
Abstract
Background:
Breast milk is vital for the growth and development of preterm infants. However, in Neonatal Intensive Care Units (NICUs), mothers often encounter significant challenges in breastfeeding.
Objective:
This study aims to systematically evaluate the barriers to breastfeeding in NICUs, thereby providing evidence-based support for clinical practices.
Methods:
A comprehensive search was conducted in the Cochrane Library, PubMed, Web of Science, Embase, and Scopus databases, up to September 2023. Meta-analysis was performed using Stata 15.0, applying fixed or random effects models to calculate odds ratios (OR) and their 95% confidence intervals (CI). Study quality was assessed using the Newcastle–Ottawa Scale for cases and cohorts and the Agency for Healthcare Research and Quality standards for cross-sectional studies. Heterogeneity was evaluated using Cochran’s chi-squared test (Cochran’s Q) and I2 statistics, and publication bias was assessed through funnel plots and symmetry tests.
Results:
A total of 32 studies were included, encompassing 96,053 preterm infants. The main barriers to breastfeeding in preterm infants included: low gestational age (OR = 1.36, 95% CI: 1.06–1.75), lower maternal education (OR = 1.64, 95% CI: 1.39–1.93), insufficient breast milk (OR = 2.09, 95% CI: 1.39–1.93), multiple births (OR = 1.615, 95% CI: 1.18–2.210), smoking (OR = 2.906, 95% CI: 2.239–3.771), and single motherhood (OR = 1.439, 95% CI: 1.251–1.654).
Conclusion:
This study underscores the need for individualized breastfeeding support strategies in NICUs, taking into account the diverse backgrounds of mothers. Future research should focus on unraveling the underlying mechanisms affecting breastfeeding in preterm infants, with the goal of enhancing breastfeeding rates and improving developmental outcomes.
Introduction
Preterm infants, defined as live births with a gestational age of less than 37 weeks (fewer than 259 days), 1 are increasingly prevalent globally. From 2012 to 2018, the annual increase in preterm birth rates was approximately 1.3%, 2 and in 2020, the number of preterm births reached 13.4 million, accounting for 9.9% of all births. 3 Breastfeeding is crucial for the growth and development of preterm infants, significantly reducing the risk of necrotizing enterocolitis, brain hemorrhage, and sepsis 4 while also decreasing the likelihood of chronic diseases in mothers.5,6 Nevertheless, the global exclusive breastfeeding rate remains suboptimal at 48.6% in 2019, 7 falling short of the World Health Organization’s targets. 8 This issue is particularly acute among preterm infants, with a breastfeeding rate of only 33.3%. 9 Owing to their immature organ functions, especially poor sucking and swallowing abilities, preterm infants often require specialized care in Neonatal Intensive Care Units (NICUs). In NICUs, multiple obstacles hinder breastfeeding, such as physiological immaturity, mother–infant separation, and reduced contact with the mother’s breast. 10 Therefore, the study of barriers to breastfeeding in preterm infants within NICU settings is of critical importance to both clinical practice and public health. Nevertheless, the current body of research faces limitations, including small sample sizes, variations in survey methodologies and measurement timings, impacts of potential confounders, and a predominant focus on the moderate and late preterm infant;11–13 these limitations restrict the universality and applicability of findings. By conducting a systematic review and meta-analysis of the existing literature, this study seeks to elucidate the challenges to breastfeeding encountered by preterm infants in NICUs. It aims to provide an evidence-based platform for devising effective interventions that can enhance breastfeeding rates among preterm infants and improve their growth and developmental trajectories.
Method
Study registration
This systematic review was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 14 The study has been registered with the PROSPERO international prospective register of systematic reviews (Registration Number: CRD42023491499).
Search strategy
To ensure comprehensiveness and accuracy, a systematic literature search strategy was adopted. We conducted extensive searches in five databases: Cochrane Library, PubMed, Web of Science, Embase, and Scopus, covering literature from the inception of each database to September 2023. Medical Subject Headings and free text terms were combined to adapt to different database search mechanisms. The specific search strategies for each database are detailed in the Supplementary Data S1.
Selection criteria
Inclusion criteria:
Study Types: Cross-sectional, cohort, and case–control studies were included. Study Subjects: Subjects were preterm infants admitted to NICU and receiving breastfeeding. Outcome Measures: The aim was to explore factors potentially leading to breastfeeding barriers in NICU preterm infants.
Exclusion Criteria:
Quality assessment
The risk of bias in case–control and cohort studies was assessed using the internationally recognized NOS, which includes eight items across three dimensions: selection (four items), comparability (one item), and outcome or exposure (three items). The NOS uses a semiquantitative star system to assess study quality, with a maximum of 2 stars for comparability and 1 star for other items, totaling a score range of 0–9 stars. Studies were categorized as low (0–5), moderate (6–7), or high quality (8–9). 15 For cross-sectional studies, the AHRQ-recommended criteria were used, comprising 11 items with options of “Yes,” “No,” or “Unclear.” Each “Yes” response scores 1 point, whereas “No” or “Unclear” scores 0. The total scores categorize studies as low (0–3), moderate (4–7), or high quality (8–11). 16
Data extraction
Two nursing postgraduates independently screened literature and extracted data using EndNote, followed by cross-validation to ensure accuracy and consistency. Any discrepancies encountered during screening or data extraction were resolved through team discussion or consultation with a third-party expert. Extracted data included the first author’s name, publication year, country or region of study, study type (e.g., cross-sectional, cohort, case–control), NOS or AHRQ score, sample size, breastfeeding rates in preterm infants, and various factors influencing breastfeeding.
Statistical analysis
Comprehensive meta-analysis of breastfeeding barriers mentioned in selected literature was conducted using Stata 15.0 software. To ensure the validity and accuracy of the analysis, each barrier factor was required to be supported by the odds ratios (OR) and their 95% confidence intervals (CI) from at least three studies. Heterogeneity among studies was assessed using Cochran’s chi-squared test (Cochran’s Q) and I2. When I2 > 50% and p ≤ 0.10, indicating significant heterogeneity, a random-effects model was used. Subgroup analysis and sensitivity analysis were then conducted to identify and explore potential causes of significant heterogeneity. If I2 < 50% and p > 0.10, a fixed-effects model was chosen for analysis. 17 To assess potential publication bias, funnel plots and tests for funnel plot symmetry were used to evaluate bias in published studies subjectively and objectively.
Result
Search results
The preliminary search yielded a total of 3,463 relevant articles, including 327 from PubMed, 320 from Cochrane Library, 2,084 from Web of Science, 251 from Embase, and 481 from Scopus. After removing duplicates, articles with irrelevant titles and abstracts, full texts not meeting inclusion criteria, studies without available OR, studies of low quality, and those without accessible full texts, 32 studies were found to meet the inclusion criteria.18–49 This included 7 case–control studies,24,25,29,31,34,39,40 13 cross-sectional studies,20–22,27,28,33,35–37,41,43,46,49 and 12 cohort studies.18,19,23,26,30,32,38,42,44,45,47,48 For the detailed literature screening process, please refer to Figure 1.

Flow diagram of study screening.
Quality assessment of studies
Upon completing the quality assessment of the included articles, 21 were determined to be of moderate quality20,23–29,31–34,36,38,39,42,45–49 and 11 of high quality.18,19,21,22,30,35,37,40,41,43,44 The 7 case–control studies24,25,29,31,34,39,40 and 12 cohort studies18,19,23,26,30,32,38,42,44,45,47,48 were assessed using the NOS, with all studies scoring 6 or higher; the 13 cross-sectional studies20–22,27,28,33,35–37,41,43,46,49 were assessed using the scoring system recommended by the AHRQ, with all studies also scoring 6 or higher. The specific scoring results are detailed in Table 1.
Basic Characteristics of the Included Studies
① Cesarean section; ② Low gestational age; ③ Prolonged hospital stay; ④ Delayed lactation; ⑤ Low maternal education; ⑥ Insufficient breast milk; ⑦ Multiple births; ⑧ Smoking; ⑨ Single motherhood; ⑩ Ethnicity; ⑪ Obesity.
AHRQ, Agency for Healthcare Research and Quality; NOS, Newcastle–Ottawa Scale.
Meta-analysis of pooled OR and heterogeneity test
Our findings indicated that out of these 11 factors, 6 showed statistical significance in contributing to breastfeeding difficulties. Specifically, low gestational age (OR = 1.36, 95% CI: 1.06–1.75), low maternal education (OR = 1.64, 95% CI: 1.39–1.93), insufficient breast milk (OR = 2.09, 95% CI: 1.40–3.12), multiple births (OR = 1.615, 95% CI: 1.18–2.210), smoking (OR = 2.906, 95% CI: 2.239–3.771), and single motherhood (OR = 1.439, 95% CI: 1.251–1.654) were identified as significant barriers. In contrast, cesarean section, prolonged hospital stay, delayed lactation, ethnicity, and obesity did not exhibit a significant impact on breastfeeding in preterm infants. The heterogeneity analysis suggested that the effects of low maternal education, insufficient breast milk, multiple births, smoking, and single motherhood were relatively consistent (PQ > 0.05 and I2 < 50%), indicating their stronger association with breastfeeding challenges. Further details can be referred to in Table 2.
Meta-Analysis of Breastfeeding Obstacles in NICU-Admitted Preterm Infants
Fixed-effect model.
Random-effect model.
NICU, neonatal intensive care unit.
Subgroup analysis
The prerequisite for conducting subgroup analyses is that the barrier factors under study demonstrate statistical significance (p < 0.05) and exhibit high heterogeneity(I2 < 50%). From the data in Table 2, two factors meet these criteria: low gestational age and multiple births. The following are the results of the subgroup analyses for these two factors.
Low gestational age
In the subgroup analysis focused on low gestational age, the pooled OR from four cohort studies was 0.76, 95% CI: (0.66–0.87), with an I2 of 0%, indicating homogeneity in this specific context. For the case–control studies, the aggregated OR from three studies was 3.40, 95% CI: (1.96–5.88), also with an I2 of 0%, reflecting a consistent trend across these studies. In addition, the combined OR derived from three cross-sectional studies was 1.46, 95% CI: (1.31–1.62), with an I2 of 43.3%, suggesting moderate heterogeneity within this subgroup. These findings illustrate that although there is a marked consistency in the impact of low gestational age on breastfeeding barriers across cohort and case–control studies, the cross-sectional studies exhibit some variability, indicating the potential influence of additional variables. The detailed outcomes of this subgroup analysis are depicted in Figure 2.
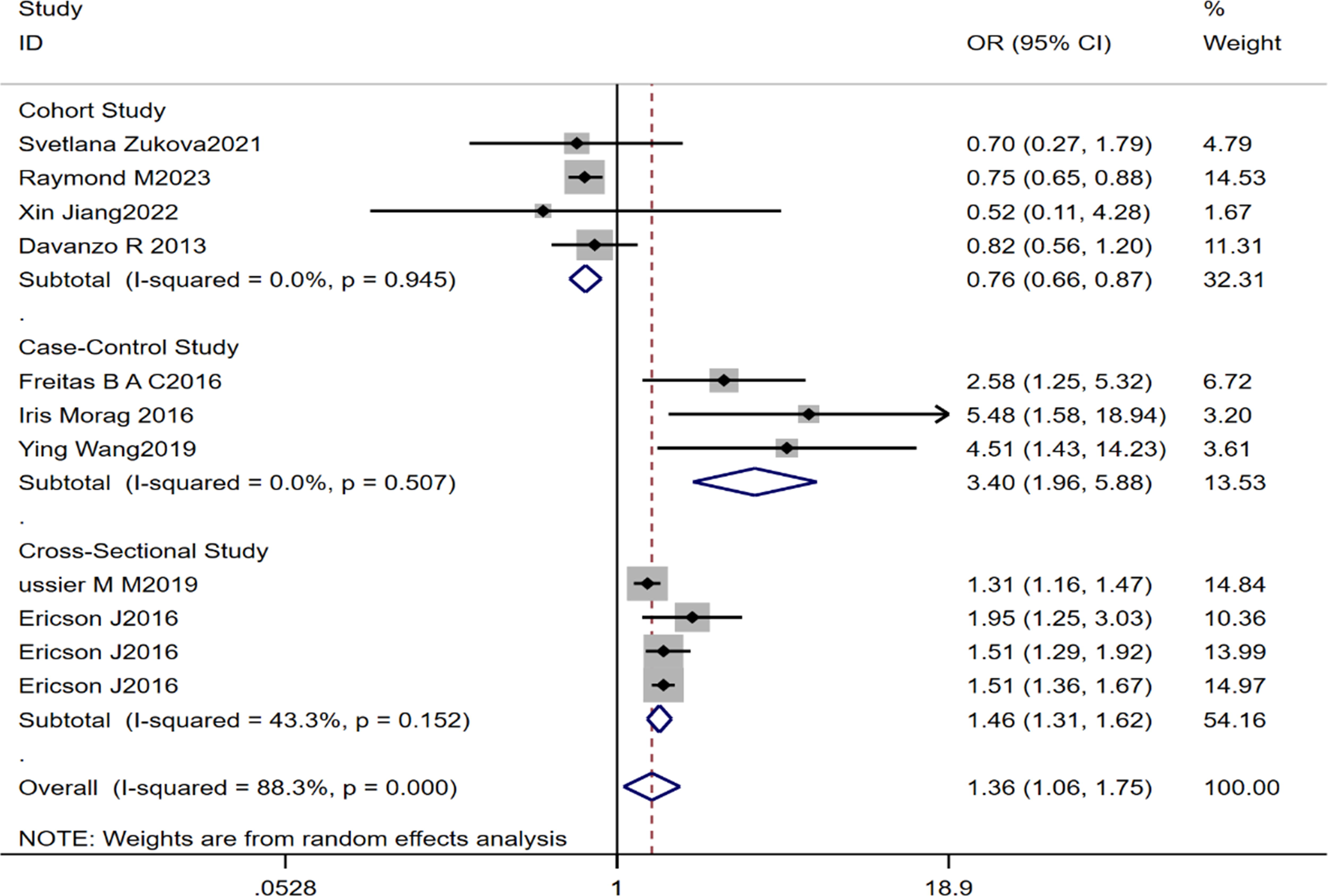
Subgroup analysis chart for low gestational age in the meta-analysis of breastfeeding obstacles in NICU. NICU, neonatal intensive care unit.
Multiple births
In analyzing the impact of multiple births on breastfeeding challenges in preterm infants, we divided the studies into two subgroups: outside of the United States and within the United States. The subgroup analysis of four studies outside the United States indicates that multiple births significantly increase the difficulty of breastfeeding, with a combined OR of 1.12, 95% CI: (1.04–1.21) and highly consistent results. In the United States, the combined OR from three studies in the subgroup analysis is 3.35, 95% CI: (2.14–5.24), also demonstrating consistency. This indicates that multiple births significantly increase breastfeeding difficulties, especially in the United States. Although the overall heterogeneity is high (I2 = 77.2%, p < 0.001), the consistency within the subgroups is notable, suggesting that geographic region may be a key factor contributing to overall high heterogeneity. Therefore, geographic location is an important consideration when evaluating the impact of multiple births on breastfeeding challenges in preterm infants. The results of the subgroup analysis are presented in Figure 3.

Subgroup analysis chart for multiples in the meta-analysis of breastfeeding obstacles in NICU. NICU, neonatal intensive care unit.
Sensitivity analysis
Low gestational age
In the sensitivity analysis for low gestational age, it was observed that the combined effect size estimates remained stable even after excluding any individual study. This indicates a high reliability of the conclusion that low gestational age is a significant barrier to breastfeeding in preterm infants. The combined effect size estimates of all studies fluctuated around a central value of 0.25, within a range of 0.18–0.31, without any extreme or outlier values, reflecting consistency and stability of the overall results. The bubble chart is found in the Supplementary Data S1.
Multiple births
The sensitivity analysis concerning multiple births demonstrated a high level of stability. Excluding any individual study did not significantly affect the OR and 95% CI for multiple births as an impediment to breastfeeding in preterm infants. The estimates predominantly centered around a combined OR of 0.14, with a 95% CI ranging from 0.07 to 0.21. This close grouping indicates strong consistency across the included studies, affirming reliability and validity of the meta-analysis. The bubble chart is found in the Supplementary Data S1.
Publication bias analysis
Given that the effective creation of funnel plots typically requires more than 10 articles, we categorized the barriers into two main groups based on maternal and infant factors for our analysis: infant factors and maternal factors. In this study, the infant factors primarily include low gestational age and multiple births, whereas the maternal factors involve aspects such as education level, insufficient breast milk, smoking habits, and marital status. We used these data to create funnel plots and conducted symmetry tests to assess potential research biases. The related funnel plots and their symmetry test results are available in the Supplementary Data S1.
Maternal factors
The funnel plot analysis indicated that the majority of studies’ effect size estimates were closely distributed around the central axis, showing no evident systematic bias. Both Begg’s and Egger’s tests did not detect any significant publication bias (Begg’s Test p = 0.617; Egger’s Test p = 0.459). Despite a slight asymmetry in the funnel plot, the results are considered acceptable, reinforcing the credibility of the study outcomes.
Infant factors
In the analysis of infant factors, although the funnel plot showed some degree of asymmetry, most studies were still concentrated near the central line, suggesting a smaller publication bias. Neither Begg’s test nor Egger’s test found significant publication bias (Begg’s Test p = 0.570; Egger’s Test p = 0.148). Overall, the meta-analysis results suggest that the effect size estimates for multiple births as barriers to breastfeeding in preterm infants are robust.
Discussion
This meta-analysis represents the first comprehensive assessment of the factors impeding breastfeeding in preterm infants within the NICU environment. A systematic review of the relevant literature enabled the quantification of key determinants affecting breastfeeding in preterm infants. Our findings identified six primary obstacles: low gestational age, low maternal education, insufficient breast milk, multiple pregnancies, smoking, and single motherhood.
Notably, smoking and insufficient breast milk demonstrated moderate to strong effects (OR ≥ 2), whereas the other four factors exhibited lesser impact (OR < 2). Particularly, smoking emerged as the most significant barrier to breastfeeding in preterm infants. Despite a limited number of studies addressing the relationship between smoking and breastfeeding barriers (n = 4), a consistent effect was observed across these studies, evidenced by a remarkably low heterogeneity (0%). Smoking was found to significantly reduce milk production and lactation duration 50 while also decreasing the fat, calorie, and protein content in the milk, 51 adversely affecting breastfeeding in preterm infants. These findings align with the research conducted by Ariz et al. 52 who reported shorter breastfeeding durations among mothers who smoked during pregnancy compared to nonsmoking mothers. Conversely, our findings slightly diverge from those of Hamilton et al. 53 who noted a higher proportion of breastfeeding among women using electronic cigarettes compared to traditional smokers. This discrepancy could be attributed to several factors. First, Hamilton et al. 53 might have focused on comparing the differing impacts of electronic and traditional cigarettes on breastfeeding, whereas our meta-analysis concentrated more broadly on the impact of smoking per se. In addition, Hamilton et al. 53 may have considered the compositional and habitual differences between electronic and traditional cigarettes, which could explain the variance in their respective impacts on breastfeeding. Moreover, lifestyle and health consciousness differences among electronic cigarette users might also influence their breastfeeding behaviors. Despite these differences, our study and that of Hamilton et al. 53 reflect the diversity and complexity in research within this field.
Furthermore, our analysis indicates a positive correlation between insufficient milk supply and breastfeeding barriers in preterm infants. Insufficient milk supply can be due to various factors, including psychological, social, or biological characteristics of the mother, leading to anxiety and frustration, which further affect the duration and effectiveness of breastfeeding. This is consistent with Riaz et al. 54 who noted that insufficient milk supply hinders breastfeeding among rural mothers in Pakistan. Interestingly, our study diverges in some aspects as we have quantitatively synthesized the impact of insufficient milk supply on breastfeeding in preterm infants, providing a macroscopic perspective. The in-depth analysis of Riaz et al. underscores the importance of understanding cultural background and personal experiences in revealing the microdynamics behind the issue of insufficient milk supply.
Our study particularly focuses on the impact of limited maternal education and single parenthood on breastfeeding in preterm infants. Moreover, the limitation in maternal education level has a significant impact on breastfeeding practices. Research indicates that mothers with lower education levels may lack sufficient understanding of the benefits of breastfeeding and strategies to resolve issues encountered during the process. Educational level is closely related to the way mothers access health information, their understanding, and their choice of health behaviors. Therefore, enhancing education levels is considered a key strategy to improve breastfeeding rates. Interestingly, some studies suggest that in low- and middle-income countries, lower maternal education levels correlate with higher breastfeeding rates, possibly because of breastfeeding being more common in these countries, influenced by social and cultural factors rather than individual choice or knowledge level. In addition, single parenthood increases the mother’s challenges in terms of economic and social support. Single mothers, with limited economic resources, often shoulder more parenting responsibilities while lacking direct support from partners or family members. These factors may lead to greater stress and fatigue for the mother, affecting her ability to breastfeed and the sustainability of breastfeeding.
Compared to Carolina et al., 55 our meta-analysis further deepens the understanding of factors affecting breastfeeding in preterm infants. Although our results concur with their findings regarding low gestational age, multiple pregnancies, smoking, and maternal education level, our study advances in exploring the impact of insufficient milk supply and single parenthood on breastfeeding. These new findings expand our understanding of breastfeeding barriers, revealing areas not previously covered by Carolina et al. 55 Moreover, our data did not support the findings of Carolina et al. on the impact of newborn weight on breastfeeding duration. These results indicate that the factors influencing breastfeeding are continuously evolving and need to be reassessed more broadly. It is noteworthy that our study differs from Carolina et al. 55 in terms of research subjects and interpretation of results. Carolina et al. focused on newborns and their mothers, finding that low gestational age reduces breastfeeding to 70%, whereas singleton pregnancy extends breastfeeding duration. In contrast, our study focuses on a specific group of preterm infants, revealing how research type and geographic location affect the relationship between low gestational age, multiple pregnancies, and breastfeeding in preterm infants. Although the methodologies and focus of the two studies differ, both highlight the significant impact of low gestational age.
Conclusions
This meta-analysis provides new insights into the systematic assessment of barriers to breastfeeding in preterm infants within the NICU environment. Our study emphasizes the importance of implementing comprehensive strategies tailored to the individual backgrounds of mothers, particularly those facing specific challenges such as insufficient milk supply and smoking. Future research is needed to delve deeper into the mechanisms affecting breastfeeding in preterm infants, including the interplay of social, psychological, and biological factors. A better understanding of these mechanisms will enable the design and implementation of more targeted interventions to enhance breastfeeding rates in preterm infants and improve their long-term health and developmental outcomes. Overall, this research not only advances our understanding of the barriers to breastfeeding in preterm infants but also offers valuable guidance for clinical practice, outlining directions for future research. These findings are crucial for optimizing nutritional management in the NICU environment and improving the overall health and development of preterm infants.
Limitations
Although our study has made progress in assessing the barriers to breastfeeding in preterm infants within the NICU environment, it also presents some limitations. First, the limited number of studies addressing each barrier may restrict our comprehensive understanding of these factors’ impacts. Second, some barriers, such as cesarean delivery, low gestational age, prolonged hospital stay, and multiple births, exhibit considerable heterogeneity in the included literature. This heterogeneity could affect the stability of our analysis results and conclusions. Finally, the overall quality of the included literature is moderate to low, potentially impacting the accuracy and reliability of our findings. In response to these limitations, future research should expand literature sources, including a wider variety of study types and languages, to increase the number of included studies and enhance their quality. In addition, given the prevalence of heterogeneity in meta-analyses, we suggest adopting more comprehensive methods in future research to explore the sources of heterogeneity. Although we have conducted subgroup and sensitivity analyses, other strategies such as meta-regression analysis, Bayesian analysis, or influence analysis should also be used to better understand the potential causes of variations in results across different studies. These diversified methods will enable more effective identification and interpretation of variables that may influence research outcomes, thereby increasing the accuracy and reliability of meta-analyses. Such comprehensive analysis will aid in gaining a more holistic understanding of the complexities surrounding breastfeeding barriers in preterm infants and provide a more robust evidence base for future clinical practice and research.
Footnotes
Acknowledgments
We have not received funds in support of research work or for covering the costs to public in open access.
Authors’ Contributions
C.L. was the lead author and primary investigator of the study. She was responsible for the study conception, design, data acquisition, and drafting the initial article. Her contributions also included the integration of data for the meta-analysis and interpreting the findings in the context of NICU environments. M.P. played a key role in the systematic review process, including the literature search, screening for eligibility, and extraction of data. She also contributed to the drafting and critical revision of the article for important intellectual content. X.L. was involved in the data analysis, particularly in the statistical modeling and sensitivity analyses. She assisted in interpreting the results and provided substantial input in the article preparation and revision stages. Y.G. contributed to the interpretation of the data, particularly focusing on the clinical implications of the findings for preterm infants in NICU settings. She also contributed to the critical revision of the article and ensured the accuracy of the data presented. J.X. and X.C., as co-corresponding authors, oversaw the entire project. They provided guidance on the study design, analysis, and interpretation of the data. They were also responsible for the final approval of the article to be submitted. Both ensured that all aspects of the work were properly investigated and resolved, and they are the points of contact for further inquiries regarding the research. All authors have read and approved the final version of the article.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This research received no external funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.