation Medicine, Developed to Align with University Values and Provide Patients with Expectations for Care
Outcomes
Collecting outcomes across all divisional pillars (clinical, research, and education) is critical to justify and sustain a medical division, particularly in a new field. Routine monitoring ensures that current programming is successful and allows for rapid and responsive growth. Clinically, we found it important to collect both process outcomes (numbers of consults) and health outcomes (breastfeeding rates). Given historical and current inequities in breastfeeding and lactation outcomes, it is critical to analyze and regularly review these measures across sociodemographic indicators, especially race/ethnicity and geography. This ensures that efforts reach patients equitably and that improvement efforts narrow, rather than widen, disparities in outcomes. For instance, preliminary analysis of our growing telemedicine program has demonstrated improved access to care by race and rural geography, a key goal of that program. Data collection, build of our data infrastructure, and use of the medical record are described in Supplementary Data S1.
Revenue
An important consideration in the development of a division is providing reimbursement and working to improve income to cover clinical, educational, and administrative costs. Research is funded by grants and is discussed below. While inpatient services do not bill for lactation consultants, BFLM providers are able to generate inpatient and outpatient bills to insurance companies for all parts of the lactating family who require medical care (pregnant people, mothers, lactating parents, infants, and children). Outpatient lactation consultants are able to bill for either the mother/lactating parent or child as a registered nurse/international board certified lactation consultant (RN/IBCLC) in New York State. Group services are poorly reimbursed, and there is no reimbursement for non-RN IBCLCs. COVID-era telemedicine reimbursement rules are still in effect in New York State, allowing for remote service access by patients who are geographically distant or who suffer transportation difficulties. If a patient lacks insurance coverage, we refer the patient to payment services who assist with enrollment.
We suffer from the same percentage of denials as other divisions in pediatrics, although reimbursement rates are generally low in this field. Moreover, changing rules around telemedicine prevent reimbursement by some insurers for RNs. It is therefore a difficult landscape from which to build robust programming, and much-needed expansion of services requires departmental support, collaboration with insurers, accountable health organizations, and grant funding. We have found that maintaining partnerships across the University is an invaluable aspect of sustainability, and we continue to receive considerable support from partners in OBGYN and Neonatology.
Administration
Originally founded as a program with a medical director in 2016, across Neonatology (NICU), Obstetrics (Maternal Fetal Medicine), and General Pediatrics, the first clinic was opened under the auspices of OBGYN. In year 5, when the Division was formalized, the Medical Director became Division Chief and the Lactation Coordinator became a Nurse Manager of Lactation. An Assistant Medical Director (fellowship-trained CNM) was appointed to run clinical operations in the outpatient setting and as a core member of the clinical leadership team. Although the Division is nested under the Department of Pediatrics, we work very closely with the Department of OBGYN to ensure consistent and streamlined provision of care across the hospital system. Table 2 describes the total clinical and administrative full-time equivalents (FTEs) in our divisional and lactation staff.
Breastfeeding and Lactation Medicine and Lactation Consultant Staff and Full Time Equivalents
FTE, full-time equivalent, a unit of measurement corresponding to the workload of individuals in an institution. 1.0 FTE corresponds to the workload of one full-time individual in a role-specific work day.
Division funded refers to support from clinical revenue, as well as departmental support, shared between the Departments of Pediatrics and OBGYN.
NA, not applicable.
Clinical Services
The identification of patient needs and development of clinical services was central to the foundation of our Division. Clinical services form the backbone of an academic division, to serve patients (the primary goal of a health system), to inform academic work (education, research, quality), and to generate revenue. We sought advice from an ad hoc community advisory board, including local services supporting peripartum families, especially those serving low-income populations. This group highlighted the need for outpatient insurance-covered lactation services and recommended that the University start an outpatient clinic. Meanwhile, inpatient lactation consultants suffered from a lack of medical support in challenging cases, difficulties interfacing with providers with varying levels of lactation knowledge, and patients who struggled with conflicting advice. We therefore sought to build clinical services in the outpatient and inpatient settings and to sustain the preexisting Lactation Study Center to offer remote support. Later efforts included incorporating telemedicine services and partnering with local primary care clinics, which are building lactation care management programs. Key interventions over time are described in Figure 2.

Key Interventions Leading to the Growth of the Breastfeeding and Lactation Medicine Division Over Time. Med Director, Medical Director; PT, Part Time; FT, Full Time; NP, Nurse Practitioner; BFLM, Breastfeeding and Lactation Medicine.
BFLM services
The outpatient BFLM clinic was founded in year 1 in response to community partners’ expressed need for an outpatient lactation service that accepted insurance coverage. We gradually increased from two half-day clinical sessions across 3 sites embedded in pediatric and obstetric practices to an independent 5 day per week practice with support groups. In year 7, an expanded and robust telemedicine program with self-scheduling and after-hours care was developed.
To increase access and maximize clinical care, most outpatient sessions are staffed by a provider (physician, certified nurse-midwife, or nurse practitioner [NP]) and two IBCLCs, who may or may not also be RNs. Each patient is seen first by an IBCLC, who completes a history, assesses goals, provides latch assessment with maximization of positioning, measures milk transfer, assesses pump/expression, and provides education and support for the breastfeeding/lactating family. The BFLM provider uses this information to complete any medical or differential diagnosis-based history and medication review, assesses vital signs and growth parameters (growth of infants/children and blood pressure of mothers/lactating parents), completes a physical examination of all parts of the breastfeeding/lactation relationship, and diagnoses and treats any medical concerns. Therefore, the scopes of practice of BFLM providers and IBCLCs overlap but differ.
IBCLCs provide patient-centered lactation education, support of normal lactation (including positioning and expression/pumping), identification of barriers to lactation, assessment and management of lactation difficulties, and support medical teams in accessing resources on difficulties (e.g., medication review). BFLM providers diagnose and treat any medical concerns that arise in the breastfeeding/lactation relationship as follows: the mother/lactating parent and the child/children. We also offer lactation-only visits for families who have less complex concerns or require follow-up for nonmedical reasons (trial of lactation assistive devices, pump fittings, etc.).
A discrete knowledge base with the provision of complex care outside the scope of primary care or other specialties forms the identity of a division. The scope of BFLM providers is outlined in the “Recommended Core Competencies for Specialists Practicing Breastfeeding and Lactation Medicine” 8 and “Breastfeeding: A Guide for the Medical Profession.” 5 The Academy of Breastfeeding Medicine, the international medical organization of BFLM physicians, supports this work through their Clinical Protocols. 9 These competencies are evaluated for physicians in the recently formed board examination through the North American Board of Breastfeeding and Lactation Medicine. Examples of common outpatient presentations include infants with poor growth/failure to thrive, oral dysfunction, ankyloglossia, and lactating mothers/parents with chronic nipple conditions, complex mastitis, low milk production, and breastfeeding in the context of other medical concerns such as multiple sclerosis and cancer. We also work with patients prenatally and induce lactation, with a special focus on LGBTQI+ lactation concerns.
Inpatient lactation and BFLM services
The inpatient lactation services are staffed with RN/IBCLCs and overseen jointly by the Lactation Nurse Manager and the Division Chief. The division has gained considerable traction with other divisions and departments through its work supporting the educational, quality, and administrative missions of inpatient lactation services, including leading policy and procedure development. To streamline our inpatient lactation services, we began by merging our pediatric (NICU) and obstetric lactation services, consolidated meetings, and created a joint management structure. We increased staffing for providing services in all settings across the hospital system (pediatric, obstetric, emergency, surgical, psychiatric, etc.).10–12 Inpatient IBCLCs are central to staff training in breastfeeding and lactation management, review and implementation of policies and procedures, and Quality Improvement efforts in supporting lactating families. They serve as the front line for identification of practice inconsistencies and patient needs and are often part of the development of protocols to implement change.
IBCLCs and other services refer complex breastfeeding and lactation cases to BFLM providers, who round 5 days per week across all hospital units. Inpatient consults are typically related to the following: low milk production, medication evaluation, substance use disorder, and oral dysfunction in the NICU; poor growth/failure to thrive or metabolic disease on the pediatric floors; and complicated mastitis or breastfeeding in the context of severe illness or surgeries on the adult floors. In collaboration with our research team, we are able to provide analysis of milk macronutrients using a Miris HMA®, useful in select cases of infant metabolic disease, poor growth, or rare maternal conditions. We also partner with laboratory services and other teams (e.g., The InfantRisk Center© of Texas Tech University 13 ) to provide milk analysis in rare scenarios and have used cultures, electrolyte analysis, and medication passage in milk to inform clinical care.
The Lactation and BFLM teams work to create consistent protocols and formalize them in our medical record and patient handouts. Difficult topics requiring consistency of care between lactation/BFLM, pediatrics, and obstetrics (e.g., use of nicotine patches, Depo-Provera® at delivery, ankyloglossia management, parental substance use disorder) are brought to existing fora, and protocols are developed. Other efforts involve program growth, for example: Divisional leadership was able to advise and support the efforts of the NICU donor milk and human–human milk fortifier program in 2017, NICU breastfeeding and lactation support, and infrastructure to support these.
Human Lactation Study Center
The Lactation Study Center was established in 1981 through the pioneering efforts of Dr. Ruth Lawrence, who recognized the urgent need for accurate, timely, and evidence-based breastfeeding and lactation advice. Her work positioned the Center nearly 40 years ahead of other institutions, making it a leader in breastfeeding and lactation medicine, and advancing support for breastfeeding as essential to maternal and child health. The Center remains closely allied with the University of Rochester Departments of Pediatrics, OBGYN, Environmental Medicine, MotherToBaby® URMedicine since 2003, and the Finger Lakes Children’s Environmental Health Center since 2018. The foundation of this Center is a telephone and email hotline, in which advice is given free of charge to health care providers.
Questions concerning medications, toxic agents, and environmental and occupational exposures through human milk are answered by the Medical Director, an OBGYN Toxicologist, whereas advanced breastfeeding and lactation management problems are handled by the Division’s clinical providers. Questions are received via telephone, texts, and emails. Most of the responses provided by telephone are accompanied by written information via email with the appropriate references for each case. Information provided is for consultation only, and providers using the service make health care decisions for their own patients and are responsible for patient care. Consumers may access information and consultation through a partner program, MotherToBaby® URMedicine.
Integration efforts
Integration into the larger medical system is key to the success of a new division, to receive referrals, communicate a novel type of medical care, and ensure follow-up. This is a key benefit of offering services embedded in a medical model instead of the current standard—an IBCLC-only, out-of-pocket, home-based service model. We serve as a regional referral center for Western and Central New York and beyond. Referrals are built into the medical record, and we provide consult notes to the patient’s primary care and obstetric providers, a key component in care coordination and continuity. We also have an e-consult model, which has shown promise in answering clinical questions such as medication review for high-risk pregnant patients. This is an updated “curbside” model in which another provider consults BFLM directly through the medical record, the question is answered with a note by the BFLM provider, and a bill is generated. Providers routinely engage in care coordination in the inpatient and outpatient settings, from ensuring appropriate medication choices for safety in lactation to ensuring agreement among medical teams in complex cases. The lactation care management program is a novel approach to care provision and integration. This program is supported by grant funding and is fully integrated into three family medicine practices in our network. It offers pro-active peer counseling and lactation support while ensuring access to community resources and higher levels of care, when indicated.
Staff education, benefits, and improvement efforts
A major challenge involved the growth and maintenance of a high-level lactation consultant workforce. We sought to improve equity in educational opportunities for staff, add to the diversity of our workforce, and rapidly build and maintain a strong IBCLC presence in the hospital. The Division therefore funds the education and certification costs associated with the achievement and maintenance of the IBCLC certification. In addition, RN/IBCLCs stay on the same promotion pathway as other hospital RNs and are, therefore, able to complete quality improvement projects and gain seniority benefits. Some examples of quality improvement projects led by this team include building outpatient support groups, standardizing our medical record documentation, including auto-updating clinical handoff tools for LCs, and widespread staff training through the CDC (Centers for Disease Control and Prevention) funded EMPower project. 14 In year 8, a lead Quality Improvement position was added, staffed by a Doctor of Nursing Practice with a background in programs to promote, protect, and support breastfeeding.
Patient and family experience
A frequent criticism of the work of lactation consultants and BFLM providers is a concern for the judgmental delivery of care, culminating in negative patient experiences. This concern was expressed by patients, staff, faculty, and leadership at the beginning of our program. The ability to create and meet breastfeeding and lactation goals is heavily socially determined and the inability to do so is linked with parental guilt and poor bonding. 15 Furthermore, marginalized groups have traditionally struggled to access appropriate and reimbursed care. Inadequate, insensitive, or judgmental medical care compounds this sense of guilt. 16
To address these concerns, we developed clinical services with a goal to empower our patients and families through a goal-directed and guilt-free environment, with the shared understanding of all care providers to prioritize parental well-being and bonding. This work is supported through a digital platform in Labor and Delivery, which allows patients to directly consult lactation through the GetWellNetwork™ 17 and access a learning library for lactation hurdles. Our outpatient office is a donor milk depot for the New York State Milk Bank, and we have established relationships with durable medical equipment providers to distribute breast pumps at our office location. Patients can access care in person, by telemedicine, electronic medical record messaging, virtual and in-person group, and by email. Collaborative relationships and regular meetings with community infant feeding, body work, lactation, and dental specialists allow us to help patients receive consistent, evidence-based care across the community. Technicians and administrative staff are trained in lactation and given shadowing experience to better understand the struggles faced by patients. A callback list enables us to track and follow high-risk patients (e.g., post-frenotomy, mastitis) proactively.
Creation of healing spaces
Leveraging emerging science in the importance of healing environments, 18 we have endeavored to use evidence-based but low-cost approaches to create our clinical spaces. Our waiting room is designed as a living room, with a bookshelf, toys, a play area, and artwork. Natural colors are used throughout the patient spaces, including our group room. Floor lamps allow us to reduce the overhead fluorescent lighting to improve infant comfort. Incorporating natural elements into workspaces has the potential to improve staff well-being and reduce stress. For the benefit of staff as well as patients, we have plants, natural seasonal décor, and a table-top fountain at checkout. Patient materials and office decor include diverse representations of patient race/ethnicity, genders, parents, and feeding types (breast, chest, pump, bottles), which promote a feeling of belonging. To improve the care of patients at risk of stigma in health care, our seating allows for larger bodies and we do not routinely weigh adult patients, both of which are advertised online. Rainbow stickers demonstrating our internal “Safe Space” training shows LGBTQI+ patients that they can expect respectful care. Our bathroom sign indicates safety for all genders. Medical charts reflect affirmed names and pronouns, and staff are trained in inclusive care at all levels. Medical interpreters are provided in person and online, and core teaching materials are available in other languages. We work with Medicaid to assist families with transportation. Both formal and informal patient and staff feedback suggest that these interventions are positively received and promote the healing environment.
Research
The Departments of Pediatrics, Public Health Sciences, and OBGYN (among others) at the University of Rochester have long been leaders in the field of breastfeeding and lactation research. This long-standing reputation for excellence is built upon the rich legacy of Dr Ruth Lawrence’s foundational work. Her tireless efforts to highlight and enhance the scientific basis for the field of BFLM shaped the field. Her legacy of trainees dedicated to this cause has circumvented the globe. Her presence is a main reason that the scientific field of BFLM has remained a sustained focus at the University throughout the years. Furthermore, many faculty with research interests in this area came to the University of Rochester in part, or primarily, due to Dr. Lawrence and this lasting focus and reputation.
Due to this steady influx of passionate faculty, we currently host 36 faculty that have direct or peripheral research interests in BFLM. In 2023, this group represented a combined ∼$32 million in active research grants related to breastfeeding/lactation, with another ∼$14 million in grants under review. Roughly $2.5 million of this funding is for programmatic interventions and outreach programs from various sources, including New York State. These awards mostly represent small groups of collaborative investigators operating in siloed disciplines across the University. In 2019, before the formation of a formal division of BFLM, researchers from Pediatrics and Public Health Sciences established the University of Rochester Human Milk and Lactation Research Consortium in an effort to coalesce these scattered areas of expertise and strategically preserve and enhance the University’s reputation for excellence in the field of BFLM. Dr Ruth Lawrence was an attendee at the consortium’s founding meeting. This group includes 17 core research faculty with direct work in BFLM and human milk from 13 departments/divisions across the academic medical center. This consortium provides organizational infrastructure for collaborative work and shared expertise, samples, learners, and funding opportunities.
In 2022, a Research Director was appointed within the Division of Breastfeeding and Lactation Medicine. This role endeavors to strategically hone our reputation for cutting-edge research that advances the forefront of care in BFLM. We capitalize on the following two underlying factors that have been at the core of the University’s reputation for excellence in BFLM: (1) an unrelenting ultimate focus on driving improvements in health outcomes of the mother/lactating parent and infant dyad and (2) interdisciplinary representation across the spectrum of translational science.
Focus on driving improvements in health outcomes of the mother/lactating parent and infant dyad
This consistent focus over the years has shaped our research program to move beyond simple associations between breastfeeding, components in human milk, and outcomes. A key feature of our research programs is the mechanistic work that has assessed regulation of human milk composition and the effects of human milk at a deeper level. Examples of this mechanistic exploration include work assessing maternal effects on human milk composition, including stress, 19 lifestyle, 20 atopy, 21 chemical exposure, 22 and probiotic and antibiotic therapies.20,23 Examples of the mechanistic work include tissue culture models that have explored the effect of human milk components on Toll-Like Receptor (TLR) activation, 24 Immunoglobulin A (IgA) class switching, 21 and basophil activation. 25 This research provides an important missing link in our understanding of the effect of human milk feeding in development of infant immunity.
Interdisciplinary representation across the spectrum of translational science
As an example of our transdisciplinary strength, our faculty are conducting research in BFLM and related fields that include molecular investigations of human milk composition and how it interacts with infant physiology on the cellular level, clinical studies of breastfeeding mother/lactating parent and infant dyads, studies of social ecological factors that impact breastfeeding behaviors and outcomes, implementation science studies evaluating the success and sustainability of models of BFLM clinical care, and breastfeeding support programs. Our ability to leverage expertise along this entire spectrum of translational research enhances our ability to implement research findings into clinical care.
Figure 3 demonstrates how these two factors coalesce to keep the University of Rochester at the cutting edge of clinical care of perinatal populations and the ripple effect at a national level.
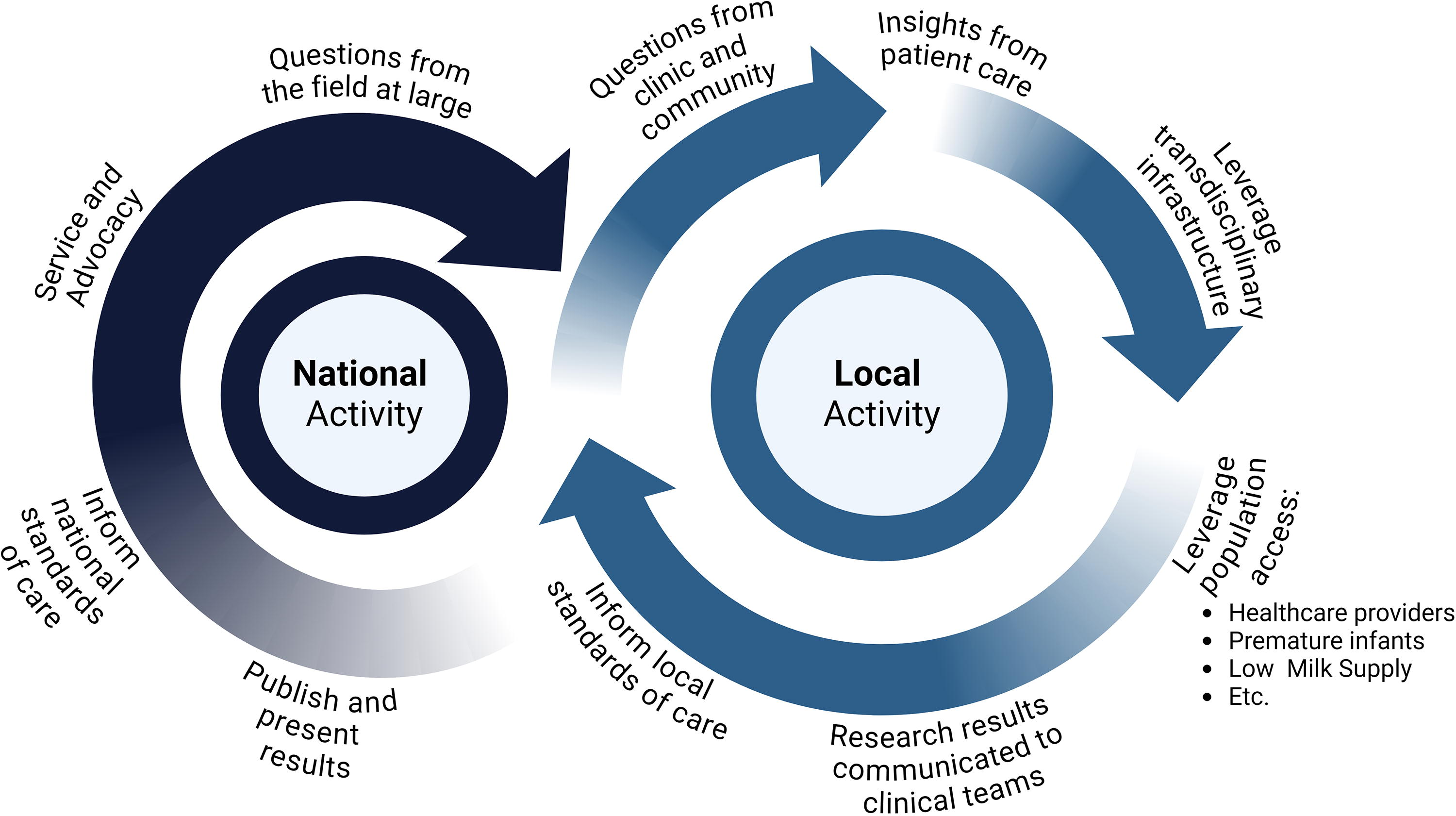
Local and National Feedback Loops Across the Spectrum of Translational Science Necessary to Consistently Push the Cutting Edge of BFLM Research and Clinical Care. Created in BioRender. Young, B. (2024) https://BioRender.com/x60z258. BFLM, Breastfeeding and Lactation Medicine.
A few factors contribute to the success and sustainability of the local research-to-clinical care feedback loop. These include our direct access to acute patient concerns and issues from a variety of clinical inputs, including both outpatient and inpatient BFLM services; our access to transdisciplinary experts in this space (organized with the research consortium); and our access to both healthy infants20,26,27 and donor milk, 28 as well as specialized patient/research populations, including health care providers, 29 premature and medically fragile infants,19,30,31 infants with a variety of diagnoses, including ankyloglossia,32–34 infectious exposure,29,35 and allergic diseases,20,21,25,36–38 and mothers/lactating parents with a variety of unique diagnoses,39,40 including low milk supply. Another necessary step in this feedback loop is the regular communication and feedback between researchers and clinical providers. This results in a more rapid implementation of evidence-based improvements to clinical care than is commonly observed in other health care settings.
At the national level, it is important that our research mission pursues the standard metrics of a successful research program, including funding and publication and presentation of results. Another crucial component of our national activity is the significant service work our faculty undertake in support of both advocacy and policy changes to accelerate dissemination and implementation of new scientific evidence at the level of acute care, public health guidance, and state and national policies. This work includes service and leadership roles for national and international professional organizations and service on national expert committees that affect policy,41,42 summarize the current state of evidence to define the research needs of the future,43–45 and provide guidance and protocols for best practices in providing evidence-based care.46–49 This perpetual dual feedback loop continues to churn based on the dedication of those involved. The service work, advocacy work, open collaborative nature, and open-minded approach of all involved are critical to continued success.
An example of how we capitalize on this framework can be found in our response to the COVID-19 pandemic. Located in New York, our academic medical center suffered the initial and virulent infection rates in 2019–2020. Questions related to the safety of human milk, postpartum separation, and general care of breastfeeding and lactating families were immediately apparent and raised by our health care providers and patients. Our research teams were consulted and were able to mobilize the expertise and existing infrastructure studying breastfeeding dyads to conduct one of the first studies of infected mothers in the country. Our findings of anti-SARS-CoV2 antibodies without any live virus in human milk allowed our hospital, outpatient clinics, and Lactation Study Center to support continual provision of maternal milk before the findings were even published. 50 In December 2020, we were the first to expand this study to include vaccinated mothers and lactating parents, capturing a population of lactating health care providers with first access to the vaccine. 29 Follow-up studies assessed the cross-reactive antibodies induced by different strains of coronaviruses. 51 These findings changed standards of care at the national level, but were implemented locally immediately.
Education
A key contribution of any university division is educating medical and nursing learners, as well as staff, across the system. This education not only enhances future care for lactating individuals but also broadens the knowledge and availability of BFLM services throughout the health care system, extending to wherever learners will eventually practice. Because of our expanded clinical services, we have been able to increase our teaching opportunities. A formal 2-week rotation for medical students, residents, and fellows was established in year 3, with online didactics and in-person clinical learning. Learning opportunities include inpatient and outpatient BFLM work, a day with our toxicologist at the Lactation Study Center, inpatient rounding with lactation consultants, and opportunities to attend support groups. We also host many learners for half and full day shadowing opportunities, including medical and nursing students, residents (pediatric, family medicine, OBGYN, pediatric dentistry, med/peds, ENT), fellows (maternal fetal medicine, NICU, NICU NP), and midwifery students. We provide routine lectures in the medical school, residencies and fellowship programs, grand rounds, and community presentations. We partner with OBGYN and Pediatric faculty to provide simulation-based lactation education to residents.
Divisional in-person fellowship
The first formal fellowship in BFLM was offered to a pediatrician supervised by Dr. Ruth Lawrence and nested under a 2-year General Academic Pediatrics fellowship. The second fellow, a midwife, completed a 3-year academic fellowship funded by the Department of OBGYN. A current divisionally funded fellowship recruits one fellow every other year and offers opportunities for academic work and advanced degrees. No ACGME (Accredidation Council for Graduate Medical Education) accredited fellowships exist in BFLM.
LILAC fellowship (Lessons In Lactation Advanced Curriculum)
Because of the expressed need and interest in our fellowship, we developed a 2-year online fellowship using adult learning principles and a community of learners approach. Based on the “Recommended Core Competencies for Specialists Practicing Breastfeeding and Lactation Medicine,” 8 the fellowship includes 18 didactic, flipped-classroom modules incorporating experts in the field with group learning. This program provides physicians and advanced care providers with the clinical, academic, and practical expertise to provide complex-care support for any lactation-related patient concern. A robust research curriculum teaches core principles of BFLM research and gives fellows an opportunity to take a project to completion (presentation and publication). We enroll overlapping cohorts each year, so that first- and second-year fellows inform each other’s work and growth. We have graduated 13 fellows across 4 countries and have 12 fellows currently enrolled from 3 countries. Preliminary program evaluation showed improved knowledge, confidence, and impact on patient care. 52
Discussion
Our BFLM Division grew out of 8 years of program development. With a strong foundation in the work of Dr. Ruth Lawrence, the legacy of her trainees in clinical and research areas, and the science she and other pioneers developed and distributed, 5 a championship model was institutionalized into a sustainable division with clinical, research, and educational contributions. Our success is supported by our efforts to create and maintain shared goals across multiple services and departments, with the Division supporting hospital goals and vice-versa.
Institutionalization into existing infrastructures is better positioned to ensure sustainability in the case of revenue changes, leadership transitions, or staff turnover. Sustainability is also promoted by the development of key positions within the Division: the Division Chief, Assistant Medical Director, Lactation Nurse Manager, and Research Director. Using a multidisciplinary approach and having the support of two departments (Pediatrics and OBGYN) have been critical to the success of the program, which has involved several years of deficit as we work to improve reimbursement. Challenges in the growth of the Division included clinical disagreements between services, identifying and training staff, negotiating reimbursement with insurers, building electronic medical record infrastructure, and creating standard and reproducible data reports for tracking interim outcomes.
Building our research infrastructure has taken many years of consistent and collaborative effort. A unique feature of our program is the focus on clinically important research questions and the rapid translation of findings to clinical spaces. Additional expansion faces many challenges. Funding remains a consistent challenge in this field. While breastfeeding, human milk, and perinatal care have received increasing attention at the national level, this has not translated into increased dedicated funding. Our collective National Institutes of Health (NIH) funding is distributed across multiple institutes, lacking a dedicated institute or focused study section specific to this field. Traditionally, our faculty have had better funding success focusing BFLM research on nonlactation-related outcomes, based on current funding priorities. Due to this funding challenge and limited education on BFLM in the medical sphere, there is a limited number of researchers conducting work in this area, making transdisciplinary collaboration essential to success. Downstream of these challenges is limited access to students and trainees who are necessary to ensure future growth in the field. Our strategic plan for expansion includes assessing each of these challenges.
Teaching multiple groups of learners not only supports our mission to provide education in lactation and breastfeeding, lactation, and maternal health (BFLM) but also reinforces our role across various areas of the hospital network. However, this level of engagement carries costs that may not be as prominent in divisions where core knowledge is obtained through standard medical training. Most medical training programs still exhibit significant gaps in breastfeeding and lactation education,32,53 prompting many to turn to BFLM learning experiences to address these deficiencies. The demand for these experiences, however, often exceeds the capacity of our faculty, lactation staff, and available facilities. Our challenge is to continue to work to incorporate basic breastfeeding education into our medical school and training programs and provide advanced and engaging education across the University. Fellows have typically sought foundational training in BFLM, and therefore, deficiencies in education are not a hurdle. Rather, both in-person and online fellows are expensive to train, and funding sources are lacking for this novel and recently boarded subspecialty.
Conclusion
With ever-increasing numbers of patients desiring to breastfeed and the increased understanding of its importance, the science and care of breastfeeding and lactating families must continue to evolve. Building on the prior work of visionaries such as Dr. Ruth Lawrence, a pioneer in the field of BFLM, BFLM faculty bring innovative care founded in the needs of patients and are at the forefront of leading research. Robust research programs are needed to address the historical inadequacy of answers in this area, and robust education programs are required to remedy deficiencies and promote appropriate management. The multidisciplinary growth of a BFLM program at a large academic medical center may serve as an example of the integration of BFLM in a university setting with a focus on sustainability and growth of services and research. Integration of multiple service lines and collaboration among provider specialties and types was key to successful growth, with the culmination as a stand-alone division. Main challenges surrounded reimbursement, data collection, and infrastructure.
Footnotes
Acknowledgments
The authors would like to acknowledge the Departments of Pediatrics (especially the late Dr. Pat Brophy and Drs. Jill Halterman and Carl D’Angio) and OBGYN (especially Drs. Eva Pressman and Loralei Thornburg) at the University of Rochester for their extensive financial, administrative, organizational, and moral support of the program and our patients. Donna Vogt-Barrows and Jillian Price have significantly supported the mission for our nursing and lactation staff. Dr. Jena Ashley was foundational in the administrative build of the new Division. The work is made possible by the commitment to excellent patient care exemplified by our lactation consultants every day. The field of BFLM, and especially our program at the University of Rochester, owes its foundation to the energy, passion, intelligence, and bravery of Dr. Ruth Lawrence.
Authors’ Contributions
C.B.R.C.: Conceptualization, project administration, methodology, formal analysis, visualization, writing—original draft, and supervision. M.B.: Project administration, resources, supervision, and writing—editing, A.D.: Conceptualization, resources, and writing—editing, L.G.: Project administration, supervision, writing—editing, and data curation, K.J.: Conceptualization, methodology, resources, program administration, and writing—editing, A.J.: Resources and writing—editing, S.H.: Resources and writing—editing, O.L.M.: Resources and writing—editing, R.P.D.G.: Resources, project administration, and writing—editing, K.P.: Resources and writing—editing, and B.E.Y.: Conceptualization, methodology, resources, program administration, and writing—editing.
Disclosure Statement
The authors have no disclosures or applicable conflicts of interest.
Funding Information
No grant funding was used for the development of this program or division.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.