
Abstract
Background:
For mothers of infants with congenital anomalies, antenatal milk expression (AME), known as hand expression during late pregnancy, allows mothers to contribute to their newborn’s care through colostrum collection. However, research is limited by self-report of AME adherence and colostrum volume.
Objective:
This study examined the ability of participants to adhere to a recommended protocol on AME for any removal and measurement of colostrum during late pregnancy.
Materials and Methods:
A prospective, longitudinal, observational design was used. Our recommended protocol involved hand expression of 5 minutes per breast for a total of 10 minutes for each AME session twice per 24 hours for any colostrum from 37 0/7 weeks gestation until birth. Women received AME education, completed milk logs, and attempted AME. The study team verified all colostrum volumes.
Results:
Nineteen women (10 nulliparous) participated, with 13 (68%) carrying infants with major organ system defects and 6 (32%) carrying infants with congenital heart defects. Most participants (52.6%) completed more than half but fewer than all AME sessions. Seven participants (36.8%) fully adhered, completing two AME sessions daily until hospital admission. Eighteen participants (94.7%) could remove milk (80–100% of the time). The 24-hour colostrum volume (median 0.35 mL, interquartile range [IQR] 0.065–0.845) and the total colostrum volume (median 3.99 mL, IQR 1.35–6.82) from AME varied.
Conclusions:
Among a small group of women of infants with congenital anomalies, adherence to a recommended protocol is feasible but varied by AME session frequency. Most women could collect colostrum for future infant feeding.
Introduction
Human milk feeding minimizes the risk, incidence, and severity of preventable complications and improves the hospital course of infants with congenital anomalies.1–3 However, intensive care obstacles can hinder mothers’ lactation and breastfeeding goals.4–7 Antenatal milk expression (AME) involves hand expression of the breast beginning at 36 0/7 (i.e., 36 weeks and 0 out of 7 days of pregnancy completed) or 37 0/7 weeks gestation. 8 Growing evidence shows AME as a safe, effective strategy for at risk dyads, enhancing mothers’ breastfeeding self-efficacy 9 and supporting milk supply by colostrum removal.10–11 For infants, AME increases the likelihood of human milk receipt, reducing formula use. 9 Mothers of infants with congenital anomalies may especially benefit as it allows them to contribute to their newborn’s care and provides infants potential immune protection through increased colostrum. 12 Research on adherence to AME guidelines and the colostrum volume collected in this population remains limited.
Feasibility of AME has not been well documented in previous studies; therefore, interpretation of milk supply outcomes is not possible without this information.8,13,14 Past AME studies were retrospective10,15 and cross-sectional16,17 studies involving the electronic health record10,15,16 and self-reported questionnaires prone to recall bias.15,17 Researchers in prospective studies attempted to measure AME adherence using written diaries or log sheets, relying on participant self-monitoring of AME and return of written materials.8,13,14 Some adherence information was lost as 40% of participants did not return their diaries, raising questions concerning adherence. 13 In a randomized controlled trial (RCT), researchers again used diaries but did not fully describe adherence, only noting that 16% of participants completed AME without specifying frequency. 8
The amount of colostrum from AME was similarly measured by participant self-report in written diaries and log sheets.8,13,14 Given AME adherence concerns, is it reasonable to question past studies that did not describe measures to verify colostrum volumes. Demirci et al. found that although 18 participants did AME, only 15 collected colostrum, indicating variability in success despite adherence. 11 To address this gap, mothers of infants with congenital anomalies are an ideal study population as they are primarily pump-dependent and use logs to track milk volume. This setting allows precise measurement of milk supply through AME. Postpartum milk supply outcomes following AME will be reported separately. This study examined the ability of participants to adhere to a recommended protocol on AME for any removal and measurement of colostrum during late pregnancy.
Materials and Methods
Design
Our pilot study used a prospective, longitudinal, observational design from 37 0/7 weeks gestation until participants’ day of birth. The timeline was based on AME initiation research. 18 Ethical approval was obtained via joint agreement from the pediatric hospital and the University of Pennsylvania.
Setting
The study was conducted from June 2022 to May 2023 in the northeast of the United States at a large freestanding children’s hospital with an international referral center for fetal diagnosis and treatment that only delivers infants with congenital anomalies. Families receive a scheduled induction or cesarean date based on their infant’s diagnosis, which is an ideal condition for recruitment and can schedule an optional prenatal lactation consultation, leading to a referral to the study team.
Sample
Eligible women were 18 years or older, English speaking, with a singleton fetus suspected of a congenital anomaly, and anticipated to deliver after 37 0/7 weeks gestation at the study site. They all received a prenatal lactation consultation and verified that they wanted to provide human milk. We confirmed women had a personal smartphone or computer, internet service, and a freezer for participation.
Our exclusion criteria included conditions that prohibit breastfeeding 19 ; abnormal breast tissue such as breast cysts; atypical hyperplasia; breast surgery that can affect the glandular tissue responsible for milk production; assisted reproductive technology or gestational diabetes mellitus as these conditions can lead to hormonal and metabolic changes that may influence milk production, 20 a risk factor for preterm labor or delivery plan at 37 0/7 weeks gestation or earlier; a history of antepartum bleeding, placenta previa, or other serious obstetric or medical issues 18 ; and if women were doing AME by the screening visit.
We distributed a recruitment flyer and ongoingly consulted an advanced practice nurse, maternal fetal medicine physician, and lactation consultant to identify eligible women. Interested women attended a screening visit by 36 0/7 weeks gestation. Enrolled women completed written informed consent and were educated on AME by 36 6/7 weeks gestation. The Diabetes and Antenatal Milk Expressing study, 8 the largest RCT on AME, informed our protocol of hand expression of 5 minutes per breast for a total of 10 minutes for each AME session twice per 24 hours, colostrum collection, syringe labeling, storage, and hospital transport. We instructed on the full protocol verbally and in written form and showed a video (https://www.youtube.com/watch?v=PnG4pW9z4Cc) and breast model demonstration of AME and related procedures. Participants’ understanding of AME was assessed by the study team using the teach-back method on the breast model.
All participants received 1-mL syringes, labels, an ice pack, and cooler and were encouraged to begin AME at 37 0/7 weeks gestation and continue daily until hospital admission. Participants completed a milk log online for each AME session. Virtual check-ins and observation of AME from the study team via Microsoft Teams meetings and every other day texts were provided to support participants. No structured script was used for virtual check-ins; these were participant-driven, allowing them to ask questions and share comments as needed. All colostrum was transported to the hospital and stored in a more than or equal to −20°C freezer. 21
Measures
Demographic characteristics
Participants self-reported via survey their characteristics: age, race and ethnicity, gender, weight, height, education, employment status, income, relationship status, parity, and lactation risk factors including diabetes, body mass index over 30, advanced maternal age, polycystic ovarian syndrome, and thyroid disease.20,22 Participants reported mode of birth and infant characteristics and evaluated their overall AME experience using Likert scale questions via survey on postpartum day 1.
Milk log
The online milk log, accessible to both participants and the study team, tracked adherence to the recommended protocol in real time. The milk log was sent via emailed survey and recorded date and time, AME session completion (yes/no), AME session duration (minutes), colostrum removed from AME (yes/no), and colostrum volume (milliliters). Participants could upload time-stamped photos of any collected colostrum and document feedback from each AME session.
AME adherence
The AME adherence of participants to the recommended protocol was based upon the milk log. Proportions were calculated for AME adherence by AME session frequency of two sessions, a single AME session, or no AME sessions per 24 hours. Full adherence was defined as two AME sessions daily until participants’ hospital admission. Partial adherence was defined as completion of one AME session, while nonadherence was defined as completion of zero AME sessions in a 24-hour period at least once until participants’ hospital admission. The highest and lowest AME adherence by AME session frequency per 24 hours was reported as a proportion range for the sample across late pregnancy.
Colostrum volume
Colostrum volume from AME was measured per 24 hours using 1-mL syringes with precision to 0.01 mL. An investigator verified each self-reported colostrum volume in the milk log by visually comparing it with the actual amount stored in the syringes.
Data analysis
All data were managed using REDCap hosted at the pediatric hospital and analyzed using Stata 18 (StataCorp. 2023. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC). Data were reported as event numbers and proportions, mean ± standard deviation (SD), or median, interquartile range (IQR), and range. Milk log comments were analyzed using simple thematic analysis. 23
We performed individual descriptive analysis and characterized the 24-hour colostrum volume per participant. We conducted descriptive analysis of the sample by hour in 24 hours and per 24 hours for AME adherence, milk removal, and colostrum volume. We differentiated the full adherence, partial adherence, and nonadherence of participants to the recommended protocol. This approach elucidated milk removal or no milk removal from AME and the 24-hour colostrum amounts. Between-group differences were compared using the Mann–Whitney U tests. Significance tests were two-sided with a significance level α < 0.05.
Results
Of 105 eligible women approached with the recruitment flyer, 37 women expressed interest. Of these, nine women were ineligible for not completing a screening visit (n = 3) or presenting with exclusion criteria (n = 6). Twenty-eight women met eligibility criteria (see Fig. 1). Twenty-five women enrolled and 19 women (76%) completed all study activities. Four women withdrew due to delivering before 37 weeks gestation (n = 2) or delivering at an outside hospital (n = 2). Two women lost interest in participating and withdrew after enrollment but before data collection. Demographic characteristics of participants are described in Table 1.
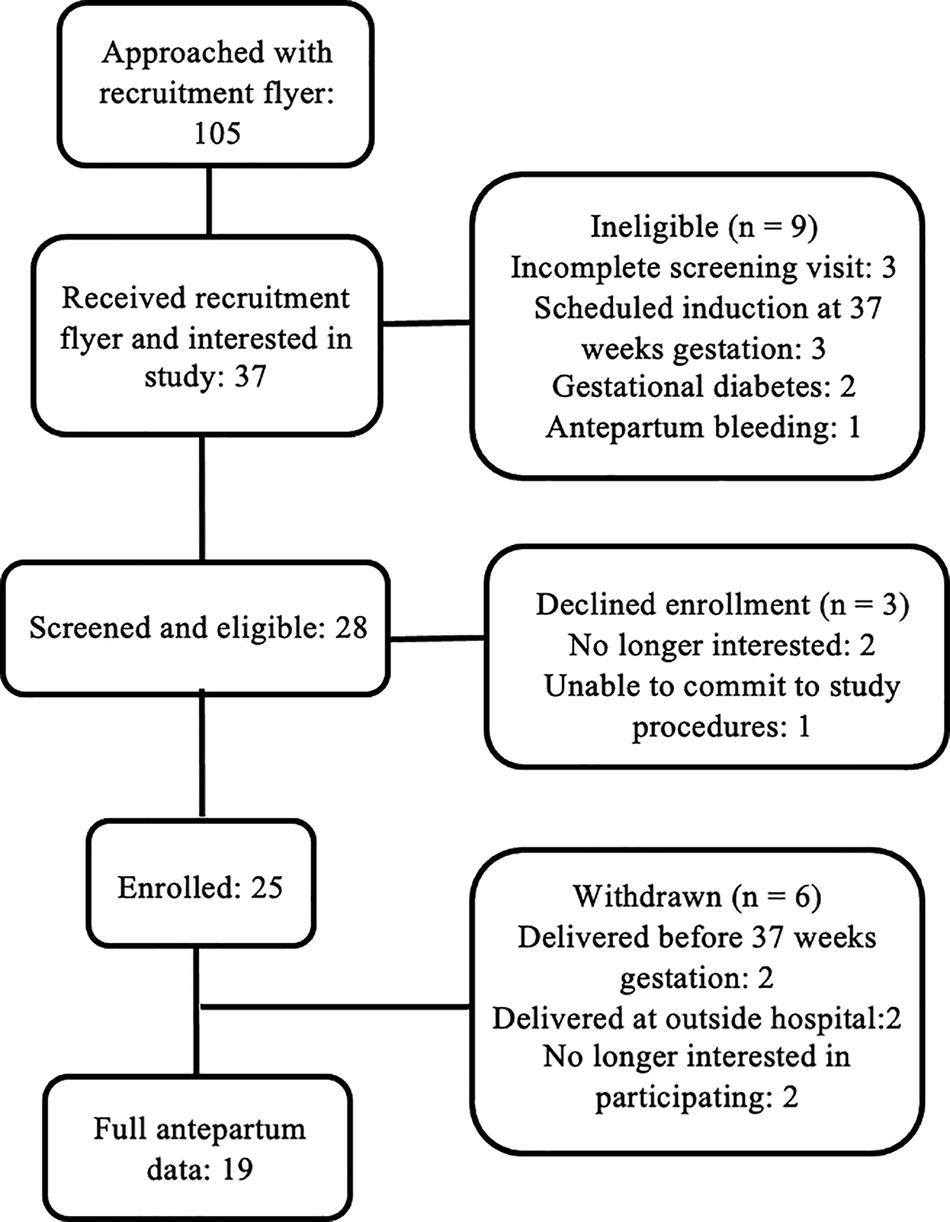
Flowchart of study recruitment and enrollment.
Demographic Characteristics of the Sample and Their Infants (n = 19)
SD, standard deviation.
Characteristics, feedback, and overall experience of AME
AME characterized per hour in a 24-hour period elucidated when participants managed to do AME in a single day. The most frequent self-reported hour (32 out of 191 instances; 16.75%) for the first instance of AME was 11:00–11:59. The hours of 21:00–21:59 and 22:00–22:59 were both the most frequent self-reported hours (37 out of 185 instances; 20%) for the second instance. Table 2 shows the self-reported average colostrum volume from an AME session per hour in a 24-hour period.
Frequency of Self-Reported Milk Removal and Volume of Colostrum from AME by Hour Within a 24-Hour Day (n = 19)
AME, antenatal milk expression; IQR, interquartile range.
Twelve (63.2%) participants shared feedback on AME. Themes and representative comments included Challenges in Collection (6 of 19; 31.6%; “Plunger on syringe popped off and I lost the colostrum.”), Too Little to Measure (5 of 19; 26.3%; “Just drops, not enough to put in a syringe.”), Differences Between Left and Right Breast (4 of 19; 21.1%; “The left breast is producing more than the right breast.”), Time (4 of 19; 21.1%; “Evening collection more fluid than earlier collection.”), and Strategies (4 of 19; 21.1%; “I pulled this extraction after taking a shower. I wonder if the warm water caused the increase.”). All mothers participated in the virtual check-ins. Three participants (15.8%) reported cramping or breast soreness with AME. No serious adverse effects related to AME were reported.
All mothers gave birth at term gestation. On overall AME experience, participants rated that they strongly agree (mean, SD: 87.3 [14.7], 93 [6.3], 91.8 [7.6], 90.5 [11.5], respectively) to each statement: (1) “I believe antenatal milk expression was easy to do”; (2) “I believe antenatal milk expression is useful”; (3) “Overall, I am satisfied with my antenatal milk expression experience”; (4) “Overall, I would consider antenatal milk expression in a future pregnancy.”
Adherence to the recommended protocol
The duration to follow the recommended protocol (median 10 days, range 2–15, IQR 7–15) varied based on participants’ scheduled induction or cesarean date (see Table 3). External factors unrelated to AME including induction date changes, high blood pressure, or amniotic fluid impacted some participants’ AME timeline.
Gestational Period, Duration, and Sessions Completed of Protocol to Practice AME and Colostrum Volume (n = 19)
AME, antenatal milk expression; IQR, interquartile range.
The total number of completed AME sessions (median 16, range 3–30, IQR 10–25) varied across participants. Eighteen (94.7%) of the 19 participants initiated two AME sessions on 37 0/7 weeks gestation. Most participants (10 of 19; 52.6%) completed more than half but fewer than all recommended protocol AME sessions. Seven of the 19 participants (36.8%) fully adhered and did 2 AME sessions daily until their hospital admission. Two participants (G and J; 10.5%) completed <50% of AME sessions.
Adherence to the recommended protocol per 24 hours varied by AME session frequency: two sessions, a single AME session, or no AME sessions. Most participants adhered to two AME sessions per 24 hours from 37 0/7 to 38 6/7 weeks gestation with adherence rate lowest at 66.7% of participants and highest at 100% of participants on separate days within this timeframe. A smaller proportion (5.5–33.3% of participants on two separate days) partially adhered and completed one AME session per 24 hours from 37 1/7 to 38 5/7 weeks gestation. Completion of zero AME sessions, that is, nonadherence, per 24 hours occurred for a very small proportion (5.3–16.7% of participants on two separate days) from 37 0/7 to 38 0/7 weeks gestation. All participants enrolled beyond 38 0/7 weeks gestation completed AME at least once or twice from 38 1/7 to 39 0/7 weeks gestation.
Almost all participants (93.3–100%) adhered to the recommended protocol duration of 5 minutes per breast for a total of 10 minutes for each AME session. Three (15.8%) participants self-reported completing AME for a duration of 7–15 minutes.
Milk removal and colostrum volume from AME
Eighteen of 19 (94.7%) participants removed milk during their full length of time to follow the recommended protocol on AME. However, seven of 19 (36.8%) participants experienced at least one instance when they could not remove milk from an AME session. Six (85.7%) of seven participants who fully adhered to the recommended protocol of two AME sessions daily removed milk each time. Participant H, a multiparous mother without any health conditions, fully adhered to the recommended protocol but could not remove any colostrum. The 24-hour colostrum volume (median 0.35 mL, IQR 0.065–0.845) and the total colostrum volume (median 3.99 mL, IQR 1.35–6.82) were highly variable. Of note, participant L and participant M, nulliparous mothers without any health conditions, attained a higher 24-hour colostrum volume (median 1.75 mL, IQR 0.33–4; median 1.7 mL, IQR 1.25–2.42, respectively) and total colostrum volume (27.48 mL; 31.48 mL, respectively) than the sample average from 37 0/7 to 38 5/7 weeks gestation. Figure 2 shows the participants’ 24-hour colostrum volume from 37 0/7 weeks gestation until their day of birth.
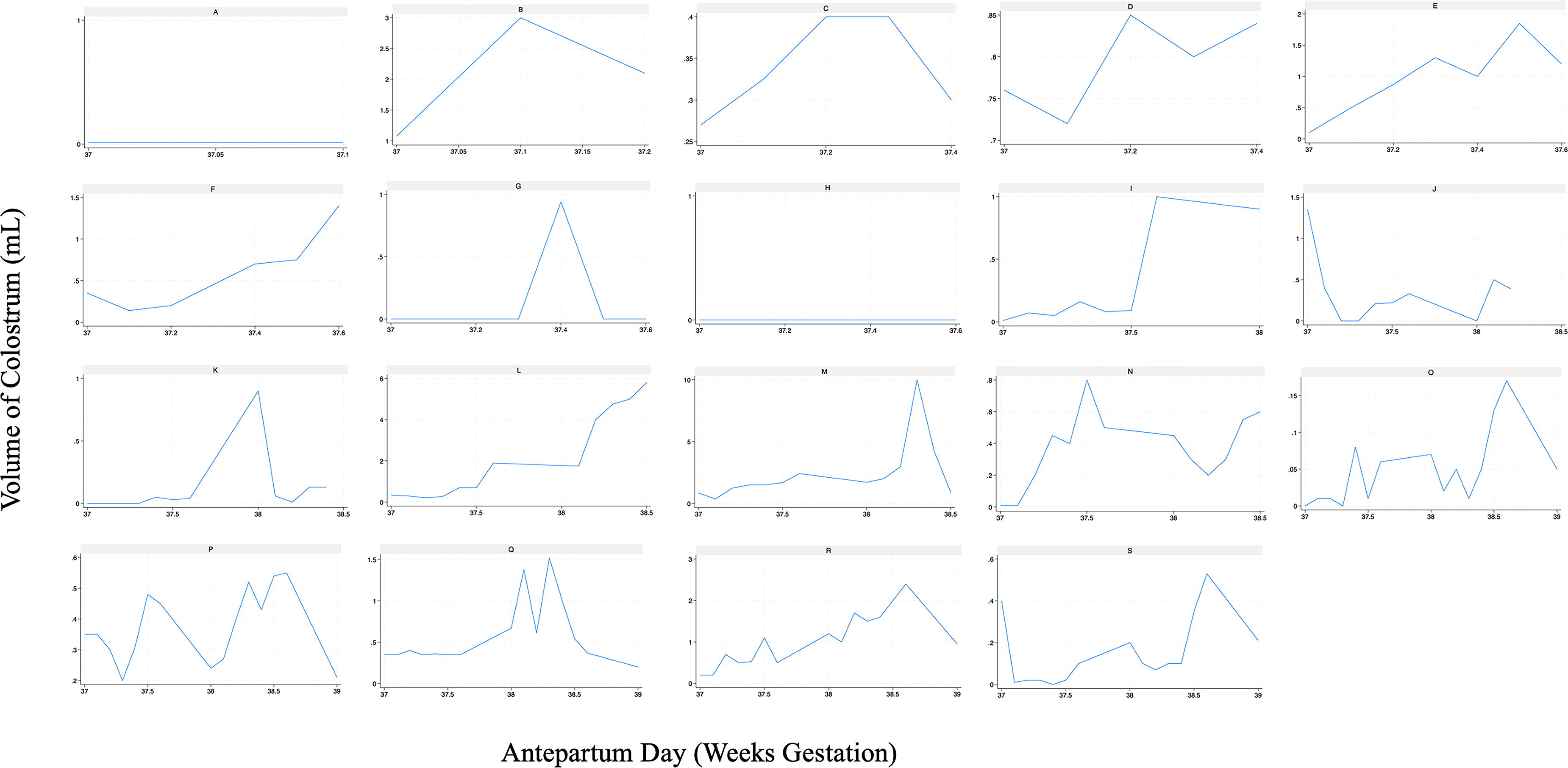
Twenty-four-hour volume of colostrum from antenatal milk expression (AME) during late third trimester of pregnancy (n = 19). Scales differ for each x- and y-axis.
The colostrum was removed and the volume obtained for those who did two AME sessions versus a single AME session varied (see Table 4). Of participants who did AME, most participants (80–100%) removed milk compared with no milk removal from 37 0/7 to 37 6/7 weeks gestation. A very small proportion (11.1–20%) of participants could not remove milk from 37 0/7 to 37 6/7 weeks gestation.
Milk Removal and Volume of Colostrum from AME by Adherence to the Recommended Protocol per Gestational Day
This table represents pregnant women (n = 19) who followed the recommended protocol for different lengths of time—range: 2 days antepartum (37 0/7–37 1/7 weeks gestation) to 15 days antepartum (37 0/7–39 0/7 weeks gestation). Event numbers and proportions calculated for any milk secretion by frequency of adherence to the recommended protocol are based on the number of participants who practiced AME on the specified antepartum day. An incremental decrease in the columns of “number of participants enrolled in study” and “the number of participants who practiced AME” signified a participant’s completion of study activities since the time to follow the recommended protocol has ended (i.e., a participant’s hospital admission for birth).
AME, antenatal milk expression; IQR, interquartile range.
Nulliparous mothers demonstrated a significantly higher 24-hour colostrum volume (median 0.52 mL, IQR 0.27–1.2 versus median 0.07 mL, IQR 0.01–0.39; p < 0.001) and total colostrum volume (median 6.21 mL, IQR 3.99–16.08 versus median 1.7 mL, IQR 0.72–3.4; p = 0.01) compared with multiparous mothers. One participant, a nulliparous mother without any health conditions, who did one AME session removed a colostrum volume of 5.8 mL compared with six participants (a group involving two nulliparous and four multiparous mothers and are all without health conditions) who did two AME sessions and attained a volume range of 0.13–2 mL at 38 5/7 weeks gestation.
Discussion
Our study found relatively good adherence to AME; however, measured colostrum volumes were much lower than those described in the literature. We used an online milk log for real-time monitoring, 1-mL syringes measuring up to 0.01 mL, time-stamped photos, and investigator verification of colostrum volumes at hospital admission. These methods were absent in prior studies as researchers relied on participant self-report in written diaries and log sheets.8,13,14 Our 24-hour colostrum volume (median 0.35 mL, range 0–10, IQR 0.065–0.845) was lower than reported per AME episode in pregnant women with diabetes (median 1.67 mL, range 0.21–14.1). 13 Similarly, our total colostrum volume (median 3.99 mL, range 0–31.48, IQR 1.35–6.82) was lower than the totals (median 39.6 mL, range 5–310; median 5.5 mL, range 0–905, IQR 0–22; median 88.5 mL, range 2.8–322) collected among pregnant women with diabetes in a pilot study, 13 an RCT, 8 and an unpublished thesis/dissertation, 14 respectively. Our volume likewise was lower than the total colostrum volume (median 5.8 mL, range 0–93.3, IQR 45.2) collected among nulliparous pregnant people in an RCT. 24 Despite our small sample size, the study’s strength lies in the triangulation of methods. Our meticulous collection and verification processes enhance measurement accuracy compared with past research and may reflect a better measurement of the natural variation in colostrum yield during late pregnancy.
Our research builds on a case series on AME in parents of infants with congenital heart defects. 25 Participants had a positive overall AME experience, similar to feedback of healthy women11,26 and those with diabetes during pregnancy.8,13,27 The high rating of “I believe antenatal milk expression is useful” suggests participants’ self-motivation despite milk removal inconsistencies. Since the health benefits of human milk are dose-dependent and colostrum boosts infant immunity, any amount collected from AME is clinically significant.
Adherence was more manageable with AME performed late morning and evening, offering insight beyond the “two AME sessions daily” guideline. This evidence may help develop more specific clinical guidelines for AME and demonstrates that AME remains feasible even with multiple health care appointments. 28 We lack data on why mothers did not consistently do AME twice daily. Other studies suggested time involvement,10,12,29 minimal milk removal,11–12 or stress related to the infant’s condition or care7,30 as factors. The focus on the infant’s health may have overshadowed mothers’ commitment to AME, affecting adherence. Our study team’s support and virtual check-ins were valuable 29 and provided opportunities to reach out but likely positively influenced participants’ fidelity to AME.
An RCT of nulliparous pregnant people found slight weekly increases in median colostrum volume (37 weeks: 0.24 mL; 38 weeks: 0.22 mL; 39 weeks: 0.29 mL; 40 weeks: 0.88 mL). 24 In contrast, we observed no clear pattern on colostrum volume per 24 hours until birth. Our results also suggest individual characteristics including anatomy, age, and parity playing a role.20,31 Notably, nulliparous mothers had higher colostrum volumes than multiparous mothers, suggesting hormonal differences affecting mammary glandular tissue development and milk secretion. 32
Our protocol recommended hand expression, as most AME studies use this method. 33 A recent RCT investigated electrical breast pump use during pregnancy, finding 66 participants (40%) adhered to the protocol of pumping 20 minutes three times daily from 37 weeks gestation. 34 However, 25 participants (38%) could not remove any colostrum or removed immeasurable drops. 34 Pumping was also associated with increased labor induction (odds ratio 2.09, 95% confidence interval 1.05–4.14). 34 Suction from pumping, unlike hand expression involving only compression, promotes oxytocin and can induce spontaneous labor when sustained for ≥1 hour. 35
During pregnancy, lactogenic hormones of estrogen, progesterone, prolactin, and other metabolic hormones regulate lactation by endocrine control. 36 Placental regulation of progesterone inhibits optimal prolactin activity, explaining increased milk secretion after birth. Saint et al.’s colostrum estimation (mean 37.1 g, range 7–122.5) in the first 24 hours after birth was larger than our values. 37 This suggests that endocrine control of lactation during pregnancy limits colostrum secretion, making colostrum removal by AME challenging and dependent on anatomical factors such as ductal size (to store colostrum) and nipple anatomy. Our use of hand expression, rather than vacuum, may have further limited colostrum volume.
We encountered challenges, including nonstandardized prenatal lactation consultations, affecting recruitment. Factors such as changes in induction dates, unplanned pregnancy events, busy schedules, and study time commitment contributed to the relatively low enrollment, withdrawal, or participants’ available time for AME. One participant had COVID-19 after enrollment but remained willing and able to do AME.
We disclose limitations. We did not provide counseling on AME discontinuation, though no serious adverse effects were reported. Colostrum volume per AME session could not be verified due to the use of the same syringe for both AME sessions in the same day. The hospital’s extensive lactation policies, combined with our observational design, sampling technique, sample size, and institutional culture limit generalizability. Additionally, the hospital’s partnership with supportive facilities (i.e., housing program and resources) affects our findings’ applicability to low resource settings. Our sample size is comparable to similar AME studies in the urban northeast of the United States (n = 29; n = 22 in AME arm of RCT, respectively).24,26
Automated data collection reduced participant burden. We validated self-reported data with time-stamped photos and verified colostrum volume, addressing reliability concerns from past research.8,13,14 Results may seem like attrition, but our sample represents a full dataset, and no dropouts occurred during data collection.
We used terms including women and mothers because 89.5% of participants identified as cisgender women. Two participants skipped the gender identity question, hinting at gender diversity but limiting use of inclusive language without knowing their preferred terminology. Future researchers should recognize the complexity of infant feeding and use language that reflects the diversity of lactating parents.
Our findings require replication with adequately powered samples to clarify the true relationship between AME adherence and colostrum removal. Such research would reveal realistic expectations of colostrum removed during pregnancy with the placenta intact, known to inhibit milk secretion, and may help mitigate negative feelings if women experienced difficulties.12,17,29,38 Future investigations should explore the mechanics of AME and individual factors.
Conclusion
A small group of women with infants having congenital anomalies did AME to potentially bank colostrum. Adherence to a recommended protocol is feasible but varied by AME session frequency. Milk removal is more likely than no milk removal from AME, although volumes are small and variable, but every colostrum drop is valuable for infant development. Time represents a major component to AME as adherence was highest in the late morning and evening and AME frequency, and number of days to follow a recommended protocol, can influence the colostrum volume removed. For mothers of infants with congenital anomalies, AME, while being effort- and time-intensive, proves useful by frequent practice of milk expression skills.
Footnotes
Acknowledgments
The authors acknowledge Julie Moldenhauer, Shawnese Duren, and Rachelle Lessen for their assistance with study recruitment and the administrative and regulatory support of Elizabeth Froh, Lonaya Baker, Susan Spinner, Sabrina Flohr, Darcy Brodecki, Michele Diorsio, and Joseph Lim. They thank Holly Harner and Rebecca Clark for their insightful feedback in the development of the article as well as Subhash Aryal and Joseph Rhodes for their statistical and REDCap support.
Authors’ Contributions
N.A.J., D.T.G., E.T.L., and D.L.S. contributed to the conceptualization and methodology of this work. N.A.J contributed to the formal conduct and analysis of this work. D.L.S. contributed supervision to this work. All authors substantially contributed to drafting or revising the article. All authors approved the final version of this article and take responsibility for its content.
Disclosure Statement
N.A.J. was the 2023 recipient of the Margaret Comerford Freda Graduate Nursing Scholarship and received funding from the March of Dimes and Pampers. D.T.G. received salary from an unrestricted research grant from Medela AG administered by the University of Western Australia. E.T.L. and D.L.S. have no relevant financial or nonfinancial conflicts of interests to report.
Funding Information
The authors acknowledge the following organizations who have generously funded this study: the