
Abstract
Objective:
The study aimed to assess the transfer of merotocin from systemic circulation to breast milk in early postpartum women and women with established lactation.
Methods:
This was a two-part, multicenter, open-label, parallel-group study. Merotocin was administered as a single 90-minute intravenous (iv) infusion mimicking the intranasal pharmacokinetic profile. In Part A, 12 early postpartum women received doses of either 4 μg (n = 6) or 16 μg (n = 6) of merotocin within 4 days of delivery. In Part B, six women with established lactation received 20 μg of merotocin. The total concentration of merotocin in plasma and breast milk and its metabolites excreted in breast milk were measured at various time points. Adverse events (AEs) were also assessed for both parts of the study.
Results:
In both early postpartum and established lactation groups (mean age, 26.3 years; 83.3% Caucasian), merotocin and its metabolites in breast milk were below the limit of quantification (25.0 pg/mL) at all time points. Sixteen treatment-emergent AEs occurred in early postpartum women only, including seven events of uterine spasm and three of breast engorgement. There was one moderate event, whereas all the other events were considered mild.
Conclusion:
Merotocin was undetectable in breast milk after single iv administration of up to 20 μg in early postpartum women and women with established lactation.
Introduction
The World Health Organization recommends exclusive breastfeeding for the first 6 months of life to reduce newborn mortality, improve child development, and reduce health care costs.1,2 Breast milk can play a key role in the health of both term and preterm infants, with benefits immediately after birth and in the longer term. 3 Breastfeeding is especially recommended in preterm infants who are often born with a higher risk of infections and developmental disabilities compared with term infants.4,5 In 2021, there were approximately 3.7 million births in the United States, of which an estimated 10.5% babies were born preterm (before 37 completed weeks of gestation). 6 Breastfeeding has been shown also to contribute to the health and well-being of mothers, being associated with a reduced risk of ovarian and breast cancer. 2
Many women experience breastfeeding difficulties, despite measures to support and increase breastfeeding rates. Generally, secretory activation or lactogenesis II is achieved by mothers within 48–72 hours of childbirth, which helps to establish a lasting milk supply. 7 However, some women may not achieve secretory activation at all, whereas others may experience low milk supply even after secretory activation. Some of the factors that can cause low milk supply are less-than-optimal breast stimulation during the critical first 2 weeks post birth,8,9 incomplete maturation of the mammary glands,8,10 preterm delivery with associated multiple risk factors,11,12 and maternal stress owing to separation from the infant during a neonatal intensive care unit stay. 9
Nonpharmacological measures such as increased emotional support, skin-to-skin contact and massage, relaxation techniques, expressing breast milk at the infant’s bedside, increasing pumping times, and alterations in mechanical expression of breast milk provide variable levels of success in augmenting breast milk production. 13 Currently, there are few pharmacological therapies globally approved for breast milk augmentation, with metoclopramide and domperidone available in many countries, but none are approved for use in lactation support in the United States. 14
The endocrinology of lactation is highly complex, with oxytocin known to play an important role both in lactation and to reverse stress-induced inhibition of milk production. 15 In a small pilot study, intranasal administration of 6 international units (IU; 10 μg) of oxytocin was demonstrated to enhance milk production in the immediate postpartum period in women who had given birth prematurely. 16 However, a subsequent study by Fewtrell et al. 17 showed that when oxytocin was administered at the recommended dose of 8 IU (13 μg), outcomes, which included total weight of milk expressed and pattern of milk production, were more variable, with suboptimal efficacy. These conflicting results may be the consequence of differences in study design and/or dosing between these two trials. More importantly, the pharmacological application of oxytocin may be constrained by dose-limiting adverse events (AEs) seen owing to vasopressin-receptor agonism, such as antidiuresis and possibly hyponatremia, which may lead to headache, nausea, and vomiting.18,19
This has prompted the investigation of potent, selective, and safe oxytocin agonists that can be used as galactagogues, either to increase milk production or milk release from the breast, as a means of improving breast milk supply. 20 The dopamine-receptor antagonists, such as domperidone and metoclopramide, are the most widely used galactagogues, despite not being approved for this purpose in many countries, with a paucity of data demonstrating any significant efficacy or safety with either agent. 14 In one study, women who had received domperidone showed increased milk volume by ≥50%; however, the increase in absolute milk volume from baseline remained modest and was not significantly greater on Day 14 or Day 28 than in women who had received placebo. 21 In another study, administration of metoclopramide demonstrated that there was no improvement in milk volume or duration of breastfeeding in women with preterm delivery compared with administration of placebo. 22 Side effects of these centrally acting agents can be serious, including tremor, bradykinesia and other dystonic reactions, and cardiac arrhythmias.23–25 In fact, safety concerns led the U.S. Food and Drug Administration (FDA) to issue a public warning in 2004 stating that distributing any domperidone-containing products is illegal, and the European Medicines Agency issued restrictions on the use of domperidone in 2014.26,27 Hence, there remains an unmet medical need for safe and effective measures to support breastfeeding, especially in women who have given birth to preterm infants.
Merotocin is an investigational potent, short-acting, selective oxytocin-receptor agonist specifically designed with minimal risk of hyponatremia for the induction and support of lactation during breastfeeding in postpartum women. 28 In a first-in-human study, intranasal merotocin spray was shown to be well tolerated at doses of up to 400 μg every 3 hours and as an intravenous (iv) infusion of 20 μg over 25 minutes. 29
Here, we present the findings from a Phase 1, two-part study in early postpartum women and women with established lactation, which investigated possible transfer of merotocin from systemic circulation to breast milk (EudraCT:2012-001354-26).
Materials and Methods
Study design and participants
This was a two-part, multicenter, open-label, parallel-group study. In Part A of the study, 12 early postpartum women received a single 90-minute iv infusion of 4 μg or 16 μg of merotocin, and in Part B of the study, six women with established lactation received a single 90-minute iv infusion of 20 μg of merotocin.
Infants received formula milk for the first 24 hours post dose (after the completion of the infusion). Breast milk samples taken 24 hours post dose from the first two women included in Part A of the study were analyzed and if the merotocin concentrations in these milk samples were below the lower limit of quantification (LLOQ) of 25.0 pg/mL, they and subsequent participants were allowed to breastfeed after 24 hours from dosing. The study was conducted in accordance with the Declaration of Helsinki and its amendments in force at the initiation of the study, in compliance with the approved protocol and its amendment, Good Clinical Practice, and applicable regulatory requirements. An independent Institutional Review Board and an independent Research Ethics Committee both reviewed and approved the study protocol. All study participants gave informed consent before any study-related procedures.
Part A: Early postpartum women
Eligible participants were healthy (well-controlled, noninsulin-dependent diabetes allowed) women of age 18–40 years with a prepregnancy body mass index (BMI) equal to or above 18 kg/m2 and below 34 kg/m2, who had had a normal pregnancy and had just delivered a single, healthy child without any sign of pregnancy-induced hypertension or pre-eclampsia, and a gestation of 37–42 weeks. Participants were required to withdraw from Part A of the study if they experienced any complications during or after parturition, such as those resulting in major blood loss (>500 mL). A single iv infusion of 5 μg or 20 μg of merotocin was administered over 90 minutes to parallel dose groups containing six participants each, all of whom were within 4 days of delivery. Analysis of the merotocin content in the tubing outflow in Part A revealed a dose loss of approximately 20%, and participants within the two treatment arms therefore received actual doses of approximately 4 μg and 16 μg, respectively. In Part B of the study, this loss was compensated for by an increase in the infusion solution concentration to negate the effects of drug adsorption by glass vessels during the dilution process and by priming the infusion tubing. Hence, the participants in Part B received the intended dose of 20 μg.
Merotocin was administered by iv infusion to decrease the high variability in bioavailability seen with the intranasal route of administration. The iv infusion was administered to mimic the pharmacokinetic (PK) profile of intranasal administration, i.e., a maximal plasma concentration approximately 15 minutes after start of infusion with a half-life of approximately 30 minutes. Milk samples were collected by emptying both breasts completely and taking an aliquot of the mixed total sample. The predose sample was taken 2 hours before dosing. Milk samples were subsequently collected from both breasts using a breast pump at 15 minutes and 3, 6, 9, 12, 18, and 24 hours after the start of infusion for analysis of merotocin and its metabolites. In addition, milk was collected ad libitum between the time points 18 and 24 hours after start of infusion with the milk saved in the separate fractions collected.
Blood samples for measurement of plasma concentration of merotocin were collected predose, at 15 minutes, and 0.5, 1, 2, and 4 hours after start of merotocin administration. Blood samples for clinical chemistry (albumin, alkaline phosphatase, alanine aminotransferase, aspartate aminotransferase, bilirubin, calcium, chloride, creatinine, C-reactive protein, gamma glutamyl transferase, glucose, potassium, phosphate, prolactin, sodium, and triglycerides), hematology (hematocrit, basophils, eosinophils, hemoglobin, lymphocytes, erythrocytes, monocytes, neutrophils, platelets, leukocytes, and reticulocytes), and hemostasis were taken predose and at 0.5 and 4 hours after start of infusion, and samples for urinalysis were taken predose, and at 1.5 and 4 hours after start of infusion.
Part B. Women with established lactation
Part B of the study included six women of age 18–40 years with a normal pregnancy (gestation 37–42 weeks) without any sign of pregnancy-induced hypertension or pre-eclampsia, who had established lactation following delivery of a single healthy child. Participants had a prepregnancy BMI equal to or above 18 kg/m2 and below 34 kg/m2; well-controlled, noninsulin-dependent diabetes was permitted. Study participants received a single iv infusion of 20 μg merotocin administered over 90 minutes. As in Part A, the infusion mimicked the time course of the PK profile of intranasal administration. Breast milk and blood samples were collected using the same method and schedule as in Part A of the study.
Study endpoints
The primary endpoint of the study was the assessment of the total amount of merotocin excreted in breast milk following a single iv dose in relation to the administered dose. Secondary study endpoints included type, frequency, and intensity of AEs and presence of metabolites of merotocin in breast milk.
Study assessments
Analyses of the total concentration of merotocin and any metabolites excreted in plasma and breast milk samples were performed by the Department of Bioanalysis at Ferring Pharmaceuticals A/S. The breast milk and plasma samples were analyzed using a method based on Waters ACQUITY I-Class ultra-performance liquid chromatography (UPLC) coupled to a XEVO TQ-S MS/MS tandem mass spectrometry system. The LLOQs were 25.0 pg/mL and 20.0 pg/mL merotocin, for breast milk samples and plasma samples, respectively, as determined from quality control samples. The method performance for the milk analysis gave a mean bias within ±5% and coefficient of variation (CV) within 11% for all concentration levels. The method performance for the plasma analysis gave a mean bias within ±6% and CV within 10% for all concentration levels.
AEs were assessed throughout the study from screening to follow-up in both Part A and Part B of the study. Collection of AEs comprised the participants’ responses to questions about their health, symptoms spontaneously reported by the participants, and clinically relevant changes and abnormalities observed by the investigator. Serious AEs were reported to Ferring Global Pharmacovigilance within 24 hours of the event.
Statistical analyses
Descriptive statistics were used to assess demographics and baseline characteristics of the full analysis set (FAS), which comprised data from all study participants who received merotocin and had at least one post-baseline study assessment. Milk and plasma concentrations of merotocin are presented by treatment group and time. AEs were coded according to the latest version of the Medical Dictionary for Regulatory Activities (MedDRA) available at the time.
Results
Study participants
A total of 18 women were included in the study; 12 in part A and 6 in part B (mean age = 26.3 years, 83.3% Caucasian) (Table 1). Participants in Part A had a mean age of 25.5 years in the 4 μg group and 24.7 years in the 16 μg group; all were Caucasian, and 50% were also Hispanic or Latino. In Part B, participants were slightly older (mean age = 28.8 years); 50% were Caucasian, 33% Black or African American, and 17% Asian.
Participant Demographic and Baseline Characteristics
SD, standard deviation; BMI, body mass index.
Quantification of merotocin in breast milk
In all women, at all timepoints, and in both parts of the study, the concentration of merotocin in breast milk was below 25.0 pg/mL, the LLOQ. All values below the LLOQ were arbitrarily assigned a value half of that level (i.e., 12.5 pg/mL) for plotting purposes. No metabolites of merotocin were detected in any of the breast milk samples collected in both parts of the study.
Quantification of merotocin in plasma
The highest mean (standard deviation [SD]) plasma concentrations of merotocin were measured 15 minutes after administration in all dose groups (Table 2, Fig. 1). By 4 hours post dose, merotocin plasma concentrations were below LLOQ in all study participants.
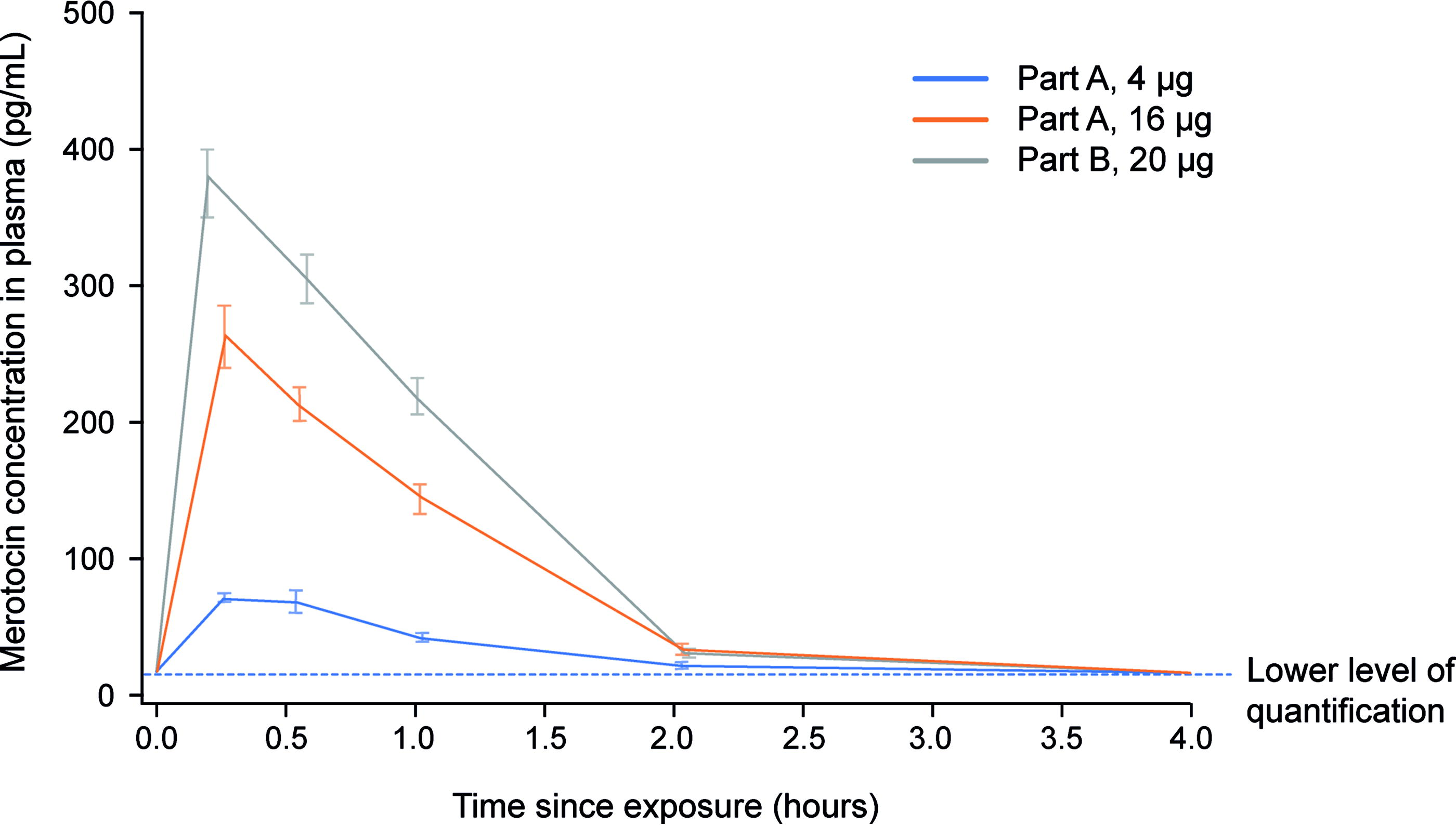
Profile plot of mean merotocin concentration in plasma over time. Error bars indicate standard error. The lower limit of quantification (LLOQ) = 20.0 pg/mL.
Summary of Mean Plasma Merotocin Concentrations Over Time (Full Analysis Set)
N, number of subjects in the full analysis set; n, number of subjects with data.
SD, standard deviation; LLOQ, lower limit of quantification (20.0 pg/mL).
Clinical laboratory findings
Evaluation of Part A and Part B clinical laboratory data revealed no apparent trends or changes related to dose in the hematology, clinical chemistry, and hemostasis parameters. For some clinical chemistry parameters, sporadic changes from normal/high values to values below normal range and from normal/low values to values above normal range were observed in both Part A and Part B in all dose groups. The values were not regarded as clinically significant, and most changes were observed only once, with the exception of normal/low to high changes in glucose (six events), triglycerides (three events), and aspartate aminotransferase and phosphate (both, two events), and normal/high to low changes in creatinine and glucose (both, two events).
Safety
No treatment-emergent adverse events (TEAEs) were reported by any participants in Part B and most TEAEs reported in Part A were mild (Table 3).
Overall Summary of Treatment-Emergent Adverse Events
TEAE, treatment-emergent adverse event; N, number of participants exposed; n, number of participants with an AE; E, number of AEs; AE, adverse event.
During the 6-week postnatal period.
Possibly related to treatment. Note that only two categories were used: reasonable possibility (evidence to support a causal relationship between merotocin and the AE) and no reasonable possibility (no reasonable evidence to suggest a causal relationship between merotocin and the AE). All assessments of causality were at the investigator’s discretion.
In Part A of the study, nine TEAEs occurred in three participants in the 4 μg dose group and seven TEAEs occurred in five participants in the 16 μg dose group (Table 3). The most frequently reported TEAEs were seven events of uterine spasm reported by six participants (four events reported by three participants in the 4 μg dose group and three events reported by three participants in the 16 μg dose group), three events of breast engorgement reported by three participants (all in the 16 μg dose group), and three events of headache reported by two participants (both in the 4 μg dose group). All TEAEs were of mild intensity except one event of uterine spasm of moderate intensity in a participant in the 4 μg dose group.
Two participants in Part A reported four AEs observed 1-day post treatment. One participant in the 4 μg dose group reported one event of oropharyngeal pain and one event of incision-site pain, and one participant in the 16 μg dose group reported one event of abdominal pain and one event of breast discomfort. All events were of mild intensity, and all events, except the event of oropharyngeal pain, were assessed as possibly related to treatment.
All TEAEs, except for one event of muscle spasm reported by one participant in the 4 μg dose group, were considered as adverse drug reactions and possibly related to treatment. No severe or serious AEs occurred, and there were no fatal AEs or AEs resulting in study discontinuation in any part of the study (Table 3).
Discussion
This study demonstrated that the administration of a single iv dose of merotocin in early postpartum women and women with established lactation did not result in any measurable transfer of merotocin from plasma to breast milk. The iv infusion was selected as the route of administration to better control the high variability and low bioavailability observed during the intranasal route of administration. 30 The amount of merotocin in breast milk was below the LLOQ of 25.0 pg/mL at all timepoints measured in all participants of the study. Moreover, no metabolites of merotocin were detected in any of the breast milk samples. The absence of detectable merotocin in the milk was not because of lack of plasma exposure. Plasma concentrations of merotocin up to 367 pg/mL were observed across doses of both study parts (Table 2), exceeding the LLOQ of 25 pg/mL for milk.
Merotocin was designed to have a high systemic clearance, which is expected to result in a short half-life suitable for multiple daily administrations. 28 Moreover, merotocin is readily degraded by chymotrypsin, 29 a proteolytic enzyme present at similar levels in both the term and preterm infant (being 10%–60% of levels in the adult intestine 31 ), which is thought to reduce the oral bioavailability of merotocin. Thus, if merotocin were to pass to the infant via breast milk, it would be degraded during digestion. However, concentrations in milk below 25 pg/mL are well below the plasma Cmax in neonatal rats at the no observed adverse effect level (2,200 pg/mL 29 ). Merotocin is presumed, therefore, also to be safe in infants since any exposure-related AEs would be unlikely to occur at a concentration below the LLOQ of 25 pg/mL. Overall, there were no safety concerns for the mothers or infants in the study population.
Oxytocin is an essential lactation hormone released during breastfeeding. 32 However, oxytocin is not receptor-selective and interacts with the oxytocin receptor (OTR) and vasopressin 1a, 1b, 2 (V1a, V1b, V2) receptors as an agonist. 33 Merotocin was designed to exhibit high affinity (EC50 value of 0.08 nM compared with 2.3 nM for oxytocin) with marked selectivity to the human OTR versus the human V1a, V1b, and V2 receptors. 28 There are varying reports on the effect of oxytocin doses administered in practice.16,17 Even the maximal reported intranasal doses of 24–40 IU (40–67 μg) resulted in a Cmax of approximately 10 pg/mL. 34 This is likely an ineffective dose considering that endogenous oxytocin levels during breastfeeding can reach peaks up to approximately 120–250 pg/mL, 35 and known side effects of oxytocin will likely limit higher doses. By contrast, peak merotocin concentrations in this study reached 367 pg/mL in the 20 μg iv dose group (equivalent to 400 μg intranasal dose) with no significant safety concerns.
In both dose groups in Part A, the most frequently reported AE by early postpartum women was uterine spasms/cramping, which were predominantly mild, except for one moderate event after administration of approximately 4 μg. This could possibly be because of the interaction of merotocin with the oxytocin receptor and the known increased oxytocin sensitivity women experience in the immediate postpartum period.19,36 There were no AEs reported in Part B.
Although these data demonstrate the safety and PK of merotocin in the study participants, there are some limitations of this study. Only mothers with healthy pregnancies and term births were included to minimize potential confounding factors owing to premature birth. 37 In addition, the study did not assess the efficaciousness of merotocin for improving lactation (e.g., milk volume over time), which will require further investigation.
Strengths of the study are the inclusion of women in the early postpartum period as well as women with established lactation, and that serial sampling of milk and plasma was performed combined with use of a sensitive assay to detect low levels of transfer of merotocin, if present, from plasma to breast milk. The absence of measurable levels of merotocin in breast milk in women in the early postpartum period is significant because at this time, before lactogenesis II and closure of the paracellular pathways in the mammary epithelium, the likelihood of transfer is at its highest. 11
Conclusions
The findings from this study indicate that merotocin and its metabolites do not cross from systemic circulation to breast milk in measurable amounts after single iv administration of up to 16 μg in early postpartum women and 20 μg in women with established lactation. Therefore, the likelihood of clinically relevant transfer of merotocin through breast milk to infants is low. Merotocin was well tolerated and does not induce vasopressin-associated AEs, with few TEAEs occurring in early postpartum women and none in women with established lactation. This study supports the potential utility of merotocin in supporting lactation.
Footnotes
Acknowledgments
Editorial support for the preparation of this article (in the form of writing assistance, collating author comments, assembling tables/figures, grammatical editing and referencing) was provided by Sarah Birch, PhD at Makara Health Communications Ltd., a Precision Value & Health Team, and was funded by Ferring Pharmaceuticals. Statistical support was provided by Okan Elci, PhD who was an employee of Ferring Pharmaceuticals at the time the article was developed.
Authors’ Contributions
T.B.: Conceptualization, Investigation, Resources, Data Curation, Writing—Review and Editing, Supervision, Project Administration; U.L.: Conceptualization, Investigation, Resources, Data Curation, Writing—Review and Editing, Supervision, Project Administration; Y.B.: Conceptualization, Resources, Data Curation, Writing—Review and Editing, Supervision, Project Administration; C.H.: Conceptualization, Methodology, Validation, Resources, Data Curation, Writing—Review and Editing, Project Administration; D.M.J.: Conceptualization, Methodology, Writing—Review and Editing; L.E.U.: Resources, Data Curation, Writing—Review and Editing; T.W.H.: Conceptualization, Investigation, Resources, Data Curation, Writing—Review and Editing, Supervision, Project Administration.
Disclosure Statement
Y.B., C.H., D.M.J., and L.E.U. are employees of Ferring Pharmaceuticals. U.L. was the principal investigator for this trial. She is an employee of Richmond Pharmacology Ltd, London UK. Richmond Pharmacology Ltd. was contracted by Ferring Pharmaceuticals A/S to conduct the clinical trial. T.B. and T.W.H. have no conflicts of interest to disclose.
Funding Information
The study was funded by Ferring Pharmaceuticals A/S, Copenhagen, Denmark.