
Abstract
Introduction:
Human breast milk macronutrients play a vital role in the development of breastfed infants and are known to be influenced by several factors. There is limited information on the influence of cannabis use during lactation on these macronutrients. Given the rising use of cannabis among lactating women with its widespread legalization, this study aimed to examine the association of cannabis use during lactation on breast milk macronutrients.
Materials and Methods:
A cross-sectional study design was used and 637 breast milk samples with measured macronutrients were utilized. Of these, 165 samples that had detectable cannabis metabolites were defined as the study group, and 472 samples from mothers who did not report cannabis use and from mothers who reported cannabis use but did not have measurable metabolites of cannabis in their milk samples were defined as the control group. Multivariable linear regression models were used to assess the association of presence of cannabis metabolites with protein, carbohydrates, fat, and calories in breast milk.
Results:
Greater protein levels (95% confidence interval [CI]: 0.112–0.376; p < 0.001) and lower fat levels (95% CI: −0.217, −0.018; p = 0.020) were found in the milk exposed to cannabis compared with reported nonexposure. The presence of cannabis was associated with an increase of 0.244 mg/dL in protein and a reduction of 11% in fats in breast milk. The levels of energy and carbohydrates were not significantly different among the two groups.
Conclusions:
This study demonstrated a statistically significant association between the presence of metabolites of cannabis in breast milk and protein and fat concentrations in breath milk. Further studies are required toward building the body of evidence to determine safety of cannabis use during lactation.
Introduction
Medical and scientific communities have identified the tremendous benefits of breast milk for newborns and infants. The World Health Organization recommends exclusive breastfeeding for the first 6 months of life. 1 The macronutrients in breast milk, namely carbohydrates, proteins, and fats, are crucial for the growth and development of infants in their first year of life.2,3 Besides supplying energy and nutrition for infant growth and development, the macronutrients in breast milk contribute in several ways to the development of the nervous system, gastrointestinal system, and immune system.4–6
Proteins in human milk are sources of essential amino acids that form the building blocks of muscle cells, neurotransmitters in the central nervous system, and antioxidative biochemicals.3,4 Proteins are essential prebiotics in the colon.2,4–6 Proteins are sources of immunoglobulin A (IgA) and lysozymes, which concentrate the intestines of breastfed babies where they protect the intestines from ingested pathogens. In addition, proteins serve in bone remodeling.2,4–6
Fats in human milk are sources of bioactive compounds crucial for the construction of cell membranes. Newborns require large amounts of this compound for the quick growth of organs.2,5 Fats are true prebiotics, and aid in the maintenance of intestinal mucosa. 4 Fats are very important for the growth and maturation of the baby’s brain and eyes, particularly in the first few months of life.2,3,5 Carbohydrates form the largest component of human breast milk and are the largest source of calories for infants. 2 The non-nutritive bioactive components of carbohydrates called human milk oligosaccharides are powerful prebiotics and are increasingly being studied as potential determinants of long-term health status and disease risk of an individual.2,3,6
Human breast milk is a dynamic bioactive fluid that varies by maternal age, ethnicity, diet, medical and mental health, socioeconomic status, smoking status, alcohol consumption, duration of breastfeeding, time of day, and sex of infant.7–20 The objective of this study was to examine the concentrations of human milk macronutrients in relation to the presence of metabolites of cannabis in breast milk. The rationale for this study is twofold. One is that animal studies (Josan et al. and Johnson et al.) found statistically significant changes in macronutrient concentrations in breast milk of mice exposed to cannabis and detectable levels of cannabis metabolites in those breast milk samples.21,22 In addition, one study on human breast milk found altered levels of carbohydrate and IgA in breast milk exposed to cannabis. 23 Second is the rapidly changing political landscape of cannabis-related policies has made cannabis readily accessible to the public. As per the 2016 Pregnancy Risk Assessment Monitoring System data, 6.5% of surveyed women endorsed use of cannabis in the postpartum period. 24 As of 2024, 32 states have either decriminalized or legalized recreational cannabis use. 25 Cannabis consumption through vaping, oil concentrates (dabbing), edibles, and smoking has become extremely popular, with some of these products containing as much as 80% tetrahydrocannabinol (THC) compared with the Food and Drug Administration-approved medicinal cannabis that has <4% THC. Qualitative studies have indicated that women use cannabis postpartum to improve mood, and that they do not perceive cannabis to be harmful to their babies, comparing it with the effects of alcohol and nicotine on babies.26,27 The American College of Obstetrics and Gynecology, the American Academy of Pediatrics, and the Academy of Breastfeeding Medicine recommend against cannabis use during lactation.28–30 With decriminalization of cannabis, health care providers are being presented evermore with the dilemma of helping women make informed decisions with respect to cannabis use during lactation in the light of limited scientific research of consumption by the mother on the consequences for the infant. This was evident in a study where 74 lactation consultants were surveyed on their opinions and recommendations for breastfeeding with cannabis use. A total of 41% reported that their recommendation would depend on the amount of cannabis used, 44% would recommend breastfeeding despite cannabis use, and 15% would recommend not breastfeeding with cannabis use. 31
Materials and Methods
Study population
A cross-sectional study design was utilized for this study. Data for this study originated from the Human Milk Research Biorepository (HMB) at the University of California San Diego (UC San Diego) named “Mommy’s Milk.” 32 Lactating women aged 18 or older in the United States and Canada provided a milk sample and completed a semistructured telephone interview about their sociodemographic characteristics, pregnancy history, health history, breastfeeding behaviors, and medication and lifestyle exposures for the past 14 days. The study population was selected based on availability of samples with measured macronutrients (n = 756). Many women in the study provided more than one sample at different study time points. Duplicate samples after the baseline samples were excluded resulting in a final sample size of 637. Of these, 165 samples had detectable concentrations of one or more of the five cannabis metabolites and were defined as “exposure” in the study. The remaining 472 samples with measured macronutrient levels were from mothers who did not report cannabis use and from mothers who reported cannabis use in the last 14 days but did not have measurable metabolites of cannabis in their milk samples (n = 23) and were defined as “no exposure” in the study. Many women in the study provided more than one sample at different study time points (Fig. 1).
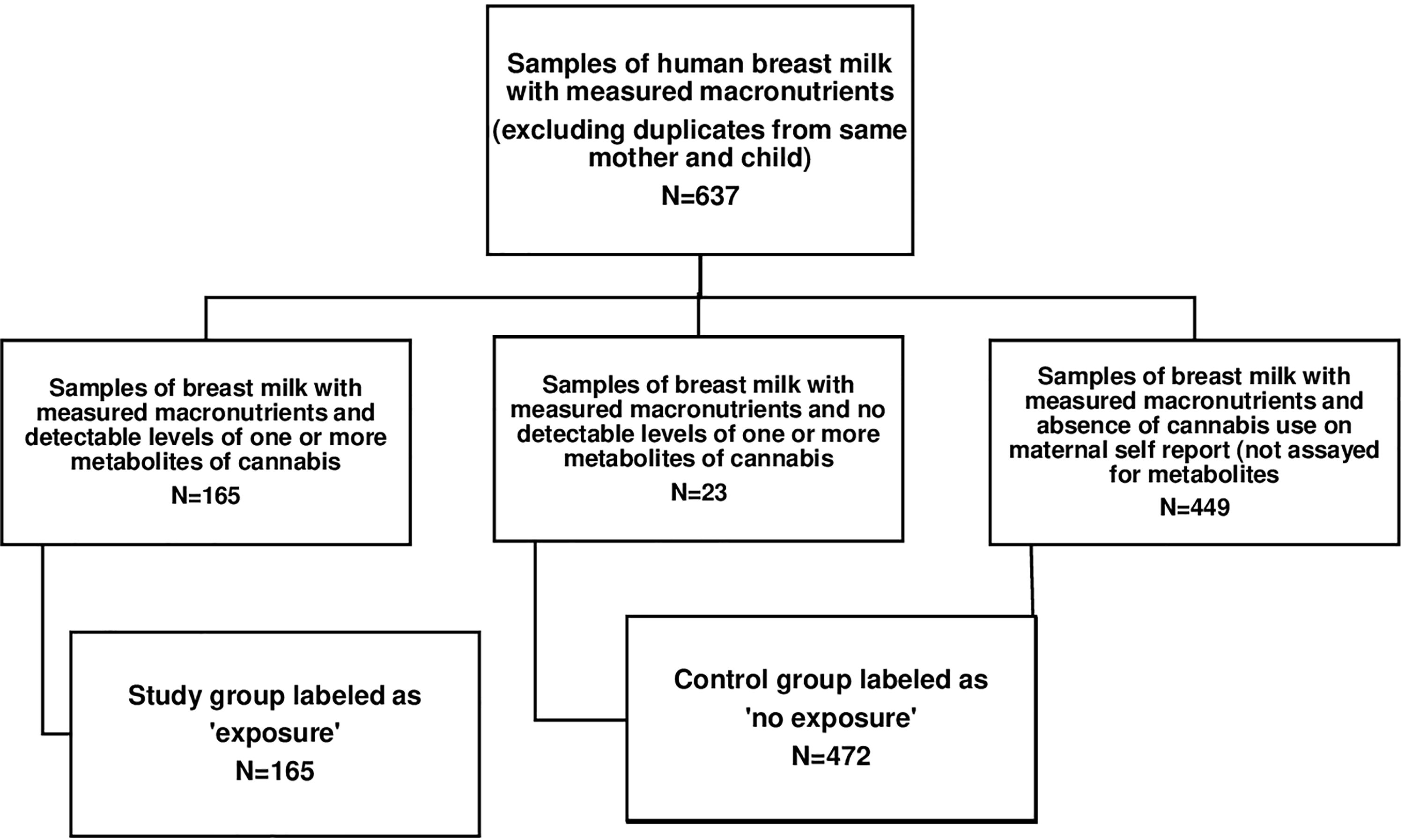
Study population.
Breast milk sample collection
Study participants collected 50 mL or more of breast milk at a local clinic or at home. Milk collected at any of the Mommy’s Milk-associated clinics/hospitals was collected from participants using a hospital-grade industrial breast pump (either the Medela Symphony or the Hygeia Enjoye) and a sterile collection kit provided by staff. Samples were transported on ice to the HMB laboratory; milk collected at home was done so with the use of a personal hand or electric breast pump and then refrigerated at 0–4°C until transported on ice to the HMB research center or picked up by courier within 24 hours of collection. Samples were stored at −80°C at HMB facilities.32,33
Measurement of cannabis metabolites
The milk samples of women who reported use of cannabis at any point while breastfeeding were analyzed for the presence and concentration of five metabolites: delta-9 tetrahydrocannabinol, cannabidiol (CBD), 11-hydroxy-delta-9-tetrahydrocannabinol (11-OH-THC), cannabinol (CBN), and the secondary metabolite tetrahydrocannabinol carboxylic acid (COOH-THC). The milk samples of women who did not report use of cannabis were not analyzed for metabolites of cannabis and presumed to be negative for metabolites in this study. The concentrations of the cannabis metabolites were measured as milligrams per deciliter of milk. Liquid chromatography was used to detect and measure the concentrations of metabolites of cannabis. 33
Macronutrient analysis
Macronutrient assays included measurements of carbohydrate (lactate), protein (casein), lipid (fatty acids) concentrations as milligrams per deciliter of milk, and calorie density of milk as calories per ounce of milk. The macronutrients were measured using point-of-care near-infrared spectrophotometry. 34 After sonification, 1 mL of milk was drawn up with an electronic pipette and expelled onto a gold transflectance chamber that was magnetically sealed carefully so as not to trap air bubbles. 34 The chamber was loaded into the SpectraStar 2400 Near Infrared (Unity Scientific, Columbia, MD) machine and spectrophotometric analysis was performed across the entire spectrum between 1,200 and 2,400 nm. Individual full spectra (1,200–2,400 nm) for each sample were compared with the reference chemistry values for each macronutrient (fat, protein, and carbohydrate) and then analyzed by Calstar software (Unity Scientific) that uses partial squares method to determine the best correlation. 34
Statistical analysis
Statistical analysis was performed using SAS Version 9.4 (SAS Institute Inc, Cary, NC). The distribution of study population characteristics was described by means or frequency depending on the functional form of the variable. The distributions of carbohydrates, fats, calories, and age of infants were found to be skewed and normalized with log transformation.
The exposure variable was categorized as “exposure” and “no exposure” based on detected metabolites of cannabis in breast milk versus no self-reported use or no detected metabolites in self-reported use. The outcome variables, concentrations of fats, carbohydrates, proteins (mg/dL), and calories (Cal/oz), were continuous variables. Relevant clinical covariates were determined through literature review. Maternal body mass index (BMI) was categorized into normal weight (BMI up to 25), overweight (BMI 25.1–30), and obese (>30) as per clinical standards. 35 Three participants who fell in the underweight BMI range were included in the normal BMI category. Maternal age and the age of the infant at the time of sample collection (reported in months) were continuous variables. Income was categorized as earning less than $60,000 and more than or equal to $60,000. Maternal education was categorized as high school, some college, college graduate, and postgraduate. Race was categorized into White and other, which included Asians, African Americans, Native Americans, and Pacific Islanders and Alaskan Americans. Ethnicity was categorized as Hispanic and non-Hispanic. Fully expressed breast milk samples (includes foremilk and hind milk) were self-reported by women as yes/no. Sample treatment was categorized as microbiome and nonmicrobiome where microbiome samples were those collected in HMB clinics supported by stringent temperature control of the sample, and nonmicrobiome samples were those collected at home. Exposures to cigarettes, alcohol, other substances, any prescription medication, and cannabis during lactation in the 2 weeks before sample collection were binary variables with yes/no values. Any self-report of depression/postpartum depression/anxiety was categorized as the presence of mood disorder. Potential confounders were identified using directed acyclic graphs (DAGs) (Fig. 2) and included maternal age, income, education, alcohol use, smoking nicotine, and mood disorder.

Directed acyclic graph for determining potential confounders.
Two-sample t-tests were first performed to assess bivariate associations of cannabis analytes with protein, carbohydrates, fat, and calories. Multivariable linear regression models were used to assess the association of cannabis metabolites with protein, carbohydrates, fat, and calories adjusted for maternal age, education, income, smoking, alcohol use, and mood disorder.
Sensitivity analysis: A multitude of factors have been known to affect the breast milk macronutrient composition.7–24 Some of these factors such as gender of the child, age of child, and degree of expression of breast milk could also affect the macronutrients in breast milk. A sensitivity analysis was performed to investigate any influence of these covariates on the study results by adjusting for these covariates in the multivariable linear regression models used for the study. In addition, a one-way analysis of variance test was performed to compare the no exposure group, the reported exposure group without metabolites, and the reported exposure group with metabolites.
Results
A total of 188 women endorsed use of cannabis in the 2 weeks before providing the breast milk sample.
Twenty-three of these women (12%) did not have detectable levels of cannabis metabolites in their breast milk. The mean maternal age in this study was 32.97 years (standard deviation 4.5 years). The mean age of participants who had cannabis metabolites in their breast milk was higher than mothers who did not report cannabis use (p = 0.01) (Table 1). The majority (87%) of the participants self-identified as non-Hispanic White in both groups. A significantly higher proportion of participants who did not use cannabis had normal BMI (p = 0.04), had a college and postgraduate education (p = 0.001), and had a household income of more than $60,000 (p = 0.001) compared with participants who had cannabis metabolites in breast milk. Use of cigarettes was significantly higher in the cannabis-positive group. The use of alcohol in the two groups was not statistically different. The presence of mood disorder in the groups differed somewhat (p = 0.05), being higher in cannabis exposure than no exposure. There were no statistically significant differences in parity of the participants, mode of delivery, or gestational age at delivery (p > 0.10) (Table 2). The median age of infants was not statistically different between the groups (p = 0.17) nor was the sex of the infant. Majority of participants provided a fully expressed breast milk sample (83.5%) (Table 2). Of the five detected cannabis metabolites in breast milk, THC was predominant (60%) followed by CBD (45%), COOH-THC (41%), CBN (21%), and THC-OH (29%) (Table 3).
Main Characteristics of Mothers and Infants Related to Human Breast Milk Samples in the Study
p Value < 0.01.
BMI, body mass index; SD, standard deviation.
Concentrations of Macronutrients Measured in Human Breast Milk Samples in the Study
p Value < 0.01.
Concentrations of Cannabis Metabolites Measured in Human Breast Milk Samples in the Study
THC, tetrahydrocannabinol; CBD, cannabidiol; OH-THC, hydroxy-delta-9-tetrahydrocannabinol; CBN, cannabinol; COOH-THC tetrahydrocannabinol carboxylic acid.
In unadjusted models, the levels of energy and carbohydrates were not significantly different between the two groups. In comparison, greater protein levels were found in the milk of cannabis exposure compared with no exposure (95% confidence interval [CI], 0.11–0.36, p value = 0.002), and lower log-transformed fat levels were found in the milk of those with detectable cannabis metabolites compared with no exposure (95% CI, −0.201 to −0.007; p value = 0.03) (Table 4).
Unadjusted Association of Cannabis Metabolites with Macronutrients
After adjusting for maternal age, education, income, alcohol consumption, smoking, and mood disorders, the difference in protein and fat levels between the two study groups remained significant. As shown in Table 6, there was a significant association between presence of cannabis metabolites in milk and both protein concentrations and log fat concentrations in the fitted regression model. Milk with metabolites of cannabis had higher mean protein of 0.244 mg/dL (95% CI: 0.112–0.376; p < 0.001) and 0.117 lower log concentration of fats (95% CI: −0.217, −0.018; p = 0.020) compared with control milk (Table 5). This corresponds to a reduction in fats of 11%.
Adjusted Association of Cannabis Metabolites with Macronutrients
Adjusted for maternal age, education, income, smoking, and alcohol use.
Sensitivity Analysis
Multivariable linear regression of cannabis exposure on fat concentration in breast milk stratified for degree of expression of breast milk.
Sensitivity analysis: Adjusting for gender and age of the infant did not change results for carbohydrates, proteins, fats, and calorie density. The results remained unchanged for proteins, carbohydrates, and calorie density when adjusting for degree of expression of breast milk, however, the results for concentration of fats changed with degree of expression of breast milk (95% CI: −0.045, 0.096; p = 0.47). A stratified analysis for degree of expression of breast milk showed that the reduction in fat concentrations in cannabis-exposed breast milk remained significant (95% CI: −0.263, −0.059; p = 0.02) in fully expressed breast milk samples but were insignificant in partially expressed breast milk samples (95% CI: −0.150, 0.160; p = 0.91) (Table 6). The results of the one-way analysis of variance test comparing macronutrient concentrations in the no exposure group, the reported exposure group without metabolites, and the reported exposure group with metabolites showed a significant difference in mean concentration of fat between the reported exposure and reported no exposure (95% CI: −0.296, −0.006), but no difference in mean concentration of fat and other macronutrients among the groups (Table 7).
Sensitivity Analysis
Between-group differences of one-way analysis of variance.
p < 0.05.
BM, breast milk.
Discussion
This study demonstrates higher levels of protein and lower levels of fat in human breast milk associated with the presence of at least one of the five metabolites of cannabis: THC, CBD, THC-OH, THC-COOH, and CBN. The change in fat was noted in fully expressed but not partially expressed breast milk samples. This finding is explained by the fact that fully expressed breast milk includes hind milk, which contains the bulk of fats in breast milk and hence is an effect modifier in this study. This study contributes to the literature by reporting the association of cannabis detected in breast milk with macronutrients in breast milk. Compared with the only other study evaluating the effect of cannabis on human milk macronutrients that had a cross-sectional study design (Josan et al.), this study found a similar positive association of cannabis with protein in breast milk. Those with detectable cannabis in milk were younger than those who did not report cannabis, which was also observed in the Josan et al. study. 23 This study examined five metabolites of cannabis as exposure similar to the Josan et al.’s study. The milk samples examined in the Josan et al. study were at 6–8 weeks postpartum, while the median age of infants in this sample was 6 months. While Josan et al. did not find any significant changes in fat, this study did find a negative association of fat with cannabis exposure during lactation. Also, Josan et al.’s study noted higher lactose levels on exposure to cannabis, whereas this study did not. These differences in results may be related to the difference in age of infants in the two study populations as milk production and composition changes with time from birth. The decrease in fat levels is consistent with the findings of animal studies by Josan et al. and Johnson et al.21,22 Similar to Josan et al.’s animal and human milk studies, no changes in milk energy density were noted in this study. Josan et al.’s study also examined subcomponents of macronutrients and found attenuated levels of secretory IgAs in milk of cannabis exposure compared with nonexposure. This finding underlines the fact that human milk has a multitude of essential micronutrients besides the macronutrients studied in this study and further research is required to examine the effects of cannabis on the composition of human milk to determine the potential indirect effects on the exposure infant.
This study has a reasonable sample size with a 1:2 ratio of exposure to no exposure groups. The exposure group was defined by detectable cannabis metabolites through validated assays as opposed to cannabis use. Given the wide variety of available forms and routes of cannabis in the market, using samples with various cannabis metabolites at detectable levels bypasses the need for pharmacokinetic considerations while measuring the associations of the metabolites with macronutrients. In addition, sensitivity analyses were performed to increase the robustness of the findings.
On the contrary, the no exposure group was defined by the absence of maternal reporting of cannabis use without a confirmatory laboratory assay. Samples from mothers who did not report cannabis use were not tested for metabolites of cannabis due to cost of testing limitations. However, the 12% of milk samples of women who acknowledged cannabis use that did not have any cannabis metabolites were included in the control group and did not show statistically significant difference in macronutrient concentrations from the control group in the sensitivity analysis supporting the findings of the study. Cannabis being an illegal drug at the federal level, reporting bias is expected with underreporting. Underreporting may have decreased since 2016 when decriminalization of recreational cannabis gained momentum across the states. This misclassification bias would bias the result toward null and, if corrected, may amplify the current findings.
Although confounders identified from literature review and DAGs were used, and sensitivity analyses were performed, unknown confounders are possible given the limited scientific evidence to date in this area.
While the presence of any concentration of cannabis is associated with a small but significant change in protein and fat concentrations, the effect of such changes on the growth of the infant is unknown. Prior studies have focused on the effect of changes in macronutrients on the length, weight, and body composition of infants, however, the effect on the development of nervous system, immune system, and gastrointestinal system has not been well studied. Future studies, longitudinal in nature, would be needed to investigate these areas.
Conclusion
This study shows statistically significant alterations in proteins and fat content of human breast milk associated with the presence of metabolites of cannabis. While science has established the benefits of breast milk macronutrients for the infant, research on the effect of any deficiency of one or more of these macronutrients on the growth and development of infants is required to understand and infer any clinical effect that the noted changes in macronutrients in the study may have on the growth and development of infants. Future studies should be directed toward building the body of evidence, dose–effect relationships between cannabis use and macronutrient compositions, as well as any differences in the effect on macronutrient concentrations between the psychoactive and nonpsychoactive metabolites of cannabis. Studies are also required to evaluate the consequences of changes in macronutrient concentrations on the development of immune, gastrointestinal, and nervous systems in infants. Only with the availability of such information can lactating women and health care providers make informed decisions on the use of cannabis during breastfeeding.
Footnotes
Acknowledgment
The authors sincerely express their gratitude to the HMB at the UCSD for providing access to the data for this study.
Authors’ Contributions
P.N.: Research design, data analysis, and article writing. G.B., K.F., and J.W.: Data analysis and article review, and editing. K.B. and C.C.: Article review.
Ethics
This research was approved by the UCSD Institutional Review Board (IRB approval #130658).
Disclosure Statement
The authors have no conflicts of interest to declare for this study.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of any of the funding bodies. In addition, the funders had no role in the study design, data collection and analysis, decision to publish, or preparation or review of the article.
Funding Information
This research was supported by the University of California San Diego (UCSD) Center for Better Beginnings, the National Institutes of Health, grant UL1TR001442, and the Gerber Foundation, project 4998 and project 6488.