
Abstract
Introduction:
The benefits of breast milk (BM) for infants have long been established. However, for health-compromised infants with difficulty processing long-chain triglycerides, BM is often discontinued, and skimmed breast milk (SBM) is used as a dietary treatment. SBM is usually produced for inpatients in a hospital laboratory. The aim of this study was to determine the viability of skimming BM at home.
Case Report:
A female infant was diagnosed with
Methods:
A nonrefrigerated benchtop centrifuge was used to produce SBM at the patient's home. The optimal setting for the centrifuge was determined and then used to process BM samples from the infant's mother. The samples were randomly selected from each 10-day period over 6 months, and 18 samples were processed in total. The hospital laboratory processed the same samples of BM and analyzed the macronutrients with a comparison of the home-produced SBM to the hospital-produced SBM.
Results:
The home-produced SBM met the dietary treatment requirement of <1.0 g/dL of fat content. Fat was significantly lower, proteins were significantly higher, and carbohydrates and calories were not significantly different compared to hospital-produced SBM.
Conclusions:
It is viable to consistently produce SBM at home that meets the dietary treatment requirements of health-compromised infants.
Introduction
The benefits of breast milk (BM) for infants have long been established. BM provides essential nutrients for infant growth and development and supplies immunological components as an infant's immunity is formed. These benefits cannot be completely matched by formula. 1 Exclusive BM feeding for the first 6 months of life and continued BM feeding for 1–2 years are considered the gold standard of diet for infants. 2
Since most of the fat content of BM is composed of long-chain triglycerides (LCT), infants with difficulty processing LCT usually have to give up BM and its associated benefits for either the short term or the long term.5–7 The MCT formula can be expensive or unavailable in certain regions/countries. 8 Therefore, many clinicians use skimmed breast milk (SBM) fortified with MCT as dietary treatment for these patients.7,9–13
SBM is the nearly fat-free fraction of BM in which almost all LCT have been removed. SBM has lower calories because of the loss of fat content and must be fortified to provide adequate nutrition.5,11,13,14 Based on the literature review, the fat content of SBM should be <1.0 g/dL when used as a dietary treatment.9,15,16 While SBM demonstrates a significant decrease in all immune cell populations, other antimicrobial properties are preserved; therefore, infants can still receive BM's developmental and immunological benefits from SBM. 17
SBM is usually produced in a hospital laboratory using a refrigerated centrifuge for inpatients. Outpatient families may have difficulty accessing hospital-produced SBM, and some families may have to remain in inpatient care for SBM access. Some hospitals had outpatients returning to the hospital biweekly for SBM. 13 However, this approach is not feasible for most nonlocal families since the monetary costs and time spent on transporting SBM can be significant. Manual fat removal after natural separation is often performed by outpatient families when SBM is recommended after discharge. 18 However, even when a trained technician performed manual fat removal, the resulting SBM still contained too much fat content to be used for dietary treatment. 18 Therefore, a better method for separating fat is needed. The goal of this study was to explore the viability of skimming BM at home, as well as to develop a procedure for doing so, producing SBM that meets the dietary treatment requirement of <1.0 g/dL of fat content.
Case Report
We present the case of a female infant with prenatally diagnosed chylothorax and left upper-extremity lymphedema/lymphatic malformation. Examination and imaging at birth were consistent with thoracic lymphatic malformations, showing a very large left pleural effusion with a dextroposition cardiac mass, left upper-extremity lymphedema, and capillary malformation of the left chest wall. Given the constellation of findings, the patient met the clinical criteria for CLOVES syndrome.
She was started on sirolimus 1 week after birth. During the hospital stay, the patient received partly oral, partly nasogastric tube feeds of SBM with MCT-enriched formula (Enfaport), and her chylothorax was brought under control. The patient was discharged at 3 months of age. The family acquired a benchtop centrifuge, intending to keep BM as part of the infant's diet so that she could continue to receive BM's benefits. The patient's family experimented with skimming BM with the support of the hospital and consistently produced SBM at home that met dietary treatment requirements. At 10 months of age, the infant's chylothorax was still under control, and pleural effusion remained minimal.
Methods
Gold standard
At Texas Children's Hospital (TCH), SBM was prepared using a refrigerated benchtop centrifuge (Hettich Rotina 380 R) running at 503 g for 15 minutes at a temperature of 2°C to 4°C to minimize microbial growth. The macronutrients of prepared SBM were then analyzed using a near infrared analyzer (Unity Scientific SpectraStar Rotating Top Window System) to ensure that the SBM met the requirement for dietary treatment of <1.0 g/dL of fat content. The SBM would be discarded if its temperature rose above 37°C during the process.
Home production of SBM
Freshly pumped or thawed frozen BM stored in sterile bottles (SteriFeed 130 mL) was mixed well in a beaker (1,000 mL) and divided into sterile centrifuge tubes (Sunne, 50 mL). A nonrefrigerated centrifuge (Sunne SN-LSC-40S) was used in this study. Centrifuge tubes with BM were loaded into the centrifuge while maintaining weight balance.
Establishment of optimal centrifuge setting
Each of the three randomly selected BM samples were divided into five aliquots. All aliquots were processed using the following centrifuge settings based on recent studies9,13,15,16,19,20:
Setting 1: 894 g for 40 minutes
Setting 2: 894 g for 30 minutes
Setting 3: 685 g for 40 minutes
Setting 4: 685 g for 30 minutes
Setting 5: 685 g for 20 minutes
All aliquots were analyzed at TCH to determine fat content. The results were grouped by the centrifuge setting (Fig. 1) to establish the optimal centrifuge setting.
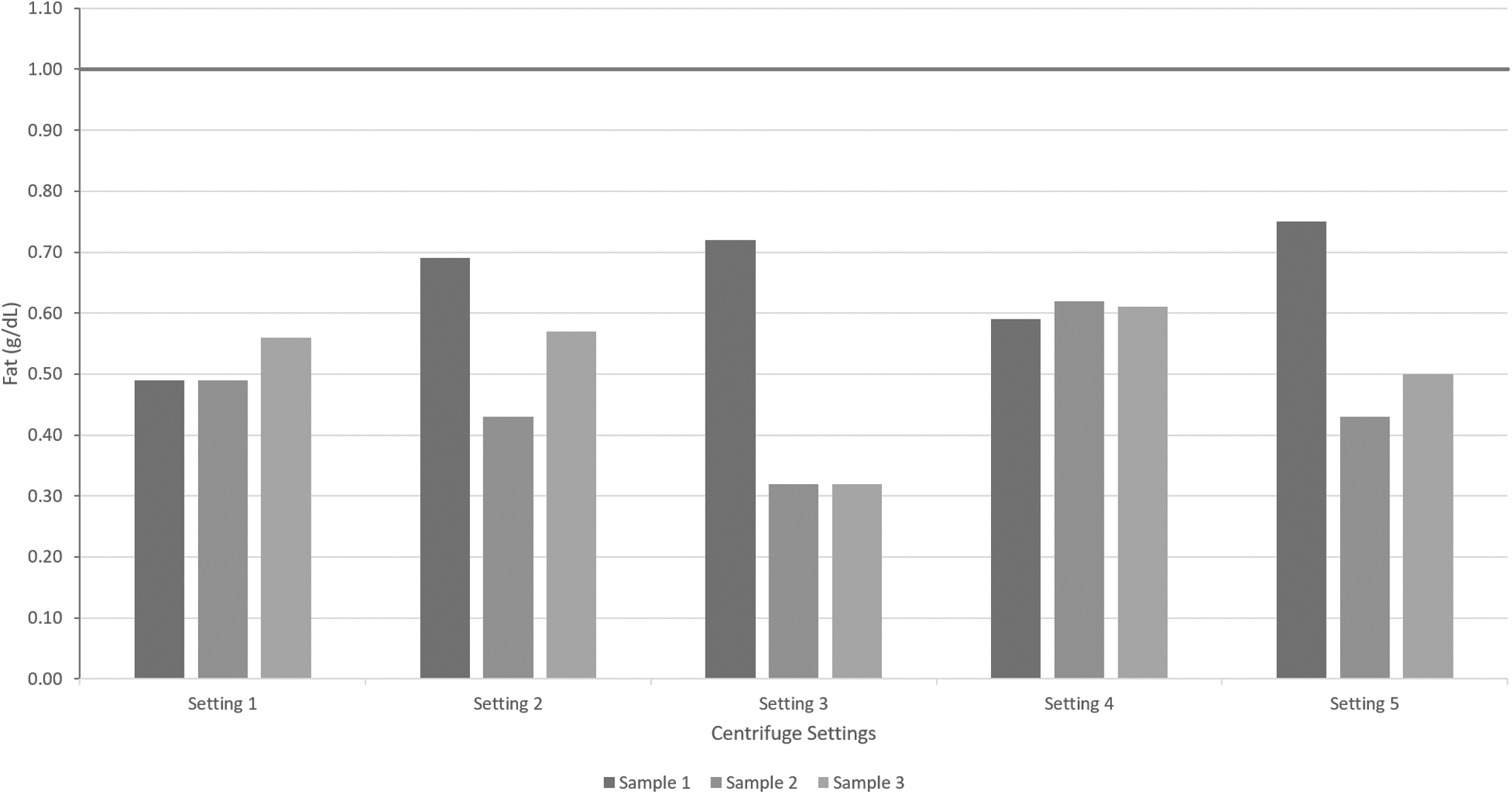
Optimal centrifuge setting determined by comparing the fat content of SBM produced at home using different settings. Setting 1 was 894 g for 40 minutes. Setting 2 was 894 g for 30 minutes. Setting 3 was 685 g for 40 minutes. Setting 4 was 685 g for 30 minutes. Setting 5 was 685 g for 20 minutes. The
Comparison of macronutrients
Each sample consisted of all BM collected by the patient's mother over a 24-hour period and stored in a freezer. One sample was randomly selected from each 10-day period, for a total of three samples per month. Eighteen samples were collected in this way during the January 2023–June 2023 period. The rationale for using this sample selection method was to minimize possible differences in the nutritional composition of the BM during different time periods. Each sample was divided into three aliquots. One aliquot was left unprocessed as the baseline. The next aliquot was sent to the TCH for processing at the hospital laboratory. The last aliquot was processed at home using the optimal centrifuge setting obtained from the previous step. The macronutrient contents of all three aliquots of the sample were then analyzed at TCH, and hospital-produced SBM and home-produced SBM were compared (Fig. 2).
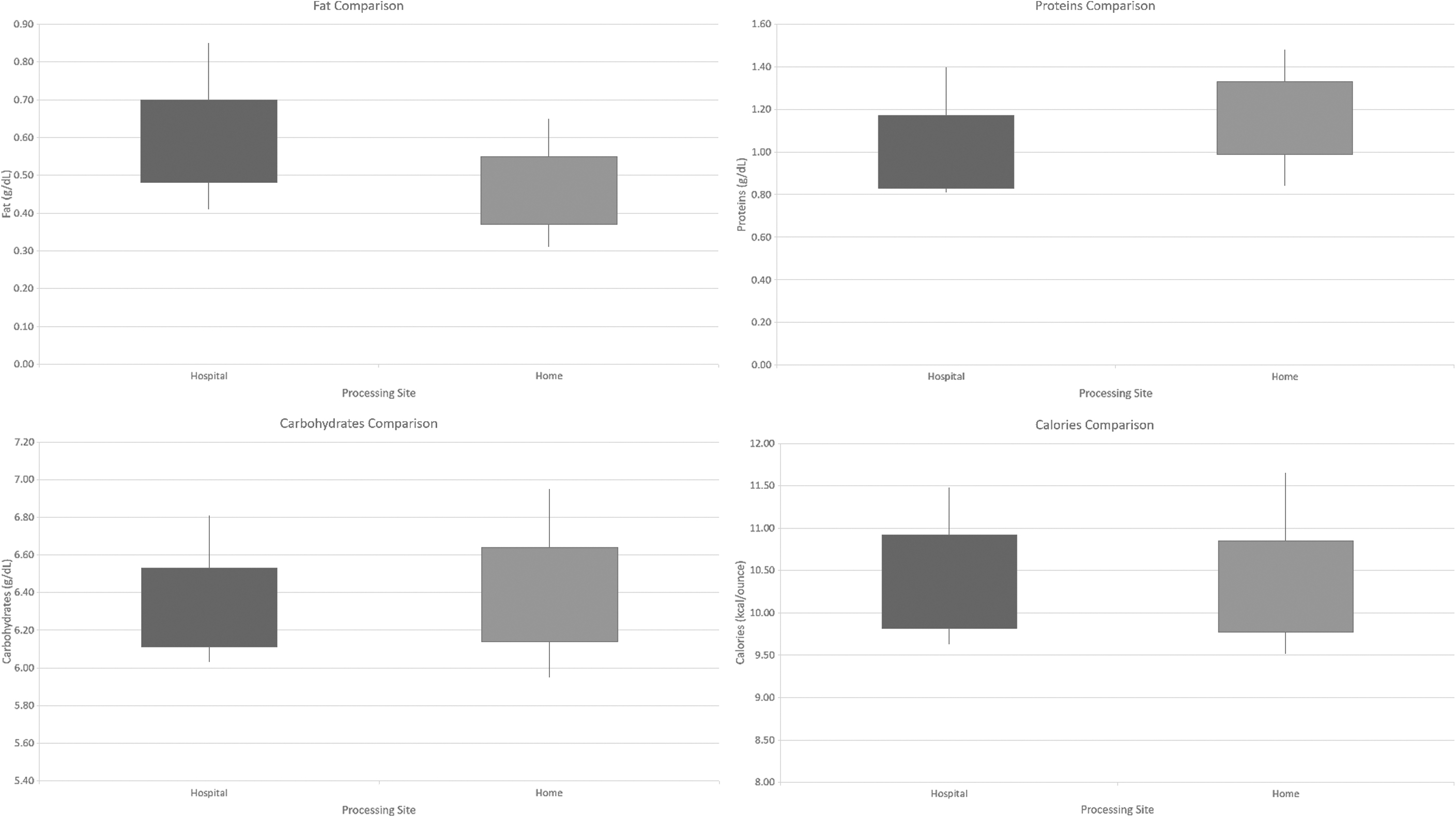
Comparison of fat, proteins, carbohydrates, and calories between hospital-produced and home-produced SBM. Processing site on the x-axis indicates where the BM was processed as well as the processing method used. BM, breast milk.
Data collection
Laboratory results were retrieved through the Epic electronic medical record system at TCH and manually transferred into Excel.
Statistical analysis
Data were analyzed using IBM SPSS Statistics for Windows, Version 28.0 (IBM Corp., Armonk, NY). To determine the optimal centrifuge setting for the home production of SBM, the fat content of home-produced SBM obtained at five different centrifuge settings was summarized with descriptive statistics. To compare the macronutrient contents of hospital-produced and home-produced SBM, the fat, protein, carbohydrate, and calorie contents of SBM were summarized with descriptive statistics. An independent samples t-test was used to compare each macronutrient of hospital-produced SBM and home-produced SBM.
Results
Determining the optimal centrifuge setting for home production of SBM
The mean fat content in home-produced SBM using each of the five settings was 0.51 (standard deviation [SD] 0.04) g/dL, 0.56 (SD 0.13) g/dL, 0.45 (SD 0.23) g/dL, 0.61 (SD 0.02) g/dL, and 0.56 (SD 0.17) g/dL (Fig. 1). Since all settings produced a fat content below the hospital requirement of 1.0 g/L for SBM, setting 5 (685 g for 20 minutes) was selected as the optimal centrifuge setting for home production of SBM because it required the least amount of processing time.
Comparing the macronutrients of hospital-produced SBM and home-produced SBM
There was a significant difference in the fat content between hospital-produced SBM (mean [M] = 0.59, SD = 0.11) and home-produced SBM (M = 0.46, SD = 0.09); t(34) = 3.709, p < 0.05. The fat content of home-produced SBM was significantly lower than that of hospital-produced SBM. The protein content of home-produced SBM (M = 1.16, SD = 0.17) was significantly higher than that of hospital-produced SBM (M = 1.00, SD = 0.17); t(34) = −2.745, p < 0.05. No significant difference was noted in carbohydrate content between hospital-produced SBM (M = 6.32, SD = 0.21) and home-produced SBM (M = 6.39, SD = 0.25); t(34) = −0.914, p = 0.367, and no significant difference in calorie content between hospital-produced SBM (M = 10.37, SD = 0.55) and home-produced SBM (M = 10.31, SD = 0.54); t(34) = 0.317, p = 0.753.
Discussion
We first used the gold standard centrifuge setting from TCH (503 g for 15 minutes) during the preliminary experiments and found that the resulting SBM had fat fragments along the side of the centrifuge tube, and the fat content was inconsistent. Therefore, we reviewed recent studies and used centrifuge settings from previous studies to design our experiments. Given the variety of centrifuges in the market, determining the optimal setting for home production is necessary to achieve the desired results.
By comparing the macronutrients of hospital-produced SBM and home-produced SBM, we determined that the fat content of home-produced SBM consistently met the dietary treatment requirement of <1.0 g/dL. Additionally, protein and carbohydrate content comparison showed that home-produced SBM has nutritional value similar to that of hospital-produced SBM. Finally, the caloric content was used by a nutritionist to determine the formula for SBM fortification.5,11,13 Home-produced SBM, with lower fat and higher protein content, may be more beneficial than hospital-produced SBM for infants with difficulty processing LCT.
Although this study sought to enable families with health-compromised infants to produce SBM at home, professional and hospital laboratory support is still required for optimal centrifuge setting determination, macronutrient analysis, and nutritionist consultation. The production of SBM at home is feasible only with professional guidance, proper patient training, and education.
Commercially available, specialized MCT formulas can be expensive or unavailable in certain regions and countries. 8 Some studies7,10 have suggested that SBM can be fortified with MCT oil, which is a safe and inexpensive alternative that can help address the issues of cost and availability. The exact ratios of SBM and MCT oil for fortification may vary case by case, and a dietary nutritionist should be consulted to prepare fortified SBM that includes proper nutritional components.
Based on the experience of the patient's family from our case report, the cost of home-produced SBM was likely lower than hospital-produced SBM. However, we cannot confidently extrapolate what we learned beyond this single case. For home-produced SBM, the patient's family purchased a centrifuge from China for ∼$200, and the shipping cost to the United States was ∼$250. No maintenance costs were incurred for the home centrifuge during the study period. Supplies were purchased for ∼$80. For hospital-produced SBM, many of the costs involved were proprietary, such as the cost of the refrigerated centrifuge, supplies, and lab staff salaries. An Internet search showed that a similar refrigerated centrifuge model costs around $16,000. The lab provided the skimming and macronutrient analysis service free of charge with management approval for our study and the patient in our case report. It is difficult to estimate the exact cost for the hospital to produce SBM, including equipment, indirect expenses, labor, and supplies, since this was not the focus of our study.
While a study by Barbas 18 used a cream separator to skim BM, this was not considered for our study. The cream separator works best with milk at a physiological temperature of 37°C according to online product reviews. Both TCH guidelines and previous studies indicate that nutritional and immunological values in BM begin to deteriorate at temperatures higher than 40°C, and bacterial growth is considerably higher at 38°C, even during a relatively short period of 4 hours. 21 Energy transfer from the skimming process will likely increase the BM temperature to these critical values.
A sample brochure for the families interested in skimming BM at home was prepared as Supplementary Data for this study. Information in the brochure should be used as part of a hospital education program to provide training for home-produced SBM under the guidance of professional laboratory staff.
Significance
The ability to produce SBM at home that meets the dietary treatment requirements for health-compromised infants with comparable nutritional value to hospital-produced SBM can be a crucial support for families needing short- and long-term treatment. Although switching to a commercially available specialized MCT formula is a viable option, infants will miss out on the benefits of BM during critical development period. The availability and affordability of these specialized formulas can also become limiting factors for dietary options in some regions/countries. 8 Substituting part of the special MCT formula with SBM or using SBM fortified with MCT oil can help reduce the cost of dietary treatment.
A procedure to produce SBM that can be performed at home may help reduce the economic burden, mental stress, and the time and cost of traveling to procure hospital-produced SBM. For families without convenient access to a hospital, using SBM fortified with MCT formula or oil may lead to cost savings when compared to an MCT formula–only diet. The length of stay for inpatients may also be reduced if the only barrier to discharge is access to SBM, and hospitals can better utilize their limited medical resources in this regard. A reduced length of hospital stay can also positively impact the financial burden for patients and health insurance providers, even when considering the costs of purchasing or leasing centrifuges and the supplies needed for home production of SBM.
Limitations
To minimize equipment variability, all experiments on home-produced SBM were performed using the same centrifuge, and further studies should be conducted to verify whether similar results can be achieved with other centrifuges. Furthermore, given that all BM samples were from a single source, more extensive studies enrolling other subjects should be conducted to substantiate our procedure for home production of SBM. Finally, the home-produced SBM was analyzed at a single institution (TCH) and not verified by a third party. Further studies with access to more than one laboratory capable of macronutrient analysis should perform external quality assessments to verify the analysis results.
Conclusions
Chylothorax is a rare but serious condition in infants. SBM as a dietary treatment may be beneficial to prevent complications such as infections and malnutrition and should be available to families with health-compromised infants. Our study found that families can produce SBM at home with similar nutritional value to hospital-produced SBM while consistently meeting dietary treatment requirements. With the support of hospital laboratories and patient education, home production of SBM helps the hospital focus resources elsewhere while lessening the logistical constraints associated with acquiring SBM for the families of health-compromised infants.
Footnotes
Acknowledgments
TCH Milk Bank (Lab) Services, Houston, TX, participated in literature review, BM skimming, and macronutrients analysis by request of the author. The authors would like to thank Dr. Amy Hair, Dr. Dantin Roddy, Ms. Joseph, Ms. Laviolette, Ms. Tucker, and their team for providing additional information and raw data for this information. The authors would like to thank Dr. Carol Carman for advice on statistical analysis.
Authors' Contributions
Y.H.: conceptualization (lead); data curation (equal); formal analysis (equal); investigation (lead); methodology (lead); resources (equal); writing—original draft (lead); writing—review and editing (equal). E.M.N.: writing—review and editing (equal). N.B.V.: writing—review and editing (equal). D.J.: data curation (equal); formal analysis (equal); writing—review and editing (equal). L.S.L.: data curation (equal); formal analysis (equal); writing—review and editing (equal). K.N.T.: supervision (equal); writing—review and editing (equal). J.L.E.: conceptualization (supporting); supervision (equal); writing—review and editing (equal).
Ethical Approval
The study was approved by the Institutional Review Board of University of Texas Medical Branch as Non-Regulatory Activity.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.