
Abstract
Background:
Gestational weight gain (GWG) may be associated with delayed onset of lactogenesis II (DOL II), but it is still unclear and controversial.
Object:
The study aims to evaluate the relationship between GWG and DOL II.
Methods:
A comprehensive search was performed in 10 electronic databases from inception to May 21, 2023, for studies that reported outcomes in breastfeeding. Data were extracted by two independent reviewers. A meta-analysis was conducted to calculate the pooled estimates of association using random-effect models with Review Manager (RevMan) software version 5.4. The primary outcome was the rate of DOL II.
Results:
In this study, 248,515 women were included in 16 eligible articles. Women with excessive GWG have a higher risk of DOL II (odds ratio [OR] = 1.28; 95% confidence interval [CI]: 1.15–1.43). Specifically, prepregnancy overweight and obese women with GWG above recommendations (OR = 3.01, 95% CI: 1.38–6.57) and underweight women with excessive GWG before pregnancy have a higher risk of DOL II (OR = 3.32, 95% CI: 1.69–6.53). Nonetheless, there is no distinction between women with inadequate GWG and those with adequate GWG in DOL II(OR = 1.08, 95% CI: 0.88–1.33). In addition, the women whose GWG is above the recommendations also tend to stop exclusive breastfeeding 1 month postpartum (OR = 0.82, 95% CI: 0.80–0.85).
Conclusion:
Excessive GWG has a negative influence on the timing of the onset of lactogenesis and exclusive breastfeeding within 1 month postpartum.
Introduction
Breastfeeding is the most ideal mode of feeding advocated all over the world, which is an essential part of the 17 sustainable development goals. It has both long-term and short-term benefits for women and children. The World Health Organization and the United Nations Children’s Fund advocate exclusively breastfeeding newborns for 6 months after birth and continuing breastfeeding until the age of 2 years or older. 1 However, the global situation of breastfeeding is not optimistic. A global survey 2 showed that among 57 low- and middle-income countries from 2010 to 2018, the exclusive breastfeeding rate for those under 6 months was 45.7% whereas the exclusive breastfeeding rate for those between 4 and 5 months was 32.0%. The figures for Eastern Mediterranean and Europe reached 34.5% and 43.7%, respectively.
Among the many factors that affect breastfeeding, delayed onset of lactogenesis II (DOL II) is an important one. DOL II is defined as the copious milk secretion that occurs more than 72 hours postpartum, which is usually measured by maternal perception of breast hardness, fullness, or leakage of breast milk. 3 In an earlier longitudinal study, 4 it was found that women who experienced DOL II had shorter periods of breastfeeding. Meanwhile, a study involving 2,491 people in the United States also found that women who experienced DOL II may not be able to maintain any breastfeeding or exclusive breastfeeding in the early postpartum period. 5
With the obese population increasing, there is a growing concern about the effects of weight on people’s bodies. Pregnancy, as a unique period in a woman’s life, naturally draws attention. Some researchers found inappropriate gestational weight gain (GWG) is associated with many pregnancy complications 6 including preterm birth, gestational diabetes, fetal growth restriction, and influences on the decision to begin or continue breastfeeding. 7
Lactogenesis stage II is considered the key to the success of early exclusive breastfeeding. 5 We’re trying to determine whether there was a relationship between the GWG and DOL II, but it turned out to be controversial. Some studies8–9 found there was no relationship between them, but Haile’s study 10 discovered that 73.2% of women with DOL II had inappropriate GWG.
We conducted this study to explore the relationship between DOL II and GWG to investigate whether pre-pregnant women with different body mass index (BMI) may have different effects on lactation initiation depending on their GWG, this could provide better weight guidance for pregnant women.
Methods
The protocol for this systematic review was developed using the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) protocol. 11 This systematic review was prospectively registered with PROSPERO International Prospective Register of Systematic Reviews (PROSPERO identifier CRD42023418908). All data came from published articles; thus, ethical approval was not required for this study.
Study eligibility criteria
We included studies that investigated the association between GWG (the exposure of interest) and DOL II or breastfeeding, and limited the types of studies to cohort, case-control, and cross-sectional studies published in all languages.
P: Postpartum women E: Inappropriate GWG in pregnancy C: Adequate GWG in pregnancy O: the occurrence of DOL and the outcomes of breastfeeding exclusive criteria
1. Unable to obtain full text and data cannot be available or converted; 2. Review, abstract, and conference papers; 3. Repeated publications; 4. Literature with a low-quality evaluation.
Search strategy
Ten electronic databases were systematically searched to find articles that meet the eligibility criteria: PubMed, Embase, Cochrane Library, Web of Science, Scopus, Ovid, Wangfang Data, China National Knowledge Infrastructure Database, Chinese Scientific Journal Database, and Chinese Biomedical Database. The retrieval strategy was developed with a combination of free and MESH words and adapted to different databases. Those words were as follows: (Weight Gain Pregnancy OR Maternal Weight Gain OR Pregnancy Weight Gain OR Gestational Weight Gain OR Weight Retention OR Postpartum Weight Retention) AND [(“lactation” OR “lactogenesis” OR “lactation disorder*” OR “hypogalactia*” OR “galactorrhea*” OR “galactorrhoea” OR “lactic Secretion*” OR “milk excretion” OR “breast secretion*” OR “milk production” OR “milk secretion*” OR “milk release” OR “mammary gland secretion*” OR “lactorrhea” OR “DOL”)]. All the databases were searched from inception to May 21st, 2023, and there are no language restrictions.
Study selection
The retrieved literature we managed and de-duplicated using the Endnote20 version. We ensured that there were no duplicate entries by manually removing them. Two trained reviewers (Z.C. and J.Y.) conducted the initial screening of abstracts. Eligible studies were screened after full-text review and then assessed for quality. Any discrepancies between the two reviewers were resolved via consensus, and if necessary, a third reviewer (Huang) joined the discussion. The entire process of literature screening was completed independently by two reviewers.
Data extraction
Data were extracted from eligible studies by two reviewers (Z.C. and J.Y.) independently. The following information was collected: name of the first author, year of study, study design, study population and participant characteristics, sample size, definitions, categories of GWG, and the method of measuring lactogenesis onset. If data were duplicated, then only the data from the study with a larger sample size were extracted. If the data were unclear, the third reviewer (M.H.) contacted the authors by email.
Outcome
The primary outcome was the rate of DOL II.
The secondary outcomes were as follows:
Unsuccessful breastfeeding initiation Exclusive Infant feeding at discharge Exclusive breastfeeding at 1 month postpartum Exclusive breastfeeding at 3 months postpartum Exclusive breastfeeding at 6 months postpartum Exclusive Breastfeeding Duration NICU (neonatal intensive care unit) admission
Definitions
Categories of BMI were defined based on the WHO recommendations: underweight, <18.5 kg/m2; normal weight, 18.5–24.9 kg/m2; overweight, 25–29.9 kg/m2; and obese, ≥30 kg/m2. Fifteen articles used the current institute of medicine (IOM) recommendations which were written in 2009 for GWG in gestations: 12.5–18.0 kg for women of underweight;11.5–16.0 kg for normal weight, 7.0–11.5 kg for overweight women and 5.0–9.0 kg for obese women. 12 But one article defined categories of BMI and GWG based on the Chinese classification: underweight, <18.5 kg/m2, recommended weight gain 15.0–22.0 kg; normal weight, 18.5–23.9 kg/m2, recommended weight gain 13.0–21.0 kg; overweight, 24–27.9 kg/m2, recommended weight gain 10.0–18.0 kg; and obese, ≥28.0 kg/m2, recommended weight gain 9.5–17.0 kg.13–14 Weight gain above/within/below the guidelines was defined as excessive/adequate/inadequate GWG. For maternal pre-regnancy weight and height, we accepted self-reported or measured values obtained during the first prenatal examination. For weight at birth, we accepted self-reported or the last measurement during pregnancy.
Quality assessment
The quality of eligible studies was appraised using the Newcastle–Ottawa Scale (NOS), 15 which is an effective tool for assessing the quality and sensitivity of observational studies. The NOS consists of nine items, with scores categorized as high quality (7–9 points), medium quality (5–6 points), and low quality (<5 points). For cross-sectional studies, we used the Agency for Healthcare Research and Quality (AHRQ) scale 16 which comprises 11 items. Scores are graded as high quality (8–11 points), moderate quality (4–7 points), and low quality (0–3 points). In cases where the research design was ambiguously reported, we determined whether it was a prospective or retrospective study based on the duration of the study and when breastfeeding outcomes were collected.
Data analysis
The associations of GWG with breastfeeding outcomes were described in each study. The pooled OR with 95% CI is was presented to explain the meta-analysis results of the association. GWG and most outcomes are binary variables represented by OR and 95% CI. For continuous variables, if data is analyzed using the same measurement tool, use the mean difference (MD). Otherwise, we used the standardized MD and calculated 95% CI. In addition, we calculated the association of inadequate or excessive GWG with breastfeeding outcomes for the studies using random effects. Specifically, we categorized GWG below or above recommendations, using GWG within recommendations as a reference, using the WHO BMI categories. We chose the random effects model for this meta-analysis owing to anticipated heterogeneity between the study population, time, DOL measurement, and prenatal care studies. Heterogeneity was assessed using the I2 statistic. For substantial heterogeneity (I2 > 50%), we plan to conduct a sensitivity analysis using a case-by-case elimination method. All analyses were two-tailed, and results were considered significant if the p value was <0.05. The meta-analysis was performed by using Review Manager (RevMan) software version 5.4 provided by Cochrane Collaboration Network. 17
Results
Study selection
A total of 8,814 studies were identified by the search. Following the removal of duplicates, 6,011 titles and abstracts were screened. Seventy-four studies were selected for full-text review, and 16 studies,8,10,13,14,18–29 involving 248,515 women, met our eligibility criteria and were included in the systematic review (PRISMA Flow Diagram Fig. 1). Of those, 12 studies8,10,14,18–21,24–26,28,29 analyzed GWG with the IOM recommendations, while one study 13 analyzed GWG with Chinese classification.

PRISMA Flow Diagram. PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis.
Study characteristics
The characteristics of the 16 eligible studies are presented in Table 1. Among these, there were four18,19,28,29 retrospective cohort studies, six8,13,23–26 prospective studies, two10,21 longitudinal studies, and four14,20,22,27 cross-sectional studies. The studies were conducted in various countries, including six studies10,18–20,22,28 were from the United States, six8,13,14,21,24,25 from China, two26–27 from Brazil, one 29 from Japan, and one 23 from Norway. The sample size ranged from 294 to 173,603 women. Nearly all studies considered GWG as a categorical variable (below versus within versus above guidelines, or below versus within/above guidelines), with 15 of these studies using the IOM guidelines, and one using the Chinese classification. In additon, 14 studies used the WHO guidelines about BMI, and two studies used the Chinese classification. Two of 16 eligible studies were restricted to the obese categories. All 16 studies provided information on the proportion of women who gained weight below or above the recommendations. Overall, 68.3% of women experienced inappropriate gestational weight gain: 26.5% and 41.8% gained weight below and above recommendations, respectively.
General Characteristic and Quality Assessment of Included 16 Articles
Means these studies we used Newcastle–Ottawa Scale (NOS) to assess their quality according to their study design.
The World Health Organization (WTO) classifies BMI as normal (18.5–24.9 kg/m2), underweight (BMI < 18.5 kg/m2), overweight (BMI 25.0–29.9 kg/m2), obese (BMI ≥ 30 kg/m2).
IOM: The Institute of Medicine (IOM) 2009 guidelines, recommended GWG “underweight” (recommended weight gain 12.5–18 kg), “normal weight”(recommended weight gain 11.5–16 kg), “overweight” (recommended weight gain 7–11.5 kg), and “obese” (recommended weight gain 5–9 kg). Based on this guideline GWG was classified as “inadequate,” “adequate,” and “excessive.”
Chinese classification as underweight (<18.5 kg/m2), normal weight (18.5–23.9 kg/m2), overweight (24.0–27.9 kg/m2), and obese (≥28.0 kg/m2).
Chinese guideline aims to recommend GWG “underweight” (recommended weight gain 15.0–22.0 kg), “normal weight” (recommended weight gain 13.0–21.0 kg), “overweight” (recommended weight gain10.0–18.0 kg), and “obese” (recommended weight gain 9.5–17.0 kg). Maternal GWG categories were then defined as excessive, adequate, and inadequate weight gain.
BMI, body mass index; GWG, gestational weight gain.
As for quality assessment, the scores of the included studies ranged from 5 to 8 points, and the average score was 6.94 points. Nine studies were assessed as high quality, and seven studies were assessed as medium quality. More details of characteristics are depicted in Supplementary Data.
Primary outcome
Delayed onset of lactogenesis II.
Seven studies8,10,13,14,21,24,25 reported DOL II, all of which used maternal perception to determine the onset of lactogenesis. Five studies8,10,21,24,25 defined GWG based on the IOM guidelines and two studies13–14 based on the Chinese guidelines.
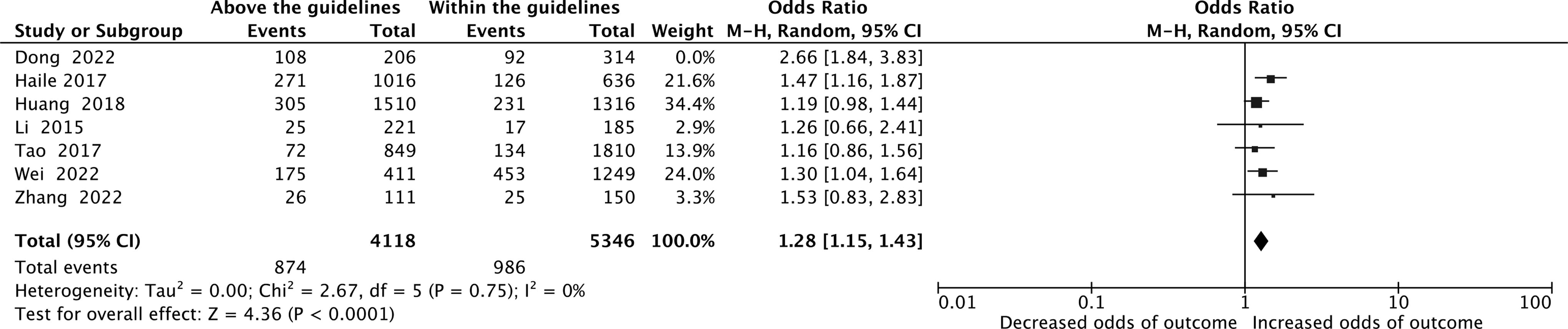
The differences in the rate of DOL II among women who gained weight below compared with those who gained weight within guidelines were relatively slight for the outcome of DOL II. GWG below the guidelines had an overall weak association with DOL II in all BMI categories groups (odds ratio [OR], 0.97; 95% confidence interval [CI]: 0.67–1.39; I2 = 83%, Z = 0.18, p = 0.86, Fig. 2). Sensitivity analysis revealed that high heterogeneity was influenced by Wei’s literature. 24 After its removal, heterogeneity decreased (OR, 1.08; 95% CI, 0.88–1.33; I2 = 27%, Z = 0.77, p = 0.44, Fig. 3). This discrepancy may be attributed to demographic factors, as Wei’s study 24 had a higher proportion reaching 56.5% of women over 35 years old, which can affect lactogenesis II onset. 30 Besides, there was also less association with DOL II in both the underweight and overweight/obesity groups with inadequate GWG (OR,1.98; 95% CI, 0.96–4.12; I2 = 0%, Z = 1.84, p = 0.07, Fig. 4). In contrast, GWG above the recommendations had a stronger association with DOL II when pooled across all BMI groups (OR,1.43; 95% CI, 1.17–1.73, I2 = 64%, Z = 3.55, P < 0.01, Fig. 5). Sensitivity analysis showed that Dong’s study 14 caused high heterogeneity, which stabilized after its removal (OR,1.28; 95% CI, 1.15–1.43, I2 = 0%, Z = 4.36, P < 0.01, Fig. 6). Dong’s study 14 included many pregnant women who give birth before full-term, leading to some differences from other studies. Furthermore, the underweight group and the group of overweight and obesity with excessive GWG also have close connections with DOL II (OR, 3.19; 95% CI: 1.91–5.31; I2 = 0%, Z = 4.45, P < 0.01, Fig. 7).
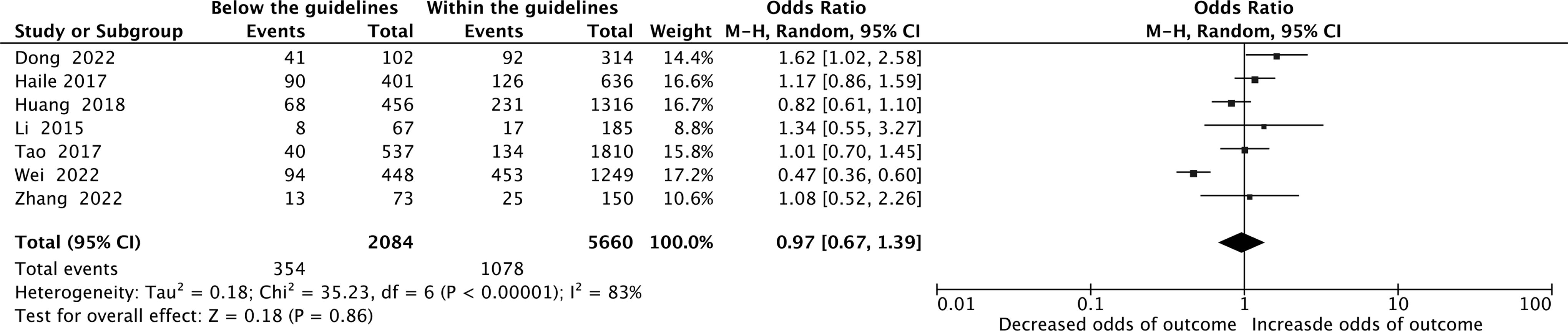
Below the guideline versus within the guideline Forest plot in DOL. DOL, delayed onset of lactogenesis.
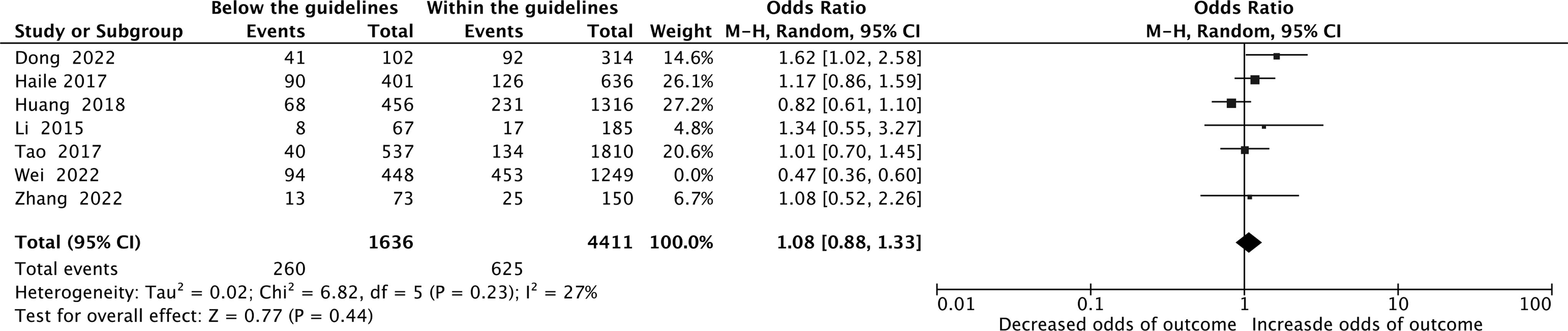
Below the guideline versus within the guideline Forest plot in DOL performing sensitivity analyze. DOL, delayed onset of lactogenesis.

Below the guideline versus within the guideline Forest plot in DOL. DOL, delayed onset of lactogenesis.
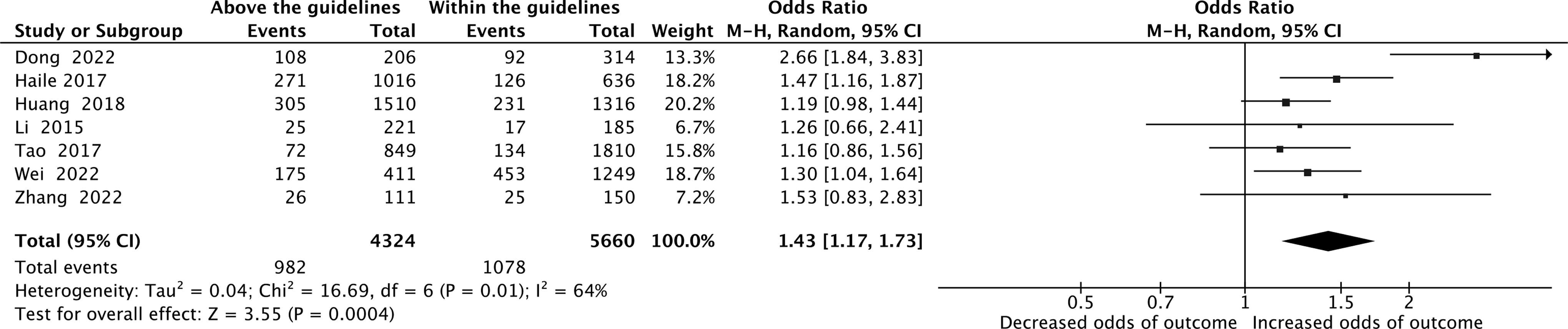
Above the guideline versus within the guideline Forest plot in DOL. DOL = delayed onset of lactogenesis.
Above the guideline versus within the guideline Forest plot in DOL performing sensitivity analyze. DOL = delayed onset of lactogenesis.
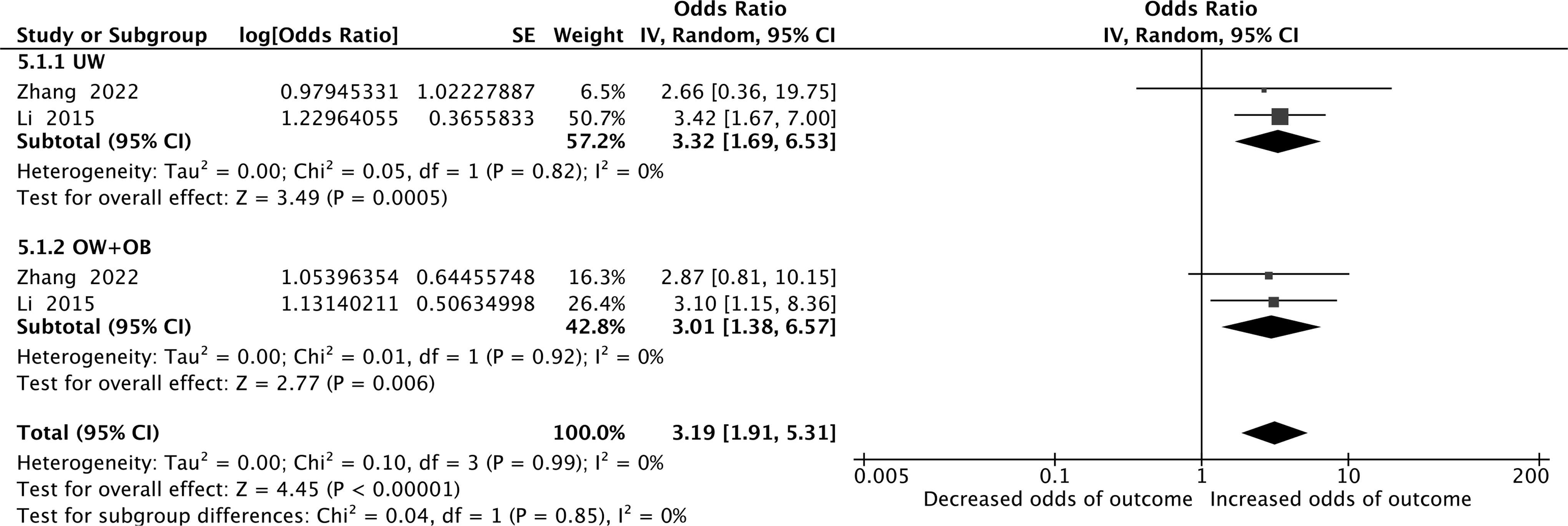
Above the guideline versus within the guideline Forest plot in DOL. DOL = delayed onset of lactogenesis.
Secondary outcomes
Unsuccessful breastfeeding initiation
Unsuccessful breastfeeding intention was assessed in two studies.22,23 Owing to the inconsistency in the extracted forms of the data for these two studies, it is not possible to conduct a meta-analysis. We can see in Martin’s study, 22 that 47.4% of women with inadequate GWG and 42.8% of women with excessive GWG experience unsuccessful exclusive breastfeeding initiation, while 61% of women with adequate GWG did so. Another study 23 reported that pre-pregnant women with inadequate GWG, and pre-pregnancy obese and overweight women with all categories of GWG are at a higher risk of unsuccessful breastfeeding initiation compared with normal-weight women with adequate GWG.
Exclusive infant feeding at discharge
There are four articles18,19,28,29 addressing the outcome of exclusive infant feeding at discharge. Two articles28–29 reported this outcome across all BMI categories, while the other two18–19 reported it based on pre-pregnancy obese women. One of these articles 18 categorized weight gain in obese women into those who gained weight excessively and those who did not, according to the IOM guidelines (i.e., those who gained weight inadequately and adequately). For analysis purposes, we divided the population’s weight gain during pregnancy into those who exceeded the standard and those who did not, then conducted a subgroup analysis on the obese population. We found that there was no significant difference in weight gain during pregnancy for exclusive breastfeeding at discharge (OR, 1.31; 95% CI, 0.88–1.94; I2 = 73%, Z = 1.34, p = 0.18, Supplementary Data). After sensitivity analysis, and then removing Darling’s study, 19 we got acceptable heterogeneity (OR, 1.12; 95% CI, 0.90–1.40; I2 = 0%, Z = 1.02, p = 0.31, Supplementary Data). At the same time, we extracted the data from the original two literature28–29 , and directly analyzed them. We found that there was also no significant difference in the breastfeeding situation at discharge whether it was above or below the pregnancy weight gain standard (OR, 0.78/0.91; 95% CI, 0.59–1.02 and 0.77–1.09; I2 = 0%/3%, Z = 1.80/1.02, p = 0.07/0.31, respectively, Supplementary Data).
Exclusive breastfeeding at one month postpartum
Only two studies20,29 discussed the exclusive breastfeeding rate at 1 month postpartum. We conducted a meta-analysis, and the results showed that the population with excessive weight gain during pregnancy had a higher risk of stopping engaging in exclusive breastfeeding than the population with adequate weight gain during pregnancy, as shown in Figure 8 (OR, 0.82; 95% CI, 0.80–0.85; I2 = 0%, Z = 14.05, p < 0.01). However, there was no significant difference in the exclusive breastfeeding rate between women with inadequate GWG and those with adequate GWG in the first month postpartum (OR, 1.01; 95% CI, 0.98–1.04; I2 = 0%, Z = 0.46, p = 0.64, Supplementary Data).

Above the guideline versus Within the guideline in exclusive breastfeeding at one month postpartum.
Exclusive breastfeeding at 3 months postpartum
Exclusive breastfeeding at 3 months postpartum was evaluated in three articles,20,22,26 but only two studies’ data20,26 can be used. Therefore, we conducted a meta-analysis of the data from these two articles. The results showed that regardless of whether the weight gain was above or below the IOM guidelines, there was no significant impact on exclusive breastfeeding after 3 months postpartum. The results are detailed in Supplementary Data. In contrast, in Martin’s study, 22 he found in comparison to women with normal pre-pregnancy BMI who gained weight within recommendations, there was a trend towards an increased risk of breastfeeding cessation by 3 months among all pre-pregnancy BMI categories of women who gained weight excessively (adjusted hazard ratio [95%CI]: normal BMI 1.32 [0.99–1.77]; overweight BMI 1.21 [0.90–1.65]; obese BMI 1.34 [0.91–1.98]).
Exclusive breastfeeding at 6 months postpartum
Only one study 23 described exclusive breastfeeding at 6 months postpartum. The results showed that compared with the group that had normal BMI and gained within the IOM, overweight, and obesity groups have a higher risk of inability to fully breastfeed at 6 months postpartum regardless of whether GWG is adequate or not. The risk of incomplete breastfeeding in people who are pre-pregnancy overweight or obese with GWG above the IOM guidelines after 6 months postpartum is 1.44 or 2.27 times higher than in the normal BMI group with GWG by IOM guidelines. The results are the same as Fernandes’, 27 women with inappropriate weight gain had a high risk of failure in the early stages of exclusive breastfeeding.
Exclusive breastfeeding duration
Exclusive breastfeeding duration was mentioned in two articles,22,26 but as one of the study’s data did not follow a normal distribution and could not be converted, the meta-analysis was not conducted on these two articles. The researcher, Castillo, 26 reported that there were no differences in the duration of any breastfeeding or exclusive breastfeeding according to GWG categories. In Martin’s 22 study, the median duration of exclusive breastfeeding (among those who initiated exclusive breastfeeding) was 90 days (interquartile range, 30–117), and the median duration of exclusive breastfeeding for women with excessive, adequate, and inadequate weight gain during pregnancy was 75 (interquartile range, 28–109), 98 (interquartile range, 42–120), and 90 days (interquartile range, 28–120), respectively.
NICU admission
Only one study 20 assessed NICU admission. In this study, 42.1% of women who gained weight above the IOM guidelines had their children admitted to the NICU. 28.2% of women with suitable weight gain had their children admitted to the NICU and 29.7% of women with inadequate weight gain.
Publication bias
Begg’s test was conducted according to the primary outcome of the association between GWG and DOL II to estimate publication bias, which suggested that no significant publication bias was detected (p = 0.548).
Discussion
Principal findings
In the current study, we aimed to describe and synthesize available data regarding the association between GWG and DOL. Our main findings in this analysis of 248,515 pregnancies were as follows:
Over half (67.5%) of the pregnant women did not adhere to the GWG recommendations with 26.2% gaining less than the recommended weight and 41.3% gaining more than the recommended weight. Women in the overweight or obese pre-pregnancy BMI groups were most likely to gain weight above guidelines. GWG above recommended value was associated with an increased risk of DOL II and stopping exclusive breastfeeding at 1 month postpartum across all BMI categories. GWG below the suggested level has minimal adverse effects on breastfeeding.
Results of the study in the context of existing literature
In current literature reviews, more attention has been paid to the impact of factors on lactation.30–31 With the increasing number of obese individuals, there is a growing awareness of the effect of obesity on lactation. However, relatively few people recognize the impact of weight gain during pregnancy on maternal and neonatal outcomes 32 (such as preterm birth, pre-eclampsia). In our study, we focus on the DOL and aim to provide a better guide for pregnant women. Our findings indicate that excessive GWG increases the risk of DOL II, particularly for pre-pregnancy obesity and overweight women. However, the precise mechanism through which excessive GWG impacts DOL II remains unclear. One possible explanation lies in the physiological differences observed in pre-pregnancy overweight and obese women, such as larger nipples. Women with a high BMI tend to have larger nipples, which can lead to the inability of infants to engage in timely and effective breastfeeding. 33 In addition, earlier research 34 has shown that obese women are more likely to experience nipple edema after childbirth, causing the nipples to flatten, which undoubtedly increases the difficulty of breastfeeding. If effective sucking, as an important way of prompting exclusive breastfeeding, cannot be satisfied, it will easily lead to DOL II. Biological factors might be more influential than psychosocial factors in Hillson’s study, 35 and they found that pregestational overweight and obese women have a reduced prolactin response at both 48 hours and 7 days postpartum. Besides, some hormones can also affect DOL II, like leptin, a protein hormone. Ren 36 found in late pregnancy that women who were overweight or obese before pregnancy had higher concentrations of leptin, which might have delayed the timing of onset lactogenesis. The probable mechanism is that excessive leptin levels would inhibit the secretion of baseline prolactin, prolonging the timing of the onset of lactogenesis compared with normal-weight women. Moreover, some researchers 37 discovered that breastfeeding practices (exclusive versus mixed), maternal pregestational BMI, and weight gain over pregnancy contributed to the milk microbiota variation. Pregestational normal-weight women with exclusive breastfeeding habits harbored a significantly higher abundance of Bifidobacterium genus. Maternal pre-pregnancy BMI was associated with human milk components. 38 Finally, the disorders of thyroid hormones, insulin, and glucocorticoids in obese women reflect their regulation of milk secretion. 39 GWG over recommended levels can exacerbate these consequences. Thus, it is necessary to keep a healthy pre-gestational BMI and appropriate weight gain.
Strengths and limitations
To the best of our knowledge, this is the first systematic review and meta-analysis to synthesize evidence on the association of GWG about the IOM guidelines or Chinese recommendations with DOL II. In addition, inclusion criteria in the meta-analysis considered methodological flaws, which are a common and important source of bias in many of the studies on GWG. Finally, this study provides information on crucial clinical practice in women across all BMI groups.
However, this review has some limitations. Some outcomes were assessed in only one or two studies, limiting the ability to synthesize data. In addition, all studies included in this review were observational, with some having relatively small sample sizes and failing to account for potentially confounding variables. Owing to the limited number of studies available for quantitative analysis, we could not stratify results into subgroups for certain outcomes. Besides, some studies only presented outcomes across all BMI categories rather than within each BMI group, making it challenging to conduct subgroup analysis and resulting in a lack of more detailed analysis of specific outcomes, such as the impact of different gestational weight gain in different BMI groups on outcome.
Conclusion
In the current study, we identified and quantified the association between inappropriate GWG and the risk of DOL II. The importance of these findings is underlined by the fact that over half of pregnant women experience inappropriate GWG. According to this, GWG may be a significant modifiable risk factor for DOL II and other adverse breastfeeding outcomes. Further prospective research is warranted to investigate the effects of underweight women before pregnancy on delayed lactation and breastfeeding during pregnancy weight gain.
Footnotes
Authors’ Contributions
C.Z.Y.: study conception and design; literature search, data collection; review and editing; writing—original draft; formal analysis. H.M.: conceptualization (lead); writing—review and editing (equal). C.Y.: interpretation of the data and revising of the article (leading). Y.J.: literature search, data collection. L.Y.: writing—review and editing (equal). L.B.: writing—review and editing (equal). P.J.: writing—review and editing (equal). L.C.: technical support.
Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
The study was funded by the project of Guangzhou Teaching Achievement Cultivation from Guangdong Lingnan Nightingale Nursing Research Institute and Guangdong Nursing Association in 2023 [No.YJYZ202306].
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.