
Abstract

T
We desired to assess transfer of triamcinolone acetonide into milk after injection with a higher dose of steroid. This case involved a 35-year-old, G2P2 Hispanic woman weighing 75 kg with a history of psoriasis and a family history of rheumatoid arthritis. She was diagnosed with left breast granulomatous mastitis during month 7 of her second pregnancy. She was unresponsive to three different antibiotic regimens and was started on 10 mg prednisolone by mouth for 3 months during pregnancy. Her disease flared after delivery, and she self-referred to the breast surgery clinic 1 month postpartum for further management. In the surgery office, she underwent injection of 120 mg (3 mL) of triamcinolone acetonide mixed with 6 mL of 2% lidocaine into a large phlegmonous area of her left breast. She pumped the left breast after injection and continued uninterrupted feeding from the right breast.
She subsequently was referred to rheumatology and started on oral azathioprine. She became asymptomatic after 3 months of treatment while continuing uninterrupted breastfeeding from the right breast. Throughout this postpartum time period, the baby struggled to remain latched to the left breast and the patient pumped this side only.
She volunteered to provide milk samples at multiple times: 0, 14, 73, 144, and 169 hours post-injection. This case report was deemed exempt from human subject review by the Amarillo TTUHSC IRB. We utilized the same high-throughput liquid chromatography mass spectrometry methodology as described in the previous publication to detect triamcinolone acetonide in these milk samples. 1 Though the Rosen–Carole report found no detectible drug, the higher dose in this case resulted in quantifiable triamcinolone acetonide milk levels in two of the five samples. These results are expected as unbound glucocorticoids that readily cross cell membranes and bind cytoplasmic receptors, preventing readily available drug for diffusion into the milk compartment. The maximum observed concentration in these samples was 24.9 ng/mL, 14 hours post-injection. Concentrations dropped to 2.11 ng/mL at 73 hours and then was found below the limit of detection which is 0.78 ng/mL as represented in Figure 1.
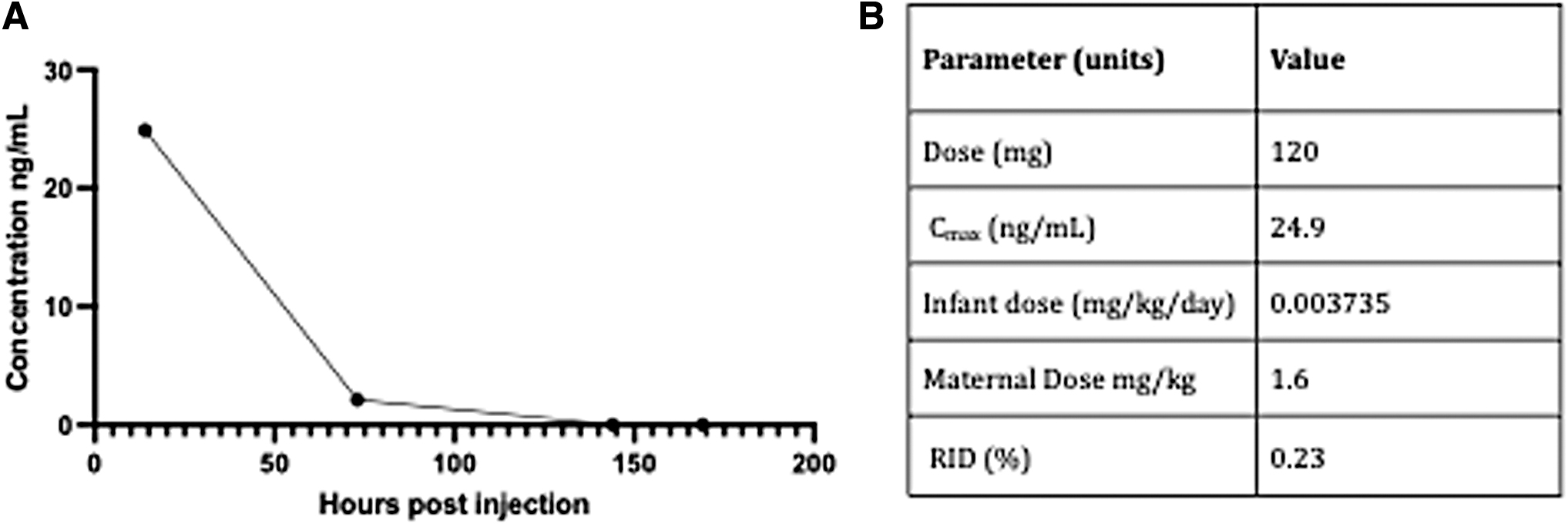
To simulate a worst-case scenario, the relative infant dose calculated from the maximum concentration is 0.23%. If this infant resumed breastfeeding at 14 hours following the maternal dose, the cumulative exposure would be no more than 0.23% of weight adjusted infant dose. Furthermore, the oral bioavailability of the drug is low. 2 The impact on breastfed infant from this exposure would likely be negligible.
These findings expand the prior analysis on triamcinolone acetonide's pharmacokinetics in human milk and the drug's safety data during lactation. Consequently, our measurements suggest no interruption of lactation on the affected breast should be required post-injection.
Aligning with the prior case report's conclusion, we emphasize the need for future research to discern the comparative efficacy of systemic steroids versus local injections in the treatment of granulomatous mastitis in lactating patients. While systemic steroids might minimally affect milk volume, they may pose additional health risks such as worsening anxiety and insomnia in postpartum women. Exploring nonsteroidal maintenance medications holds potential for further investigation. For example, azathioprine, an oral immunosuppressant with a demonstrated history of minimal transfer into milk, 3 has been reported to be safe and effective for resolving granulomatous mastitis. 4
Footnotes
Acknowledgment
We thank the participant's dedication to the health of future mother–infant dyads.
Authors' Contributions
Conceptualization: K.M. and T.W.H.; data curation: K.M. and P.D.; formal analysis: P.D.; investigation: K.M.; methodology: P.D.; project administration: K.K. and T.W.H.; resources: K.K.; software: P.D.; supervision: T.W.H.; validation: P.D.; visualization: P.D.; writing—original draft: K.M., K.K. and P.D.; writing—review and editing: K.M., K.K., P.D. and T.W.H. All authors have consented to the publication of this article in Breastfeeding Medicine.
Disclosure Statement
K.K. has served as a consultant for Advonate Clinical Development Strategies Ltd. K.K. and T.W.H. coauthor Hale's Medications and Mothers' Milk. The other authors of this article do not have any conflict of interest to disclose.
Funding Information
No funding was received for this article.