
Abstract
Objectives:
To describe the implementation of a successful two-week virtual breastfeeding elective for medical students during the COVID-19 pandemic and characterize student demographics, objective knowledge, and perspectives on breastfeeding before and after the elective.
Study Design:
We adapted the Santa Rosa Kaiser Permanente Family Medicine breastfeeding residency curriculum to create a two-week virtual medical student elective using Kern’s six steps of curriculum development and a competency-based education framework. Educational components included self-paced modules, shadowing experiences, and group didactics. Objective knowledge was assessed with multiple-choice tests before and after the elective compared using a paired t-test. Reflective writing pieces were qualitatively analyzed using the six phases of thematic analysis developed by Braun and Clarke.
Results:
From 2020 to 2023, 40 medical students completed the elective. Breastfeeding knowledge increased significantly from the pre-test 72% (95% CI: 52–92%) to post-test 91% (95% CI: 81–100%) (p < 0.001). Over 90% of students felt that learning objectives were met well or very well and agreed or strongly agreed that the elective increased their knowledge and confidence in providing anticipatory guidance to breastfeeding parents. Similar themes were shared across students’ reflective writing pieces, with nearly 30% (n = 23) of the student essays addressing socio-cultural and racial differences in beliefs surrounding breastfeeding.
Conclusion:
A virtual breastfeeding curriculum for medical students is well-received by stakeholders (patients, lactation consultants, students, etc.) and improves breastfeeding knowledge and confidence. A virtual elective is an innovative and effective way to deliver breastfeeding education and can be used even when institutional breastfeeding or lactation support is unavailable.
Inclusive Language Statement
At the time of this study, the terms “breastfeeding” and “mother” were used. However, we acknowledge all forms of lactation, including chestfeeding, and recognize that not all people who give birth and lactate identify as female.
Introduction
Human milk is the preferred nutrition for infants, and prolonged, exclusive breastfeeding is well-documented to benefit both mother and child. 1 The World Health Organization (WHO) recommends breastfeeding within the first hour of life, exclusive breastfeeding for six months, and continued breastfeeding support until at least two years of age. 2 However, in 2020, the national average of exclusive breastfeeding at six months for infants in the United States was only 25.4%. 3 Racial disparities in breastfeeding are particularly striking in the United States, with initiation rates for Black (77.1%) and Native American (82.3%) groups and continuation beyond ten weeks for Black (57.2%) and Native American (60.5%) groups ranking the lowest among all races. 4
Despite the Surgeon General’s call for improved breastfeeding education for health care professionals at all levels of training, standardized requirements for breastfeeding education in medical training are lacking. 5 In 2011, the Academy of Breastfeeding Medicine (ABM) published guidelines for the integration of core competencies in breastfeeding and lactation into undergraduate and graduate medical education. 6 However, these guidelines are not widely adopted. An extensive review and survey of a preclinical undergraduate medical curriculum in the United States revealed that core competencies in breastfeeding were either covered superficially or not at all, and the majority of medical students were not comfortable with basic breastfeeding medicine. 7 Post-graduate training faces a similar problem. The Accreditation Council for Graduate Medical Education (ACGME) requires that residency programs meet core competencies in breastfeeding education for accreditation. 6 Disappointingly, surveyed program directors report that breastfeeding education is only provided for a median of nine hours for pediatrics programs, eight hours for family medicine, and 23 hours for obstetrics and gynecology (OB/GYN) over all the years of training. 8 Educational curricula designed specifically for medical students and residents are essential to address the need for improved education.
Educational programs for breastfeeding date back to 1977 when the San Diego Lactation Program began training healthcare students and professionals. 9 By 1985, the program was incorporated as Wellstart, an independent non-profit organization funded by the United States Agency for International Development. 9 In 2010, the American Academy of Pediatrics (AAP) developed a breastfeeding residency curriculum based on the second edition of the Wellstart Lactation Management Self-study Modules. 10 These curricula were designed for integration into pediatrics, OB/GYN, and family medicine residency programs. 10 Currently, there is no similar standardized educational curriculum for undergraduate medical education. 5
Traditionally, undergraduate medical education involves group didactics and in-person clinical experiences. 11 However, during the COVID-19 pandemic, the Association of Medical Colleges recommended suspending all direct patient contact responsibilities for medical students. 12 Virtual education became the primary teaching modality during the early part of the pandemic and continues to be used in conjunction with in-person activities. 13 Looking ahead, a blend of virtual and traditional in-person learning is expected to play a significant role in medical education. 13 This transition calls for the development and sharing of online teaching resources to support learning across medical institutions. 13
The goal of this work is to describe the experience of implementing a successful two-week virtual breastfeeding elective for medical students during the pandemic and to characterize outcomes and curriculum receivables, including student demographics, objective knowledge gained, and perspectives on breastfeeding.
Methods
Participants and setting
From 2020 to 2023, 40 medical students from a four- or five-year pathway at a medical school in an urban, Midwest city enrolled in a two-week virtual breastfeeding elective as part of their clinical education. Inclusion criteria for participation in the elective included completion of core clerkships in Pediatrics and OB/GYN. To ensure small group interactions, each elective offering was limited to three to seven students. Institutional review board exemption was obtained for this review.
Educational components
The initial breastfeeding curriculum was adapted with permission from the Kaiser Permanente Santa Rosa Family Medicine Breastfeeding Elective curriculum which was shared online. The AAP Breastfeeding Curriculum was reviewed, but its use was limited due to ongoing revisions and the unavailability of its websites and curriculum. 14 As a result, the course faculty designed a large part of the elective using Kern’s six-step approach to curriculum development and the competency-based education framework.15,16 The elective was continuously revised based on feedback from students and senior faculty educators. The syllabus included pre- and post-tests, self-guided modules, group sessions, and virtual shadowing of lactation consultants (LCs) and breastfeeding medicine physicians.
Pre/post-testing
The AAP Breastfeeding Curriculum pre- and post-tests were distributed to assess students’ knowledge about breastfeeding and clinical practice before and after completing the modules. 14 The pre-test (25 questions) was completed before the first group session, and the post-test (25 questions) was completed before the last group session.
Asynchronous, independent work
The syllabus included 82 links, consisting of videos, websites, and virtual resources from nonprofit organizations, public health organizations, academic centers, and local hospitals. Students completed or reviewed three resources in each of the following five ACGME Core Competencies, totaling 15 modules: (1) Medical Knowledge, (2) Patient Care, (3) Interpersonal Communication Skills, Professionalism, and Disparities/Cultural Considerations in Breastfeeding, (4) Systems Based Practice, and (5) Practice-Based Learning. Each competency included a list of learning objectives to guide the students (Table 1).
ACGME Learning Objectives by Core Competency
Synchronous, interactive group sessions
Students attended three virtual interactive group sessions. The first session consisted of course introductions and an interactive presentation on common breastfeeding positions and issues. The second session was an interactive case-based didactic showcasing common clinical scenarios such as jaundice, nipple pain, and engorgement. In the final session, students presented on an evidence-based topic of their choice.
Virtual shadowing with lactation consultants (LCs) and breastfeeding medicine physicians
Students virtually shadowed either individual or group appointments with LCs, addressing common breastfeeding concerns. All lactating patients granted permission for the students’ presence, and students joined from a private location to ensure patient privacy. In-person shadowing experiences were later offered in the Breastfeeding Medicine Clinic (established in 2022) with the course faculty.
Reflective writing assignments
Students were asked to complete two one-page reflective writing pieces by the end of the elective. A rubric was provided with criteria on knowledge and reflection, logical organization of thoughts and content flow, and grammar and writing style. Although students could choose any topic related to breastfeeding, writing prompts were also provided (Supplementary Appendix Data S1).
Educational presentation or handout
Each student researched, prepared, and presented a 5-minute topic of interest in the form of a presentation, patient education handout, or a clinical case study. A rubric with criteria on content and design, use of reputable and variable resources, and oral presentation style was provided for guidance and grading.
Course evaluation
Upon completion of the elective, students filled out an anonymous evaluation form. The form assessed how well course learning objectives were met, satisfaction with course facilitators, effectiveness of instructional materials and didactics in increasing knowledge and confidence in giving anticipatory guidance, subjective engagement with the elective, and the most and least effective components of the elective. The evaluation used a 5-point Likert scale and free-response questions.
Statistical analysis
Each pre- and post-test was graded as percent correct out of 25 questions. 14 Breastfeeding knowledge and confidence of learners were compared using paired-sample t-test of raw test scores. Reflective writing pieces were qualitatively analyzed using the six phases of thematic analysis developed by Braun and Clarke. 17 The identified themes were then grouped by the five core competencies. Student demographic information was self-reported based on the AAP pre-test and course evaluation questions and summarized with descriptive statistics. Race was collected to characterize the racial and ethnic diversity of the students who chose to participate in this elective. All analyses were conducted in the software R (Vienna, Austria).
Results
A total of 40 students completed the elective between 2020 and 2023, and all students turned in elective materials. Most students (86%, 24/28) were in their fourth year of medical school, female (92%, 35/37), and had diverse specialty interests. Students self-identified with diverse racial and ethnic backgrounds, including American Indian/Alaska Native (3%, 1/37), Asian (16%, 6/37), Black/African American (16%, 6/37), Hispanic or Latino (11% 4/37), and White (49%, 18/37). Two students self-identified as “Other” (Table 2).
Student Voluntary Self-Reported Demographic Characteristics
Predefined choices for student demographics prevented separate reporting of race and ethnicity and specification of “Other.”
The mean pre-test score increased from 72% (95% CI: 52–92%) to 91% (95% CI: 81–100%) on the post-test (p < 0.001). The percentage of students reporting confident or very confident in their ability to address parents’ questions about breastfeeding increased from 5% (2/37) before the elective to 62% (17/27) after the elective. Similarly, students reporting confident or very confident in their ability to competently manage common breastfeeding problems increased from 8% (3/37) to 62% (17/27) (Fig. 1). Following the elective, 91% (29/32) of students indicated that breastfeeding education would be influential or very influential in their future care for mothers and babies.
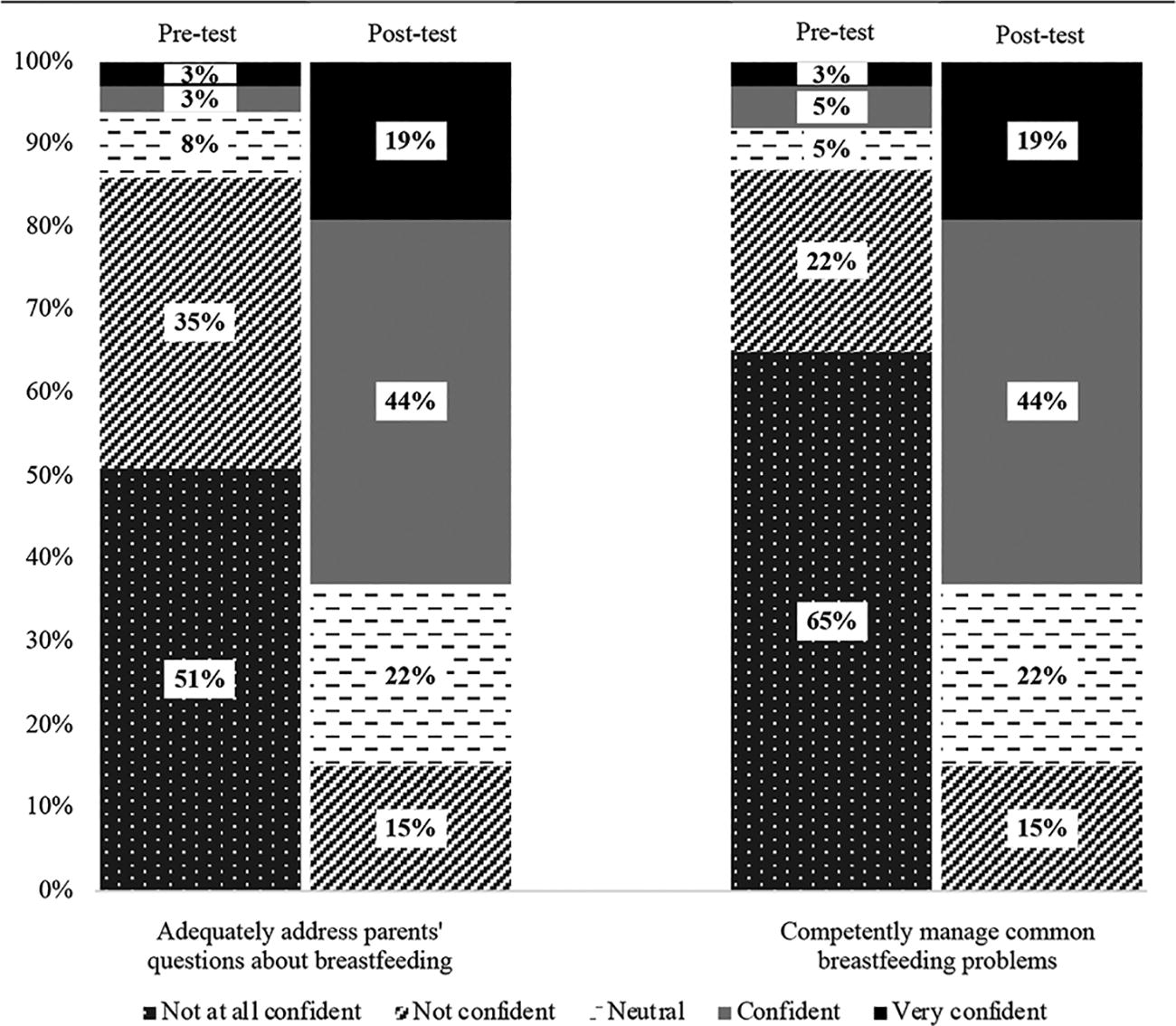
Students' self-perceived confidence in providing anticipatory guidance to patients. Students rated confidence in “addressing parents’ questions about breastfeeding” and “competently manage common breastfeeding problems” on pre- and post-tests. Confidence was measured on a Likert scale with a range from 1 = “not at all confident” to 5 = “very confident.”
Student reflective writing pieces demonstrated the integration of course material and personal experiences. The ten most frequently mentioned themes are presented in Table 3 and are categorized by the five core competencies. Nearly 30% (23/80) of student essays reflected on the socio-cultural and racial differences in beliefs surrounding breastfeeding.
Reflective Writing Top Ten Most Common Themes by ACGME Core Competency a
Each student wrote two reflective writing pieces for a total n = 80.
Calculated as number of essays that mentioned theme divided by n.
Reflective writing pieces also included themes related to the Medical Knowledge core competency, but they did not rank among the top ten most common themes.
From the course evaluation, each of the three overall course learning objectives was considered to be met either well or very well by 97%, 92%, and 95% of the students, respectively (Fig. 2). All students (100%) indicated that the instructional material and didactics increased their knowledge and confidence in giving anticipatory guidance to parents about breastfeeding. In addition, all 40 students felt engaged, involved, and would recommend the course to their peers. Student comments identified virtual visits with LCs as one of the most effective components of the course. Students also provided feedback on the completed modules, highlighting those that were helpful and identifying others as redundant or obsolete.

Student evaluation of overall course learning objectives. Students scored how well each of the three-course learning objectives was met on the course evaluation form. Scores were measured on a Likert scale with 0 = Not Covered, 1 = Poor, 2 = Fair, 3 = Average, 4 = Well, 5 = Very Well. All students chose scores of three or higher.
Discussion
This study demonstrates that a multicomponent two-week virtual breastfeeding elective is well-received and significantly improves learning outcomes. The significant improvements in both objective knowledge and self-perceived confidence suggest the effectiveness of the delivery method and curricular components in teaching knowledge and application of breastfeeding medicine.
Our multicomponent elective comprised of self-study modules, group sessions, and shadowing stands apart from previously described single-component interventions that included either self-study modules or in-person clinical teaching alone.10,18–20 Interventions with similar multicomponent educational curricula have been described at the University of New Mexico (UNM), 21 Lehigh Valley Health Network in Pennsylvania, 22 and the University of Wisconsin, Madison. 23 However, unlike our elective, these interventions were not delivered in an entirely virtual format.
At UNM and Lehigh Valley, breastfeeding curricula were designed for OB/GYN and/or pediatric residents, respectively. Both curricula included Wellstart self-study modules and hands-on sessions with lactation specialists.21,22 Our modules were curated by faculty, partly due to a lack of sustained funding for the Wellstart modules. The didactics at UNM covered topics similar to those of our interactive group sessions, including the anatomy and physiology of lactation, common breastfeeding problems for mothers and newborns, and the promotion and support of breastfeeding. 21 We opted for interactive group sessions over didactics to encourage active student participation. A unique curricular component at UNM was feeding evaluations for each mother–baby dyad during clinical rounds in the newborn nursery and the postpartum floor. 21
A different curricular approach was implemented at the University of Wisconsin, Madison, where family medicine residents attended a four and a half-hour interactive workshop comprised of didactic presentations and role-play with standardized patients. Residents were evaluated with Objective Structured Clinical Examinations (OSCEs), which consist of observed role play with standardized patients scored using an objective checklist, 30 days before and after the workshop. 23 Neither our intervention nor those described at UNM or Lehigh Valley included practice with standardized patients or OSCEs. Standardized patients are useful educational tools that allow learners to practice new skills as they transition into clinical practice. 24
Interventions at UNM, Lehigh Valley, and University of Wisconsin, Madison all demonstrated positive outcomes following the educational intervention.21,22 Specifically, at Lehigh Valley, patients treated by residents who completed the intervention were twice as likely to continue exclusive breastfeeding through six weeks post-partum compared with those patients who were treated by the residents prior to the breastfeeding education intervention. 22 Residents at UNM self-reported improvements in knowledge, and found the curriculum very helpful in providing support for breastfeeding mothers. 21 At the University of Wisconsin, Madison, residents improved in the evaluation and diagnosis of common breastfeeding problems and reported increased confidence in their skills. 23 Similarly, students who completed our elective self-reported improved confidence in providing anticipatory guidance and demonstrated objective improvement in breastfeeding knowledge.
Although each of these interventions was successful, the authors at UNM also highlighted challenges in implementing the in-person elective. Listed barriers were: high demands on faculty time, difficulty coordinating sessions, and insufficient time for learners to engage in hands-on clinical experiences and complete the recommended modules. 21 Virtual delivery of educational experiences may alleviate the challenges of in-person interventions.
At the onset of the COVID-19 pandemic, the abrupt transition from in-person to virtual education forced faculty and students to quickly adapt to the changing environment and find new ways to teach and learn. 12 Completion of asynchronous modules allowed students to tailor their own learning experiences and spend time engaging with materials of interest. The synchronous component of the elective included three interactive group sessions, creating a strong “social presence” among students and faculty. We believe that the blend of virtual delivery methods and the incorporation of various learning methods in our curriculum contributed to the successful evaluations of the elective. All students (100%) indicated that they agreed or strongly agreed that they were engaged and involved in the material.
Although active engagement is crucial for knowledge acquisition, the translation of classroom knowledge to clinical care presents a significant challenge in virtual learning. 25 To address the translation of knowledge, students shadowed LCs and observed how classroom knowledge is applied to clinical care. Students evaluated this experience highly, ranking it among the best components of the elective. Although it is impossible to replicate the experience of in-person clinical skills training in a virtual curriculum, online education prepares students for telehealth practice and provides extra time for refining clinical reasoning skills. 11 To address the need for hands-on experience, in-person shadowing opportunities in the Breastfeeding Medicine Clinic and lactation support groups were offered in summer 2022 and fall 2023, respectively, due to relaxed COVID-distancing measures. Future offerings of this elective will include more in-person opportunities. 25
Our elective curriculum was developed by expert faculty in breastfeeding medicine with attention to local and systemic health disparities. The modules mirrored the structure of the AAP residency curriculum and included videos, case studies, presentations, AAP policy statements, and external references incorporated from the AAP curriculum. 14 The school campus and surrounding affiliated hospitals where students conduct clinical rotations are located in an urban city with significant health disparities between different racial groups and high infant and maternal mortality rates in the Black populations. 26 We included resources from local hospitals and public health organizations in the modules to highlight the importance of racial disparities and cultural considerations in breastfeeding. Nearly 30% (n = 23) of the student essays explored the sociocultural and racial differences in beliefs surrounding breastfeeding, demonstrating increased attention, awareness, and interest in this theme. Two medical students who identify as Black and Native American felt empowered to write on this topic after learning about historic and current disparities in breastfeeding in their identified backgrounds for the first time. 27 Understanding racial disparities, combined with reflective practice, enhances students’ abilities to counsel patients in an empathetic and patient-centered way. 27
Key factors for successful elective implementation include early and consistent buy-in from all stakeholders, including students, LCs, physicians, patients, medical school leadership, etc. Faculty interest and dedication were additional factors; we believe that the faculty directors, having professional and personal experiences or challenges with breastfeeding, contributed to the elective’s success. Students who took this elective were engaged, and 43% planned to pursue specialties in OB/GYN, pediatrics, or family medicine, where they will likely care for breastfeeding patients. Students were also motivated to engage in this elective to gain knowledge for themselves, family, and friends. This is crucial, given physician women have lower breastfeeding rates than the general population, often related to barriers like inflexible schedules, short duration of maternity leave, and financial losses.28,29 Upon learning of this elective, pediatric residents and practicing pediatricians attended group sessions when their schedules allowed. Unexpected positive outcomes also included interest in and development of a pediatric resident breastfeeding curriculum and elective, along with partial use of the elective syllabus for healthcare clinician training for a hospital’s Baby Friendly certification status.
Implementation of this virtual elective posed several challenges, including frequent changes or removal of websites and resources, necessitating constant revisions of the links in the syllabus. Additional difficulties included a lack of protected faculty time to create, direct, and revise the course and a lack of administrative help in registration, course material distribution and collection, virtual meeting logistics, and student evaluation completion. The elective could only be offered a few times a year, as elective dates were chosen around faculty clinical shifts and students’ schedules. We were unable to accommodate at least 50 other students who expressed interest in taking the course due to scheduling challenges or other reasons. There were limitations in reporting race and ethnicity separately due to the pre-test’s use of predefined options, rather than allowing free responses.
Future directions could involve a comparison of undergraduate and graduate trainee outcomes, including those from the pediatric resident breastfeeding elective added in 2023, standardized patient encounters, and clinical opportunities. It would also be helpful to assess outcomes in elective participants’ and their patients’ breastfeeding success using tools like a breastfeeding self-efficacy tool or metrics like breastfeeding initiation and duration. This curriculum could be adapted to various institutions and trainees around the world to meet local contexts, cultures, and learner and patient needs. 14
Conclusion
A virtual breastfeeding curriculum for medical students is well-received by students and improves objective knowledge test scores and self-reported confidence in giving anticipatory guidance to new parents about breastfeeding. Beyond gaining clinical knowledge, students also reflected on topics of special importance to them, with many focusing on social determinants of health. This work adds to the current literature by demonstrating the effectiveness of virtual educational material for medical students with the goal of improving breastfeeding education. Future work should address how this curriculum could be adapted in other settings and countries and ultimately impact clinical outcomes.
Footnotes
Authors’ Contribution
S.K.L. co-founded and co-directed the educational elective and curriculum, conceptualized and designed the study, designed the data collection instruments, collected data, conducted data analysis, drafted the initial article, and critically reviewed and revised the article. J.M.W. carried out data analysis, drafted the initial article, and critically reviewed and revised the article. H.S. is a co-director of the educational elective and critically reviewed and revised the article. L.L. carried out the initial analyses and critically reviewed and revised the article. L.F. co-founded and co-directed the educational elective and critically reviewed and revised the article. All authors approved the final article as submitted and agree to be accountable for all aspects of the work.
Author Disclosure Statement
Dr. S.K. Lam receives paid speaking fees from the Ohio Lactation Consultant Association and the Institute for the Advancement of Breastfeeding and Lactation Education. Dr. H. Szugye receives paid speaking fees from the Institute for the Advancement of Breastfeeding and Lactation Education. Dr. L. Furman receives a stipend as an Associate Editor for Pediatrics. Other authors have no disclosures.
Funding Information
No funding was secured for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.