
Abstract
Objective:
To explore the influence of religious beliefs and faith on breastfeeding initiation among mothers in Israel.
Materials and Methods:
The study, conducted from February 2022 to July 2023 at Bnai Zion Medical Center (located in Haifa district) and Laniado hospital (located in Netanya, Sharon plain), included mothers and their partners who voluntarily completed questionnaires. The survey, comprising 26 questions, delves into religion, faith, religiosity, and infant feeding approaches, while considering various socioeconomic and health-related factors.
Results:
Religious and secular mothers exhibited a higher inclination toward exclusive breastfeeding compared with the traditional mothers (p < 0.001). Notably, more maternal education years were associated with more exclusive breastfeeding (odds ratio [OR] 1.59; 95% confidence interval [CI] 1.09–2.32; p = 0.017). However, older age of youngest sibling (OR 0.56; 95% CI 0.32–0.98; p = 0.041), cesarean delivery (OR 0.64; 95% CI 0.44–0.94; p = 0.023), and no desire to breastfeed during pregnancy (OR 0.67; 95% CI 0.57–0.80; p < 0.001) emerged as significant factors decreasing exclusive breastfeeding.
Conclusion:
The study indicates that the level of religiosity and prenatal intention to breastfeed impact breastfeeding practices, along with maternal education, age of the youngest sibling, and delivery mode. These insights provide valuable guidance for initiatives aimed at boosting breastfeeding rates, particularly in sectors where rates are comparatively low.
Introduction
Breastfeeding confers health benefits to both the breastfed baby and breastfeeding mother. The pair engaged in nursing is known as the breastfeeding dyad, and the benefits to the infant and mother encompass a wide spectrum, which is evident not only in the early postpartum period but also later in life. 1 The benefits for the infant range from tangible clinical outcomes such as decreased illness rates and mortality to subtler effects. Breastfeeding has been shown to reduce the risk of gastrointestinal infections,2,3 necrotizing enterocolitis,2,3 respiratory infections,2,3 sudden infant death syndrome,2,3 allergies, 2 asthma,2,4 type 2 diabetes,2,5 obesity,2,5,6 irritable bowel syndrome, 2 and Crohn’s disease, 2 and enhance cognitive abilities2,7 and emotional intelligence. 7 Human breast milk serves as the normative source of infant nourishment, playing a crucial role in enhancing global food security and promoting health. In addition, it holds significant economic value, highlighting the importance of accurate measurement and acknowledgment to safeguard its sustainability for generations to come. 8 Evidence-based advantages for breastfeeding mothers include lower rates of breast and ovarian cancer, osteoporosis, and cardiovascular disease. 9 It has also been found to decrease the likelihood of bleeding and anemia in the early postpartum period. 9 Furthermore, more nuanced impacts on the well-being of the breastfeeding mothers related to hormonal regulation and the fostering of the mother–infant bond facilitated by breastfeeding exist. 7
The World Health Organization and the United Nations International Children’s Emergency Fund (UNICEF) advise exclusive breastfeeding up to 6 months, followed by continued breastfeeding alongside complementary nutrition until the age of 2 years or more. 10 The Israeli Ministry of Health similarly suggests exclusive breastfeeding for 6 months, with combination of breastfeeding and complementary nutrition as long as it is suitable for both the mother and the baby. 11
Despite these guidelines, the prevalence of breastfeeding mothers is still relatively low. 1 According to a UNICEF survey from 2018, an estimated 41% of newborns were exclusively breastfed until 6 months of age.
Nursing is a complex practice impacted by a range of socioecological factors, including education, maternal employment, inadequate breastfeeding counseling before birth, aggressive formula promotion, lack of social support regarding breastfeeding, and religious beliefs. 12
Religious scriptures, including the Jewish Talmud and the Bible, often refer to breast milk. 13 Breastfeeding is used in the Bahá’í Writings as a symbol of divine generosity, presenting breastfeeding in a positive light. 14 The Quran has verses that refer to breastfeeding. In the very first chapter, the responsibility of the parents to provide their children with breast milk in their first two years of life is emphasized. 15 The Quran presents breastfeeding as the fundamental right of every newborn and infant. 16 Furthermore, in the Indian culture, evidence of the belief that breasts and milk symbolize sweetness and longevity can be found even in the earliest literature. 17
Many factors influence breastfeeding choices among mothers. Research suggests that women with higher levels of religiosity tend to breastfeed more than their less religious counterparts.18,19 For instance, a study of a predominantly Christian, unmarried population with low economic status found that women who regularly attended religious services were more likely to initiate breastfeeding, although this effect was more pronounced at initiation than in its duration. 20 Similarly, in a previous study in Jerusalem, ultra-orthodox Jewish mothers initiated breastfeeding significantly more than secular or traditional mothers. 19 In addition, previous reports worldwide have shown high breastfeeding rates among Jewish women, as demonstrated in studies from the United States and the United Kingdom.13,21 Conversely, Arabs in the United States and earlier reports from Israel have also shown high rates of breastfeeding initiation and duration compared with Jewish mothers.22–24
Studies have demonstrated the feasibility of enhancing both the initiation and duration of breastfeeding among mothers through effective interventions. 1 These interventions include offering relevant guidance to mothers, practical aid during breastfeeding, and emotional as well as social support. 1
Several scholarly reports propose that a mother’s choice to breastfeed may be influenced by her religious and faith beliefs.13,20,25 However, despite the potential significance of this intersection between religion and breastfeeding, there is a lack of data concerning the influence of religion and faith on the initiation of breastfeeding among mothers in Israel. Given Israel’s diverse ethnic and religious landscape and the role that religion plays in shaping societal norms and practices, this topic was of special interest. The aim of this study was to investigate the impact of religious beliefs and faith on the initiation of breastfeeding among mothers in Israel.
In Israel, religious populations vary widely, ranging from those who strictly adhere to traditional religious practices to those with a more modernized approach integrating contemporary life with religious observance. Traditional Israelis often exhibit lower levels of religious observance, potentially not actively practicing religious rituals or adhering to religious laws. Distinguishing between these distinct population segments is crucial when studying breastfeeding habits because cultural and religious beliefs greatly influence breastfeeding practices. Understanding the unique cultural norms, values, and attitudes toward breastfeeding within each group can facilitate tailored interventions and support programs to better address the needs and preferences of individuals in these communities, ultimately enhancing maternal and child health outcomes.
Materials and Methods
Study design
Conducted as a descriptive survey research, this study aimed to explore the relationship between the beliefs, religious affiliations, and level of religiosity of mothers in Israel and the prevalence of breastfeeding practices.
The research involved mothers and their partners who delivered term or late preterm (36–42 weeks of gestation) infants at Bnai Zion Medical Center in Haifa and Laniado Hospital in Netanya, Israel, within the time frame of February 2022 to July 2023. Inclusion criteria consisted of mothers and their partners who willingly completed the provided questionnaires, regardless of their newborn feeding choice. Conversely, the study’s exclusion criteria included those who were unable to fill out the questionnaire for any reason or declined to participate.
To verify respondent anonymity while linking the questionnaires of the mothers with their partners, participant questionnaires were coded with three digits. The distribution of the questionnaires took place during the discharge process from the well-baby nursery. The questionnaire consisted of 26 questions and took approximately 5 minutes to complete. Hebrew and Arabic versions of the questionnaire were used. (Supplementary Data S1)
The study was approved by the Institutional Review Board (approval number: 0158-21-BNZ).
Study factors
The questionnaire centered on topics of religion and faith, ethnic origin, and early infant feeding from birth until discharge.
Questions 15–17 on the questionnaire were designed to evaluate the degree of religiosity among the participants. They help to assess the depth of religious or spiritual conviction held by the respondent, understand the individual’s overall religious orientation or affiliation, and assess the regularity of participation in religious ceremonies or events. Jewish women may participate in synagogue services, observe rituals such as lighting Shabbat candles, and recite prayers. In Islam, women may engage in daily prayers, attend Friday congregational prayers, and participate in Ramadan gatherings. Christian women may attend Sunday worship, join prayer groups, and take part in ceremonies such as baptism. Recognizing the frequency of women’s religious involvement sheds light on their commitment to faith and cultural traditions.
Level of faith was presented as a continuum from 1 to 5, and the three categories of religiosity included “religious,” “traditional,” or “secular.” Frequency of participation in religious ceremonies was recorded.
Infant feeding practices were categorized as exclusive breastfeeding, partial breastfeeding (a combination of breastfeeding and formula feeding), or exclusive formula feeding.
In Israel, the majority of the population (around 74%) is Jewish of different ethnic origins (such as “Ashkenazi” and “Sepharadic”). Arabs constitute around 21% of the population, and most are Muslim (around 83%). Other smaller groups are Arab Christians and Druze. We collected data on the participants’ “religion” (e.g., Jewish, Muslim, Christian), ethnic groups (i.e., Jews, Arabs), and origin groups within ethnic groups (e.g., Ashkenazi Jews, Sepharadic Jews). In addition, the survey explored various demographic and clinical data, including family status, education level, employment status, average monthly income, birth count, gestational age, infant birth weight, childbirth delivery method, desire to breastfeed during pregnancy and the influence of breastfeeding consultants on maternal feeding decisions. Place of residence was collected and converted later to an estimate of socioeconomic status (SES) by using the database of the Central Bureau of Statistics in Israel. The questionnaire, translated into English, appears in the appendix.
Data analysis
Differences among categorical variables were assessed using the Chi-square test. For ordinal variables, Kruskal–Wallis one-way analysis of variance on ranks was performed.
Variables that demonstrated either significant or trend association with present infant feeding were further analyzed in a univariate model, in which odds ratios (ORs) with a 95% confidence intervals (CIs) were calculated to estimate the impact of each independent variable on exclusive breastfeeding and any breastfeeding (encompassing exclusive and partial breastfeeding).
Multiple logistic regression model included the variables that exhibited significance or trend in the univariate analysis. Because of the study question, religiosity was forced into all models, even if no significant association was found in the univariate analysis.
We set our threshold for statistical significance at p < 0.05, and a p value of < 0.10 was considered indicative of a trend that justifies inclusion in the multivariate model. Data collected from the questionnaires were entered into a Microsoft Excel spreadsheet (Microsoft Office, Seattle, WA), and subsequent statistical analyses were conducted using SigmaPlot, version 11.0 (Systat Software Inc. San Jose, CA) and Minitab®, version 16.2.2 (Minitab Inc. State College, PA & Coventry, UK).
Results
Five hundred and fifteen participants completed the questionnaire, with 490 of them providing information on their present infant feeding practices that could qualify for inclusion in the statistical analysis. Not all participants answered every question, resulting in a varying number of participants for different variables. Of the responders, 431 were mothers, and only 59 were fathers. The characteristics of the questionnaire respondents are outlined in Table 1.
Characteristics According to Infants’ Feeding Group
χ2-results presented as number (percent %).
Kruskal–Wallis one-way analysis of variance on ranks—results presented as median (interquartile range: 25%, 75%).
Significant differences in early infant feeding were observed among mothers with different categories of religiosity (p < 0.001), as depicted in Table 1 and Figure 1. Both religious and secular groups displayed a higher tendency for exclusive breastfeeding compared with the traditional group, which predominantly favored a combination of breastfeeding and formula. Frequency of participation in religious ceremonies did not affect feeding practices.
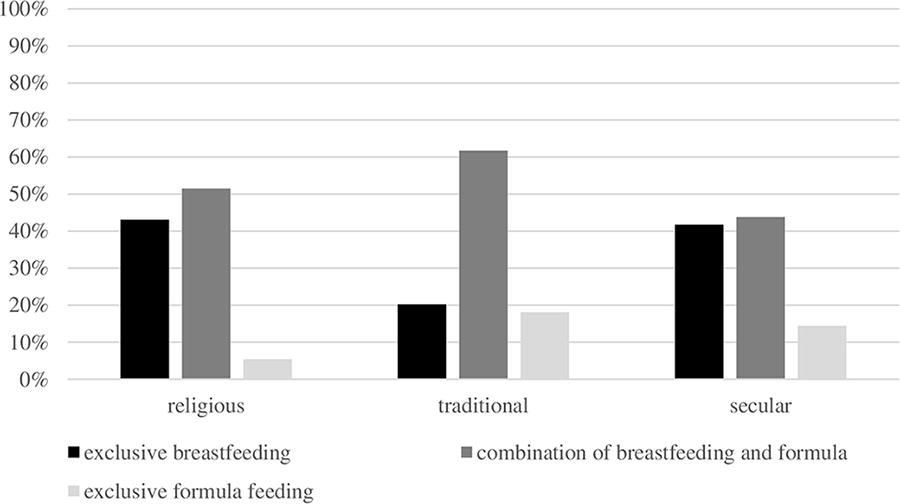
Religiosity and infant feeding practice.
Delivery mode was also significantly associated with feeding practices (p = 0.003) (Table 1), as illustrated in Figure 2. Mothers of infants delivered via vacuum extraction or cesarean section exhibited a reduced inclination toward exclusive breastfeeding when compared with those born through vaginal delivery.
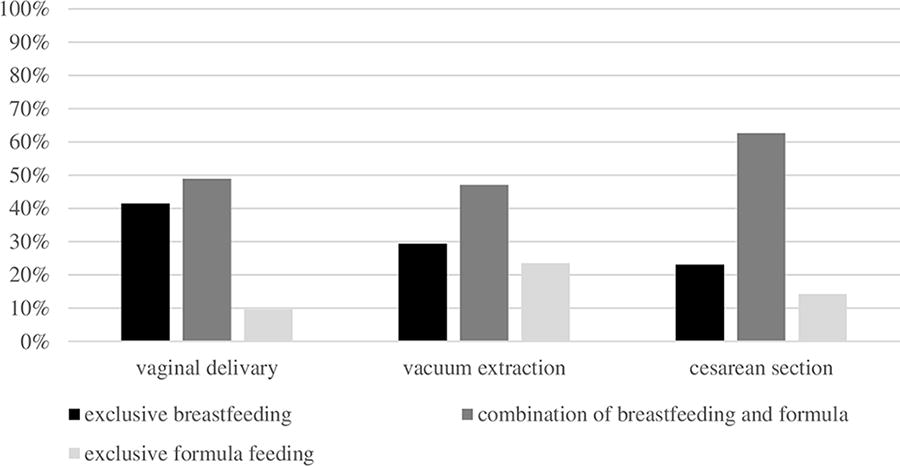
Mode of delivery and infant feeding practice.
There was a statistically significant positive correlation between a higher level of maternal education and a greater inclination toward breastfeeding (p = 0.005) (Table 1), as shown in Figure 3. Mothers who had not completed high school appeared to deviate from this trend, however, there was a very small sample of this group in this cohort (n = 2). Paternal level of education did not affect feeding practices.
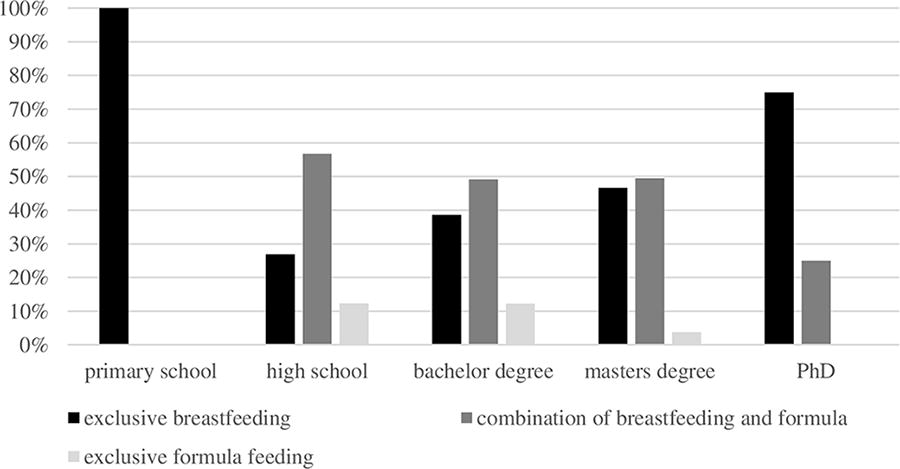
Maternal education and infant feeding practice.
As expected, mothers who expressed an intention to breastfeed during pregnancy were more likely to follow through with any breastfeeding compared with those who did not have this specific intention before delivery (p < 0.001) (Table 1).
Comparing feeding practices between Jews and Arabs revealed that Jewish mothers exhibited a higher preference for exclusive breastfeeding (p = 0.001), whereas the majority of Arab mothers preferred a combination of breastfeeding and formula feeding, as depicted in Figure 4. No significant differences were found among different Jewish origins (Ashkenazi, Sephardic, and others) or among different Arab origins (p > 0.05). No difference was found when comparing all religions (p > 0.05) (Table 1).
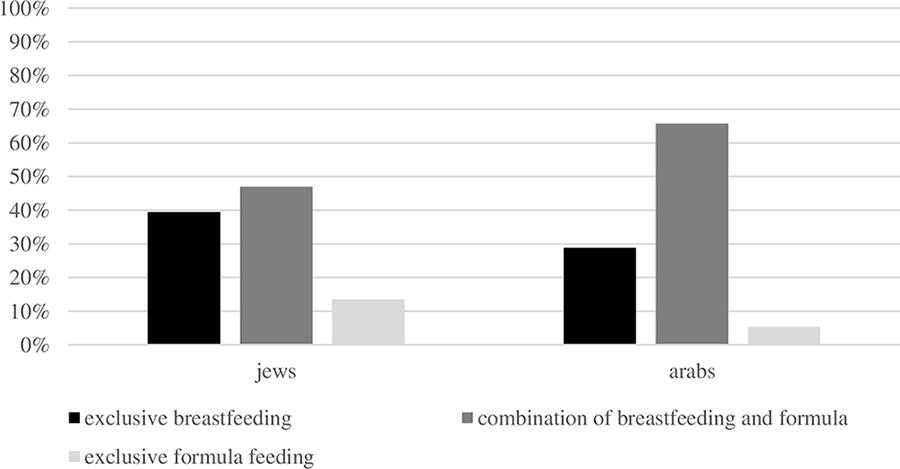
Differences between Jews and Arabs regarding infant feeding practice.
Other demographic factors, including family status, maternal age, partner’s age, employment status, average monthly salary, SES, infant’s gender, gestational age, infant’s birth weight, and age of the youngest child in the family before the present delivery, were not associated with statistically significant differences in early feeding practices (p > 0.05).
In a univariate model examining factors affecting exclusive or any breastfeeding, maternal education, birth number, mode of delivery, and the absence of desire to breastfeed during pregnancy were significantly associated with exclusive breastfeeding. Absence of desire to breastfeed and religiosity were significantly associated with any breastfeeding (Table 2).
The Odds for Exclusive or Any Breastfeeding by Factors Associated with It a
Factors (characteristics) that were found to have significant (p < 0.05) or trend (p < 0.10) association to present infant feeding (Table 1) were studied in this univariate model.
OR, odds ratio; CI, confidence interval.
In a multiple logistic regression model using the factors found to be significant in the univariate model, maternal education years (OR 1.59; 95% CI 1.09–2.32; p = 0.017), age of youngest sibling (OR 0.56; 95% CI 0.32–0.98; p = 0.041), delivery via cesarean section (OR 0.64; 95% CI 0.44–0.94; p = 0.023), and the absence of a pre-existing desire to breastfeed (OR 0.67; 95% CI 0.57–0.80; p < 0.001) were all identified as significant factors influencing exclusive breastfeeding. In addition, maternal education years (OR 2.21; 95% CI 1.09–4.46; p = 0.027), cesarean delivery (OR 0.50; 95% CI 0.28–0.89; p = 0.018), and the absence of a pre-existing desire to breastfeed (OR 0.46; 95% CI 0.36–0.60; p < 0.001) were also found to significantly impact any breastfeeding (Table 3).
Multiple Logistic Regression Model of Factors Associated with Exclusive or Any Breastfeeding a
Factors that were found to have significant (p < 0.05) or trend (p < 0.10) association to exclusive or any breastfeeding (Table 2) were entered into the multiple logistic regression model. Because of the subject of this study, religiosity was forced into all models (even if no significant association was found in the univariate analysis).
OR, odds ratio; CI, confidence interval.
Discussion
This study investigated the association between religious beliefs and early feeding practices of neonates in the Haifa district and Sharon plain in Israel. Israel has a very diverse population, encompassing various religious groups such as Jews, Muslims, Christians, and Druze. According to data from the Central Bureau of Statistics in Israel, for the year 2020, the country’s population comprised 74.04% Jews, 17.94% Muslims, 1.93% Christians, and 1.58% Druze. 26 Focusing on Haifa, a culturally diverse city where most of the research data were gathered, the population in 2020 consisted of 85.6% Jews, 5.96% Muslims, 5.83% Christians, 0.168% Druze, and the remaining residents belonged to various other minority groups. 27 In the Sharon plain, the population in 2020 consisted of 73.9% Jews, 21.43% Muslims, and the remaining belonged to other minorities. 28 Within each of these groups, there is a spectrum of religiosity, spanning from secular to religious.
When examining the influence of maternal religious concepts and beliefs on early breastfeeding, we identified that the level of religiosity and the intention to breastfeed during pregnancy play pivotal roles. Our findings revealed that both religious and secular mothers exhibited the greatest inclination toward exclusive breastfeeding compared with traditional mothers. This is an interesting finding, as mentioned earlier, prior knowledge indicated that women with higher levels of religiosity tended to breastfeed more than their less religious counterparts.18,19 We also mentioned a previous study, where it was found that ultra-orthodox Jewish mothers initiated breastfeeding more than secular/traditional mothers. 19 However, the authors included both secular and traditional mothers in the same group, and the level of religiosity was only examined within the Jewish population, whereas our study referred to religiosity across all religions included. Of note is that when we included the variable of religiosity in a model using ORs, its significance diminished. This may be explained by the fact that both extremes of this variable were associated with exclusive breastfeeding. When considering such a variable as an ordinal factor, its impact becomes less discernible. The effect of a high level of religiosity on exclusive breastfeeding may be explained by the strong endorsement of breastfeeding by the “Talmud” (the basis for the Jewish religious legal code) and the “Koran” (the main text of the Muslim religion) as well as the advantage of controlling birth intervals by lactational amenorrhea.29,30 However, the high rate of breastfeeding in secular mothers is less intuitive and was not described before. It may be related to the fact that secular mothers in our population had a higher level of education (61% academic degrees among religious mothers versus 83% among secular mothers), which may contribute to increased breastfeeding.
We found a significant difference in feeding practices between Jews and Arabs, with Jewish mothers exhibiting a higher exclusive breastfeeding rate than Arab mothers. Overall past breastfeeding rates in Israel were higher than the rates in this cohort. We speculate that the decline in overall exclusive breastfeeding rates and especially in the Arab population in our cohort reflects a national trend in Israel,25,31 perhaps related to an increase in women employment over the years, aggressive marketing of formulas such as “breast milk substitutes” and increased rates of cesarean sections.
Maternal education level and the mode of delivery had a notable impact on early infant feeding practices in our cohort. Our results demonstrated that a higher level of maternal education was associated with a stronger preference for breastfeeding, a trend that aligns with findings from previous research studies.19,32,33 This association can be attributed to several factors, including improved access to information, the presence of supportive social networks, and a deeper understanding and knowledge of the health benefits associated with breastfeeding.
Regarding the mode of delivery, our study indicated that mothers who underwent cesarean section were less inclined to breastfeed, consistent with findings in the literature. 33 This phenomenon can be attributed to various factors such as an extended recovery period, delayed initiation of breastfeeding, limited opportunities for early skin-to-skin contact that interrupt initial bonding, and the psychological impact of the surgical experience itself.
Another interesting finding was that a shorter age gap between the newborn and his/her youngest sibling was linked to an increased probability of exclusive breastfeeding. This connection may stem from the mother’s recent breastfeeding experience, had it been successful, which may boost her confidence and satisfaction in breastfeeding, and provide easier access to breastfeeding support networks.
Various worldwide initiatives to enhance breastfeeding practices have been launched, with Israel also actively participating in this effort. In the United States, the Healthy People 2010 initiative established several breastfeeding targets, including a goal for 75% of the new mothers to begin breastfeeding, with 50% continuing for a minimum of 6 months and 25% continuing for a year. In addition, the aim was for 40% of the infants to be exclusively breastfed for 3 months, and 17% exclusively breastfed for 6 months. However, only the first goal of initiation of breastfeeding by 75% of new mothers was achieved. 34 Following this, the Healthy People 2020 initiative introduced a new objective as follows: for 82% of infants to experience breastfeeding at some point, with 61% continuing for at least 6 months, and 25.5% being exclusively breastfed up to 6 months of age. Looking ahead to Healthy People 2030, the United States aims to raise the proportion of infants exclusively breastfed to 42.4% and to increase continued breastfeeding through the first 12 months to 54.1%. Notably, while breastfeeding initiation rates are markedly high in the United States, the majority of women neither exclusively breastfeed for the full first 6 months, nor do they continue to breastfeed throughout the entire first year. 35
Beginning from 2016, Israel has been compiling breastfeeding data through the “Healthy Thought” system, covering roughly 65% of the nation’s children. As per these data, 92% of newborns are breastfed at least once immediately after birth, with 50% of them being exclusively breastfed at the age of 1 month. Around 30% of mothers maintain exclusive breastfeeding up until the 6-month mark. Unfortunately, the data reveal a gradual decrease in breastfeeding rates over the years. 31
The primary strengths of this study are exploring the issue of religiosity within the diversity of our population, which encompassed various religious backgrounds and varying levels of religiosity within each group, and capturing reliable feeding data at the time discharge from the hospital so that parents had to recall only the 2–3 last days since the delivery, minimizing recall bias.
This study has several limitations. The study results rely on patient self-reporting and does not stem from direct observational data. However, in its essence, religious and spiritual belief is self-defined and mostly self-reported and it cannot be measured in a completely objective manner. To decrease the bias of self-report on religiosity, our questionnaire included an objective measure of frequency of attending religious ceremonies. Furthermore, it is essential to acknowledge the potential for selection bias. Although equally approached for participation in the study, mothers who did not breastfeed their infants were less likely to participate in the study compared with those who did breastfeed. Unpublished data from Bnai Zion Hospital examined the feeding practices of newborns before their discharge, revealing that 15% of the infants were exclusively breastfed, 64% received partial breastfeeding, and 21% were exclusively formula-fed. In contrast, our study found rates of 37.14%, 51.43%, and 11.43%, respectively. Although we aimed to record both parents’ effects of religiosity on breastfeeding practices, the majority of our respondents (87.8%) were mothers (430 out of 490), and the few fathers that filled-in the questionnaire were actually doing so for their wives, thus probably describing also maternal attitudes and beliefs. Thus, our study actually reflects only Israeli mothers’ attitudes toward breastfeeding and their relation to their level of religiosity, as outlined in the title of this article.
In summary, we found that in the Israeli population, we studied that both religious and secular mothers exhibited a higher inclination toward exclusive breastfeeding compared with traditional mothers. The study indicated that along with the level of religiosity, maternal education, age of the youngest sibling, delivery mode, and prenatal intention to breastfeed influenced breastfeeding practices. These findings may aid in developing and implementing strategies aimed at increasing the breastfeeding rates, especially in populations with lower rates of breastfeeding initiation.
Footnotes
Acknowledgments
This work was performed by S.A in partial fulfillment of the MD thesis requirements of the Technion’s Rappaport Faculty of Medicine, Haifa, Israel. The authors are grateful to the multidisciplinary team of dedicated nurses, breastfeeding consultants, psychosocial workers, and physicians in the departments of neonatology at Bnai Zion Medical Center and Laniado Medical Center.
Authors’ Contribution
H.Z., A.G., A.T., and A.R.: Conceptualization, methodology, and software. S.A., H.Z., and A.S.: Data curation. A.R.: Statistical analysis. S.A. and H.Z.: Writing—original draft preparation. S.A. and A.G.: Visualization and investigation. A.R. and A.G.: Software and validation. A.G., A.T., and A.R.: Supervision and writing—reviewing and editing.
Author Disclosure
All authors have nothing to disclose.
Conflict of Interests
All authors declare no conflict of interests.
Funding Information
None to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.