
Abstract
Background:
Ankyloglossia (AG) diagnoses are increasingly common, and management is not standardized. Nonsurgical alternative therapies are frequently recommended in conjunction with or instead of frenotomy, with uncertain evidence.
Objective:
To evaluate the efficacy of nonsurgical alternative therapies (chiropractic care, myofunctional therapy, and osteopathy) in improving breastfeeding for infants diagnosed with AG.
Methods:
PubMed, Embase, CINAHL, Scopus, Web of Science, Clinicaltrials.gov, and Google Scholar were searched (September–October 2023). Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed. A librarian-designed search included the terms “Ankyloglossia,” “Non-surgical,” “myofunctional therapy,” “chiropractic,” “osteopathy,” and related therapies, with no date restrictions. English language studies of infants <24 months with AG and alternative therapy were included. Risk-of-bias evaluation used Newcastle–Ottawa Scale (NOS).
Results:
Of 1,304 identified articles, four studies (2016–2022) met inclusion criteria (two cross-sectional, one case report, and one case series). All studies reported frenotomy in combination with alternative therapy yielded favorable outcomes for maternal pain, weight gain, feeding duration, and maintenance of latch. The risk of bias was moderate for two studies, low for the case series, and not calculated for the case report, which has an inherent high risk of bias. All studies lacked control or comparator groups preventing definitive conclusions about the role of alternative therapies in AG.
Conclusion:
Although some studies suggest the potential benefits of combining alternative therapies with surgery for AG-related breastfeeding issues, the lack of control groups renders the evidence inconclusive. Nonsurgical approaches alone currently lack sufficient evidence. As these alternative therapies gain popularity, rigorous research is crucial to determine their cost-effectiveness and role in managing AG.
Introduction
Ankyloglossia is a condition of restricted tongue mobility caused by a short, tight, or thick lingual frenulum that may insert close to the distal tongue tip. Between 4% and 11% of newborns have AG. 1 In some cases, AG can contribute to maternal nipple pain and inadequate breastfeeding latch, which may contribute to premature breastfeeding cessation. 2 Breastfeeding is the ideal form of infant nutrition, offering benefits to both members of the breastfeeding dyad, including reduced respiratory infections, improved cognition, decreased risk of obesity in the infant, and decreased rates of breast and ovarian cancer in the lactating parent. 3 Less than half of infants under 6 months old are exclusively breastfed, despite WHO recommendations and the well-established advantages of breastfeeding. 3
Breastfeeding difficulty can be multifactorial. Managing AG, if present, is an important component of the comprehensive care of breastfeeding dyads. Examination of the frenulum must be complimented by observing latch and feeding. 4 Oral examination may reveal restriction of tongue motion in all planes, and/or a heart-shaped tongue tip. 5 There are multiple described diagnostic classification schemes, without a consensus on the gold standard diagnostic technique. 6
Lactation consultation is the cornerstone of optimizing breastfeeding. Interventions may include positional adjustments, infant gape improvements, breast tissue manipulations or use of adjuncts like nipple shields. Frenotomy is a low-risk treatment that may be helpful with proper patient selection. 7 Physical therapy, speech therapy, and alternative medicine procedures, such as orofacial myofunctional therapy, osteopathy, and chiropractic care, are among the other treatments that may be suggested but have uncertain evidence. Though these nonsurgical techniques are potentially low risk, they may be expensive or delay definitive management.
This systematic review aims to comprehensively assess nonsurgical therapies for breastfeeding in infants with AG, whether used alone or as adjuncts to surgical treatment.
Materials and Methods
This systematic review adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines 8 and was prospectively registered in the PROSPERO database (CRD42023471827).
Search strategy
The search strategy was developed with a medical librarian. PubMed, Embase, CINAHL, Scopus, Web of Science, Clinicaltrials.gov, and Google Scholar were searched between September and October 2023. “Ankyloglossia” or “tongue-tie” was searched in conjunction with surgical treatment (frenotomy/frenectomy) and alternative therapies (myofunctional, chiropractic, and osteopathic therapy). Detailed search strategy can be found in Supplementary Data 1. No date filter was applied, and non-English studies were excluded.
Selection criteria
Inclusion and exclusion criteria were determined using the PICOS model (population, intervention, comparison, outcomes, and study design). Inclusion criteria included diagnosis of AG, age <24 months, nonsurgical alternative therapies other than lactation consultation alone, and assessment of breastfeeding outcomes. Study designs included randomized controlled trials (RCTs), nonrandomized controlled trials, cohort studies, case reports, and case series. Papers were excluded if they did not adhere to inclusion criteria, were not in English, or not peer-reviewed.
Study selection process and data extraction
Two researchers (R.C. and J.L.) independently assessed abstracts and full texts for study inclusion. A third investigator (R.A.) resolved discrepancies. Extraction included author information, publication date, study type, sample size, gender, interventions, outcome measures, measurement tools, and main results.
Assessment of risk of bias
Two investigators (R.C. and S.K.) independently assessed risk of bias using the Newcastle–Ottawa Scale (NOS). 9 Based on the majority opinion, studies were categorized as “good”(scores ≥7), “fair” (scores 2–6), or “poor” (scores ≤1) quality.
Results
Search results
A total of 1,304 articles were identified. After removal of duplicates, 766 were screened and 4 met inclusion criteria.10–13 (Fig. 1).
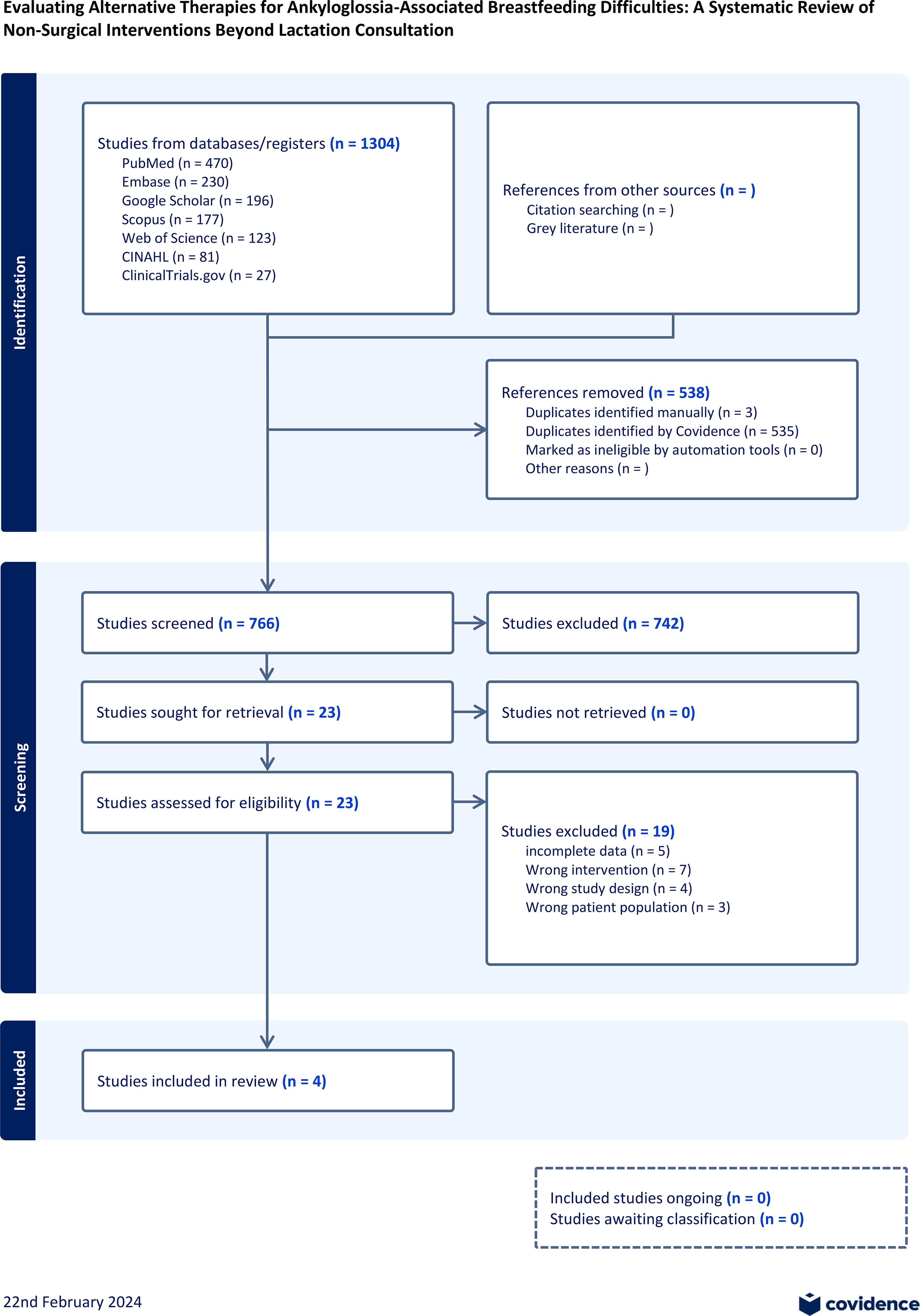
Prisma flow diagram.
Study population and interventions
Studies were published between 2016 and 2022, with patient N ranging from 1 to 171, age range: 0–6 months. Countries of origin included Spain (N = 2), United Kingdom (N = 1), and Australia (N = 1). Two studies had the same first author [Ferrés-Amat et al.’s (2017) cross-sectional study and 2016 case report].10–11 Two articles were cross-sectional (Ferrés-Amat, 2017, and Miller 2017), one case report (Ferrés-Amat, 2016), and one case series (Greenwood, 2023).10–13 Two out of four studies included predominantly female patients (55.6–56% of patients), while the remaining two studies, both by Ferres-Amat et al., included more male patients (64.9% male in the cross-sectional study; one male infant in the case report).10–13 Lactation consultation was an intervention in two of four studies.10–11 Frenotomy was performed with myofunctional therapy (MFT) (two of four) or combined with osteopathic (Greenwood et al.) and chiropractic manipulation (Miller et al.).10–13 The detailed characteristics of the included study are shown in Table 1.
Study Characteristics.
In two studies, only a subset of patients had a diagnosis of ankyloglossia (AG).
Descriptive data
The cross-sectional study by Ferrés-Amat et al. assessed duration of feeds at breast, weight gain, and pain using a visual analogue scale (VAS). 10 The case report by Ferrés-Amat et al. looked for maternal pain using the same VAS, weight gain over time, and length of feeds. 11 The retrospective case series by Greenwood et al. utilized the Breastfeeding Self Efficacy Score–Short Form (BSES-SF), and maternal breast pain VAS score (scored from 0 to 10). 12 The BSES-SF is a validated scale, consisting of 14 questions on a 5-point Likert scale, scored from 0 to 70. A VAS (rated from 0 to 10) completed by parents at clinic intake were also used to estimate “noisiness” of the child after feeding, ability to latch to breast, and sustain latch on breast. A high score indicated worse symptoms for pain and noise, whereas a low score indicated poorer latch and poor sustenance of latch. 12 Miller et al. scored “feeding difficulties” as reported by mothers using an 11-point scale they reported having validated in a previous study, 14 scored from 0 (no feeding problem), 5 (moderate problem), to 10 (serious problem). 13
Assessed outcomes
Ferrés-Amat et al.’s cross-sectional study allocated all patients to receive lactation consultation initially. If difficulties persisted, MFT was recommended. If MFT was ineffective, patients were offered frenotomy. This study reported that 33 of 171 (19.3%) cases of breastfeeding problems and AG were resolved by lactation consultation alone; 50 of 171 (29.2%) cases were resolved by both lactation consultation and MFT, while 88 of 171 (51.5%) cases proceeded to frenotomy. 10 The authors classified patients into “mild”, “moderate”, or “severe” based on the presence of clinical criteria (one or more of poor weight gain, long breastfeeds, and maternal pain) and Coryllos classification. 10 Among those the authors categorized as “mild,” only 14% of patients underwent frenotomy, whereas in the “moderate” group, 40% of patients had frenotomy, and in the “severe” category, 65% of patients underwent frenotomy. 10
In Greenwood et al.’s study, patients with AG could not be separately analyzed. Among 18 dyads, 10 reported AG diagnosis prior to study inclusion, with 9 having prior frenotomy. BSES-SF was administered, with scores ≤50 indicating a heightened risk of breastfeeding cessation. 12 Postintervention, BSES-SF scores significantly increased for participants with both not at-risk baseline scores (>50) (p = 0.005) and at-risk (≤50) baseline scores (p = 0.022). The percentage of dyads expressing confidence in breastfeeding across all 18 dyads rose from 5.5% to 72.2% at discharge. Reductions in pain and noise (p = 0.006 and p = 0.009, respectively) and improvements in the ability to latch and maintain latch (p < 0.001 for both) by VAS were observed in the entire group. 12
Miller et al. collected data via surveys from mothers, enrolling 131 infants over 5 months, with 51 reporting AG diagnosis before study inclusion. The mean “feeding difficulty” score reduced from 4.6 to 1.1 after approximately four chiropractic sessions, with discharge from care upon resolution reported by mothers. They quote an average improvement of 76% over those sessions. 13 Again, those with AG could not be separated.
Breastfeeding time, breastfeeding difficulties/comfort, VAS, BSES-SF
Ferrés-Amat et al.’s cross-sectional study provided parental reports of pretreatment and posttreatment feeding duration, without a description of the interval between measurements (Table 2). 10 Breastfeeding times significantly differed between groups before treatment (p = 0.029) but not after treatment (p = 0.142). Nearly all patients in the MFT group (98%) and surgical group (97.7%) gained >100 g/week post treatment (p = 1.0). Before treatment, the groups differed in proportion, feeding directly at breast versus mixed breast and bottle (p = 0.032). Post treatment, the majority shifted to exclusive breastfeeding (87.7% of all patients, no difference between groups) (p = 0.191). The pretreatment VAS pain rating did not differ significantly between the MFT group (mean 5.10, standard deviation [SD] 3.27) and the surgical group (mean 5.33, SD 3.07) (p = 0.153). Posttreatment pain was improved in both groups and again did not differ between groups (MFT group 0.98, SD 1.46; surgical group 0.81, SD 1.25) (p = 0.597). 10 Statistical comparison of changes in within-group scores were not provided.
Ferres-Amat Case–Control Breastfeeding Times.
Note that the groups differed before treatment, with the frenotomy group having a higher proportion of patients requiring 60+ minutes per feed.
The Ferrés-Amat case report examined a 17-day-old male with Coryllos grade II AG (fine/elastic frenulum, 2–4 mm from tongue tip to floor of mouth, close to alveolar ridge). Initial maternal pain VAS was 10 (maximum score), weight gain <100 g/week, parental reported feeding time >60 minutes, with “poor latching and unproductive sucking.” Lactation consultation was initiated. Simultaneously, MFT was offered, stimulating sucking and rooting reflexes, along with conducting intraoral and extraoral exercises. Twenty-minute MFT sessions were conducted twice weekly for 1 month. The family was provided home exercises (six repetitions performed at least three times daily). Frenotomy was performed at 21 days of life. After combined frenotomy, MFT, and lactation consultation, maternal pain decreased from 10 to 5 (VAS), weight gain improved to 200 g/week, and parental reported feeding time was 30 minutes at 5 weeks. At 9 weeks, maternal pain was 0, weight gain 200 g/week, and feeding time was 15 minutes. 11
Greenwood’s retrospective series described osteopathic intervention in 18 breastfeeding dyads including 10 with AG diagnosis prior to study inclusion (9 with previous frenotomy). These patients could not be separated from those without AG. The study objective was to determine if osteopathy improved breastfeeding difficulties in general. Patients with AG were included if breastfeeding symptoms were reported to have persisted despite frenotomy and the recommended post frenotomy exercises (in the nine having frenotomy). Interventions were provided over 7.4 weeks (treatment number range 3–7). Several VASs were utilized (maternal pain, breastfeeding latch, and maintenance of latch, all scored from 0 to 10) and BSES. The VASs were not validated, whereas the BSES is validated. 15 A significant difference in BSES score preintervention (median 52) to postintervention (median 64) (median change 11, interquartile range 8–15) was reported (p < 0.001). Among patients with frenotomy, only one out of nine fell into the category of “at risk for breastfeeding cessation” (BSES < 50), whereas the majority did not. VAS pain scores significantly improved from pre- to postintervention (2.3–0, p = 0.006). Latch VAS score changed from 5.6 to 9 post intervention (p < 0.001). The “maintenance of latch” VAS score changed from 4 to 8.5 post intervention (p ≤ 0.001). 12 The subset of patients with AG was not separately analyzed. No harms were reported. 12
The goal of the Miller cross-sectional study was to determine the frequency of AG diagnosis in patients presenting for chiropractic care with “breastfeeding difficulties”. A mean “score of feeding difficulties” was reported in 131 infants. The study population included 51 patients with report of prior AG diagnosis. Of those patients, 77% (39/51) had previous frenotomy. At intake, the mean score in all patients was 4.6, and 1.1 at follow-up, without statistical comparison. 13 Patients with AG diagnosis were not analyzed separately.
Assessment of risk of bias
The NOS, scored out of a maximum of nine points, was used to assess risk of bias in the included studies. Greenwood et al. indicated the potential existence of selection bias. 12 Ferrés-Amat et al.’s 2017 cross-sectional study was scored 7 out of 9 points (“good” quality study); Greenwood et al. and Miller et al. were scored 5 out of 9 and 3 out of 9 points (“fair” quality studies), respectively.10,12,13 Case reports have high inherent risk of bias, and therefore Ferrés-Amat et al. was not scored. 11 The detailed evaluation is provided in Supplemental Table S1.
Discussion
AG poses challenges in both diagnosis and treatment. There are no standardized diagnostic criteria. 4 Treatment paradigms vary, and not all cases of AG require intervention. Multiple recent systematic reviews support frenotomy as a low-risk intervention in properly selected children to improve breastfeeding in the setting of AG, and this is reflected in expert consensus guideline documents.2,4,16–18 In many other surgical settings, pre- and postoperative physiotherapy has been utilized to enhance recovery, including orthopedic surgery,19–20 neurosurgery, 21 and thoracic surgery. 22 Some providers also offer detailed recommendations for pre- and postfrenotomy care, through MFT, chiropractic care, physiotherapy, and osteopathy. 23 However, existing studies on specific postfrenotomy “exercises” do not demonstrate consistent benefit, and the other modalities have limited literature.16,24
This systematic review evaluated alternative therapies, including MFT, chiropractic care, and osteopathy, for infants with AG and breastfeeding issues. The included studies reported improvements. However, methodological flaws, including absence of control groups, made it difficult to discern if improvements resulted from the intervention, placebo effect, or time alone, which prevents definitive conclusions. This highlights the need for more well-designed studies with appropriate control groups.
Our findings differ from a previous systematic review examining MFT for AG, which considered indications beyond breastfeeding, such as sleep apnea, “tension,” and speech issues. 25 While the prior review suggested frenotomy’s superiority over MFT alone, they suggest improved outcomes with a combined approach. Some studies from the previous review met our inclusion criteria.10–11 Our specific focus on breastfeeding improvement prevented definitive conclusions about alternative therapies, contrasting with prior findings.
Expert consensus advises evaluating latch issues and addressing any concurrent medical conditions that could exacerbate breastfeeding challenges prior to any surgical therapy.26–27 Both the 2020 AAO consensus statement and the 2021 Academy of Breastfeeding Medicine (ABM) position statement discourage postfrenotomy massage and exercises owing to insufficient evidence.4,16 The ABM underscores the importance of clinical follow-up to offer ongoing breastfeeding support as necessary. Skilled lactation support, including latch and position adjustments, temporary nipple shields, and expressing breast milk, can address many breastfeeding challenges, and these evidence-based approaches should be central to optimizing breastfeeding.
The Ferrés-Amat approach aligns with established guidelines, offering noninvasive interventions initially and surgery only if deemed necessary. Lactation consultation, their initial step, is supported by strong evidence of effectiveness. 28 MFT followed in patients failing lactation consultation alone, and frenotomy followed. However, the study did not aim to prove the efficacy of MFT or allow a comparison between approaches owing to baseline differences between groups. While the study design currently precludes definitive conclusions about efficacy, no adverse effects were observed. Nevertheless, recommending MFT based on existing evidence is not possible at this time based on existing literature.
Miller’s study investigated a possible link between AG and breastfeeding difficulties, suggesting chiropractic treatment’s potential benefit based on participant reports. 13 However, the study’s limitations, including its descriptive nature, patient reports of previous AG diagnosis, and grouping of these patients into the larger group of patients with “breastfeeding difficulty,” hinder definitive conclusions regarding the efficacy of chiropractic care in AG. The scale described in the study, although reported to have been validated by the authors, is not a standard scale used in other literature. The study design has significant potential for placebo effect. Stronger evidence is needed to confirm the true prevalence of AG, the effectiveness of frenotomy, and the role of chiropractic treatment in this context. There are a few studies that suggest chiropractic care may improve breastfeeding, particularly for issues linked to musculoskeletal problems and biomechanics, when combined with other support like lactation consultants.29–30 However, these studies do not evaluate AG. In addition, although there are no complications reported in this patient series, there are case reports of serious vascular complications in adults after cervical manipulation.31–32 Theoretical risks associated with spinal manipulation should be carefully considered before recommending chiropractic care in infants.
Greenwood et al. showed significant differences in BSES and VAS scores (for latch, maintenance of latch, breast pain, and noisiness of feeding) before and after intervention with the use of osteopathic measures. 12 After a median of five osteopathic treatments over 7.4 weeks, all 18 mother and infant dyads (including 10 with AG) reported improvements in all scores. This analysis brings forth several concerns. Firstly, AG was not formally diagnosed within the study but rather reported by parents. Data, therefore, is lacking regarding the accuracy of the diagnosis and the classification and severity of AG. The inability to separate data specifically for patients with AG adds an additional layer of complexity. This challenge is shared by Miller et al. The lack of a control group makes it difficult to conclude that observed improvements were attributable to therapy versus placebo effect, frequent follow-ups, or simply time. VAS measures collected were completed by parents rather than blinded raters, which also may confound results. Though we cannot draw strong conclusions based on the included study, osteopathy warrants more study. A previous single-blind, RCT examining osteopathic manipulation for breastfeeding difficulty, excluding patients with AG, did find significant improvement in several scores including VAS for pain in the osteopathic manipulation therapy (OMT) group. 23 Focused research in AG is specifically required.
The BSES-SF assesses psychological confidence. It is influenced by various factors and is not always indicative of breastfeeding success. 33 Lactation consultation for latch optimization has demonstrated improvement in BSES-SF scores. 33 In addition, scores may improve over time without intervention, which is also observed in VAS breast pain scores. 33 Considering the time interval between measurements in the studies,11–12 changes in VAS and BSESs may partly reflect the passage of time alone.
Future research should include more robust multiarm randomized trials. This would help clarify whether alternative therapies can be viable substitutes or adjuncts for frenotomy, identify potential patient subgroups who might benefit most from specific approaches, and explore if combining frenotomy with an alternative therapy enhances outcomes.
There are several limitations to this systematic review. There were few studies with varied methodologies, preventing meaningful comparison or meta-analysis. The patients included in the study did not uniformly have description of AG using descriptive criteria or tools. Furthermore, the exclusion of non-English studies and the inability to separate patient groups, including those with AG, from more general breastfeeding difficulties, contribute to the overall limitations of this review.
Conclusion
The included studies examining MFT, OMT, and chiropractic therapy all report improvement in breastfeeding metrics. However, it is not presently possible to attribute these improvements to the intervention alone. While no harm is reported in any study, the possibility of delaying definitive management and costs of care require careful consideration. Further research is crucial to clarify their role and ensure optimal care for patients with AG.
Footnotes
Authors’ Contribution
R.C. methodology, investigation, data curation, writing (original draft); S.K. data curation, formal analysis, validation, writing (review and editing); J.L. investigation, data curation, writing (review and editing); R.A. investigation, data curation, writing (review and editing); C.M.L. validation, supervision, writing (review and editing); M.E.G. conceptualization, methodology, validation, supervision, writing (review and editing); R.C. conceptualization, methodology, investigation, writing (original draft); S.K. methodology, formal analysis, data curation, validation, writing (review and editing); J.L. investigation, writing (review and editing); R.A. conceptualization, investigation, writing (review and editing); C.M.L. methodology, validation, writing (review and editing); M.E.G. conceptualization, methodology, formal analysis, validation, writing (original draft and review and editing), supervision.
Disclosure Statement
None of the authors have any conflicts of interest to report.
Funding Information
There are no sources of funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.