
Abstract
Objective:
Wound healing is a complex and dynamic process essential for restoring tissue integrity and homeostasis. It is thought that breast milk contributes positively to the wound healing process, thanks to the components it contains. The aim of this study is to compare the effects of breast milk on the wound healing process at different lactation stages and to evaluate the underlying mechanism(s).
Materials and Methods:
The effects of breast milk from different lactation stages (colostrum, transitional, and mature milk) on wound healing were determined by in vitro scratch assay in L929 fibroblast cells. 2,2-Diphenyl-1-picrylhydrazyl (DPPH), total oxidant, and antioxidant capacity were used to confirm antioxidant effects. The effect of breast milk on netrin-1 levels in L929 cells was elucidated by ELISA.
Results:
Breast milk at different lactation stages promoted wound healing. While the wound closure percentage was determined as 48.7% in the control group, this rate was determined to be the highest at 81.6% in the mature milk group (p:0.0002). The free radical scavenging capacity of colostrum, transitional, and mature milk with DPPH was determined as 49.69%, 60.64%, and 80.85%, respectively, depending on the lactation stages. Netrin-1 levels detected by ELISA were determined as 490.1 ± 6.5 pg/mL in the control group, while the lowest level was determined as 376.6 ± 4.5 pg/mL in mature milk (p:0.0003).
Conclusions:
Breast milk, especially mature milk, promoted wound healing on L929 cells by suppressing netrin-1 levels and scavenging free radicals.
Introduction
Wound healing is a complex and dynamic process essential for restoring tissue integrity and homeostasis. It involves a series of intricate cellular and molecular events culminating in the repair of damaged tissue and the reestablishment of its normal structure and function. 1 The process can be broadly categorized into four overlapping phases: Hemostasis, inflammation, proliferation, and remodeling, each characterized by distinct cellular activities and molecular signaling pathways. 2 This process is composed of reepithelialization, fibroblast repopulation, and extracellular matrix (ECM) remodeling. Fibroblasts play a key role in reepithelialization in the wound healing process. Along with re-epitelisation, restoration of the dermis occurs through migration and proliferation of fibroblasts. Multiple cell types in the dermis layer function to activate fibroblast proliferation and migration necessary to repair the dermis. For example, recent studies have shown that intradermal adipocytes play an important role in fibroblast activation and migration. The response of fibroblasts during wound healing determines the outcome of tissue repair. In response to injury, fibroblasts release growth factors that trigger fibroblast migration and proliferation. They also secrete inflammatory cytokines to trigger the immune response to protect against external pathogens in the wound. These fibroblasts also produce other extracellular matrix proteins to aid wound repair. 3 Fibroblasts are the most abundant cells in skin tissue. Various in vitro and animal models are available to screen for the wound healing nature. Among these, the fibroblast cell-based scratch assay is an inexpensive and well-established model that supports the initial understanding of the wound healing efficacy of new therapeutic agents.4–6
Breast milk, often referred to as “liquid gold,” is the natural source of nutrition for infants and is known to contain a diverse array of bioactive components, including growth factors, cytokines, hormones, and immune cells. 7 Depending on the period and secretion composition, breast milk can be classified as follows: 1- Colostrum: Secreted in the first 5 days after birth, 2- transitional milk: Secreted between days 5–15 after birth following colostrum and 3- mature milk: Secreted after the fifteenth day postpartum. 8 Beyond its nutritional value, breast milk has been recognized for its potential therapeutic properties, including antimicrobial, anti-inflammatory, and immunomodulatory effects. 9 These properties suggest that breast milk may play a beneficial role in wound healing.
Several studies have investigated the effects of breast milk on wound healing, both in vivo and in vitro. For example, research by Fernández et al. (2013) demonstrated that breast milk exhibits antimicrobial activity against a wide range of pathogens, suggesting its potential utility in preventing wound infections. 10 In addition, studies have shown that breast milk contains various growth factors, such as epidermal growth factor (EGF) and transforming growth factor-beta (TGF-β), which have been implicated in promoting tissue repair and regeneration. 9
Despite the growing body of evidence supporting the potential wound healing properties of breast milk, the underlying mechanisms remain poorly understood. Furthermore, most studies have focused on the effects of breast milk on cutaneous wound healing. Utilizing an in vitro model can isolate and control various factors that may influence wound healing, allowing a more detailed examination of the specific effects of breast milk on the process. In addition, by gaining a better understanding of the underlying mechanisms, this may be able to develop novel therapeutic strategies utilizing breast milk or its components to enhance wound healing in clinical settings.
Investigating the effective factors in wound healing is important for developing medical interventions and accelerating the healing process. In recent years, the potential effects of netrin-1 on wound healing have received increasing attention. Netrin-1 has been identified as an axonal guidance molecule primarily involved in neuronal guidance and cellular migration processes. 11 However, recent studies suggest that netrin-1 may also play an important role in tissue healing and regeneration.12–14 How netrin-1 contributes to wound healing processes such as cell migration, proliferation, angiogenesis, and anti-inflammatory responses is still not fully understood.
The main aim of this study is to compare the effects of samples from different periods of breast milk on wound healing in an in vitro wound model and to understand the mechanisms behind these effects. At the same time, determining the antioxidant activity levels of breast milk and evaluating its effect on netrin-1 levels in L929 cells are important to understand the contribution of this molecule, which plays a potential role in wound healing. By elucidating the effects of different periods of breastfeeding on wound healing, this study may shed light on future clinical applications and contribute to the development of new treatment strategies to accelerate wound healing.
Materials and Methods
Sample collection
Milk samples were taken from the mothers included in the study (n = 3) on the 5th (colostrum), 10th (transitional milk), and 20th day (mature milk) of lactation, before breastfeeding, from one breast, with the help of a vacuum milk pump collected into sterile milk bags. The breast milk was not subjected to any pasteurization process. Samples at +4°C were used in the analysis to determine the total oxidation/antioxidant status of the breast milk. The samples taken were stored at −20°C to be used in further analyses.
The breast milk collection protocol was approved by Burdur Mehmet Akif Ersoy University Ethics Committee (Approval No.2022/05). Before donating fresh milk, the breastfeeding mother was informed and consent forms were obtained.
Preparation of samples
Before the study, the collected samples were placed in plastic tubes and centrifuged at 5,000 rpm for 5 minutes. The surface layer was passed with a thin pipette tip and the supernatant was taken into a clean tube. It was centrifuged at 10,000 rpm for 5 minutes to remove cells and cell debris. These samples containing soluble proteins were used for all analyses. It was then filtered through a 0.22 syringe filter and stored at −20°C until analysis.
DPPH assay
The antioxidant activity of breast milk was determined by the 2,2-diphenyl-1-picrylhydrazyl (DPPH) free radical scavenging method. Breast milk samples were mixed with 0.1 mM DPPH (abcr GmbH, Germany, Cas# 1898-66-4) solution prepared with methanol at a ratio of 1:1 without dilution. The mixtures were incubated for 30 minutes in the dark. Then, absorbance values at 517 nm wavelength were measured using a UV–Vis spectrophotometer (T60 UV-PG Instruments). Methanol was used as a blank. In the negative control, methanol was used instead of the sample and mixed with DPPH solution at a ratio of 1:1. The antioxidant activity of the samples was calculated with the following formula:
Total oxidant/antioxidant capacity assay
Total oxidant/antioxidant capacity (TOC/TAC) and oxidative stress indexing (OSI) parameters were studied to reveal the oxidant and antioxidant status of human breast milk during different periods of lactation. The principle of the method used to determine TOC is that the oxidants in the sample oxidize the iron ion chelating complex. Ferric ion forms a chromogenic colored complex in an acidic medium. The intensity of the color is directly proportional to the amount of oxidant in the sample and the total amount of oxidation is determined by spectrophotometric measurement at 530 nm. This analysis is calibrated with hydrogen peroxide (H2O2) and the results are expressed as H2O2 equivalents (μmol H2O2 Equiv/L). 15
The TAC principle is a colorometric method measured spectrophotometrically, working on the basis of 2,2’-azino-bis(3 ethylbenzothiazoline6-sulfonic acid) (ABTS). To determine the total antioxidant capacity, the antioxidants in the sample cause the reduction of ABTS radicals in the procedure, resulting in the disappearance of the dark blue-green color of ABTS. The total antioxidant amount is determined by spectrophotometric measurement at 660 nm. This analysis is calibrated with Trolox (Vit E analog), a stable antioxidant solution, and expressed as Trolox equivalent (mmol Trolox Equiv/L).
16
The protein content of milk samples was determined spectrophotometrically by measurements at 595 nm according to the Bradford (Coomassie Brilliant Blue) method.
17
The percent ratio of TOC level to TAC level was regarded as the OSI. The OSI value was calculated with the following formula:
In vitro wound healing assay
The scratch assay was used as a model for evaluating breast milk for wound healing potential. For in vitro wound healing testing, the L929 fibroblast cell line was used. L929 cells were procured from American Type Tissue Culture. L929 cells were then cultured in a controlled laboratory environment using Dulbecco’s Modified Eagle Medium (DMEM) (Biowest, France) enriched with 10% fetal bovine serum (Biowest, France) and 1% penicillin-streptomycin (Biowest, France). The incubation was carried out at 37°C and a carbon dioxide level of 5%. The cells were grown in the medium for 2–3 days until they reached 80–90% confluency, at which point the medium was changed. When the cells reached a sufficient amount, they were washed with Phosphate Buffer Saline (PBS) and trypsinized by adding Trypsin-EDTA (ethylenediaminetetraacetic acid) (0.25%) (Biowest, France). Cells were collected from the culture dish and transferred into 6-well cell culture dishes at a density of 5 × 105 cells/well and incubated for 24 hours. Cells were grown into monolayer in a 6-well cell culture dish and then the cell layer was scratched using a sterile pipette tip to create a wound. The cells were washed with PBS to remove debris, and the cells were then treated with fresh DMEM containing 25% breast milk. The control group was treated with DMEM medium only. After the wound was created, the wound healing process was monitored for 6 and 12 hours. At specific time intervals, cell migration and cell proliferation in the wound area were analyzed by imaging under an inverted light microscope (Olympus CK40) and using the ImageJ program. The percentage of wound closure was calculated using the following formula:
Detection of netrin-1 levels
Human netrin-1 levels were assessed in duplicate using a specific ELISA kit (Catalog #E1277Hu, Bioassay Technology Laboratory, Shanghai, China) following the manufacturer’s guidelines. Breast milk samples were thawed on ice, and were sterilized using a 0.2 µm filter. These samples were treated for 72 hours with 25% in culture media of the cells cultured the day before in 6-well plates (1x105 cells/well). At the end of the period, the supernatants were centrifuged, aliquoted, and stored at −80°C until used for the ELISA experiments. The minimum detectable level of human Netrin-1 was 10 pg/mL. Briefly, the supplied standard stock solution was diluted in 1:2 to create the standard curve. Then, each sample was added into wells, mixed with netrin-1 antibody in duplicate, and for reaction, the HRP-Streptavidin solution was infused into these wells. After incubation at 37°C for 60 minutes, each well was washed five times. After washing, the substrate A and the substrate B were added, and incubated at 37°C for 10 minutes in the dark. Then, HRP reaction was interrupted by adding stop solution. The optical density values were measured with MultiscanGO spectrophotometer (Thermo Fisher Sci, Massachusetts, USA) at 450 nm. The netrin-1 (pg/mL) quantification of each sample was performed by four parameter logistic (4PL) curve of the standards.
Statistical analysis
All experiments in this study were conducted independently. Graphs showed the average of the data obtained from these experiments along with calculated standard deviations. The graphs were drawn using GraphPad Prism 8 software, and all results were statistically analyzed using GraphPad Prism 8 and SPSS software. Student’s test was used to compare differences and significance was considered at p ≤ 0.05. The data were analyzed for intergroup comparison in TAC, TOC, and OSI using one-way variance analysis (One-Way ANOVA) and Tukey’s Post-test. All experiments were performed at least three times.
Results and Discussion
Breast milk is the primary source of nutrition for the healthy development of the baby and has various positive effects on health with the bioactive components it contains. In this study, the antioxidant activity of breast milk at different stages was evaluated using the DPPH method (Fig. 1). First, the inhibition rate against DPPH in the colostrum sample was determined as 49.69%. This demonstrates the existence and importance of the antioxidant capacity of colostrum. Colostrum has a particularly rich ingredient profile to strengthen the baby’s immune system and protect against infections in the postnatal period. Transitional milk sample showed a significant increase in antioxidant activity than colostrum. The inhibition rate against DPPH was measured as 60.64%. This shows that the antioxidant capacity of milk increases during the maturation process and has more protective potential for the baby. Finally, the mature milk sample had the highest antioxidant activity. The inhibition rate against DPPH was recorded as 80.85%. In the DPPH test for radical scavenging activity, the mature milks were more potent (80.85%) to reduce the stable radical DPPH in comparison with colostrum and transitional milks. This suggests that the antioxidant capacity of breast milk increases as it matures, becoming an important source to support the health of the baby. Also, statistical comparison was made by analysis of variance with repeated measures in cases with complete sampling (n = 3).

DPPH radical scavenging activity of breast milk in different lactation stages. 2,2-DPPH, diphenyl-1-picrylhydrazyl.
In the study conducted by Zarban et al. (2009) on milk samples (colostrum, transitional, and mature milk) collected at different times of lactation from 115 healthy women with full term, total antioxidant capacity was determined by FRAP (Ferric Reducing Antioxidant Power Assay) test and radical scavenging activity was determined by DPPH test. In the sixth month of the study, total antioxidant levels in colostrum decreased from 1061.6 ± 500.6 μmol/L to 724.7 ± 302.4 μmol/L. DPPH test results showed that the radical scavenging activity of colostrum had a higher potential (50 ± 20%) in reducing stable radical DPPH compared to transitional (40 ± 20% and 41.9 ± 19%) and mature milk (44 ± 19% and 38.2 ± 17%). Zarban et al. reported a trend toward decreased antioxidant activity levels by DPPH assay as lactation progressed to later stages. 18 Sanchez-Hernandez et al. (2021) determined antioxidant activity using DPPH and ABTS tests on milk taken from 18 mothers included in the study at different stages of lactation. According to the DPPH results, mean values were determined as 150.4 µmol TE/L, 148.6 µmol TE/L, and 156.4 µmol TE/L, median values were 161.5 µmol TE/L, 137.3 µmol TE/L, and 157.2 µmol TE/L for colostrum, transitional, and mature milk, respectively, and no statistically significant difference was determined between lactation stages. 19 When the samples included in the studies are evaluated, it is thought that these differences may be caused by conditions such as the number of samples, 15 the average day on which the samples were taken, 14 storage conditions,20–22 and premature or full-term birth.23,24 Previous studies have reported that milk content is also affected by factors such as diet 25 and maternal age. 26
In the study, TOC, TAC, and OSI, which are biomarkers of oxidative status parameters, were studied to reveal the oxidant and antioxidant activity of breast milk in different periods of the breastfeeding period. TAC was highest in colostrum and significantly decreased through the course of lactation with lowest levels measured in mature milk (p < 0.001). The lowest values of TOC were observed in transitional milk compared to breast milk. TOC was significantly higher in mature milk compared with colostrum and transitional milk (p < 0.001, both). The lowest values of OSI were observed in colostrum and significantly increased through the course of lactation. OSI of mature milk was significantly higher than other breast milk (p < 0.001) (Table 1). In the study where the total antioxidant capacities of colostrum, transitional, and mature milk samples were evaluated, it was similarly highest in both preterm and full-term groups, and gradually decreased in other samples. In addition, it has been determined that CoQ10, α- and γ-tocopherol concentrations in human milk are directly related to the antioxidant capacity of milk. 27 In the study by Deniz et al. (2021), where they evaluated the antioxidant/oxidant status of preterm and term milk samples in different periods of lactation, TAC level was found to be highest and OSI value was found to be lowest in both preterm and term colostrum samples. In the foremilk and hindmilk total oxidation/antioxidant status analyses of preterm/term transitional and mature milk samples, it was observed that the TAC value of term transitional milk was found to be significantly higher. 24 Similarly, Silva et al. (2024) found the antioxidant profile of colostrum to be higher than that observed in the later stages of milk, indicating that pro-oxidants increase in the later stages. The study highlights the vital role of a balanced maternal nutrition in shaping the pro-oxidant status of breast milk, along with its effects on baby health. 28 In another study, it was found that the malondialdehyde level in colostrum was lower and the antioxidant enzymes Superoxide dismutase and Catalase activities were higher in preterm groups than in term groups. 29 In a different study, it was reported that as the lactation period progresses, malondialdehyde levels increase, and nitric oxide and lactoferrin levels and catalase and superoxide dismutase activities decrease. The results of the study highlight the importance of breastfeeding immediately after birth to benefit from the antioxidant advantages of colostrum. 30 We concluded that the oxidant–antioxidant balance in breast milk gradually decreases in terms of antioxidant capacity in the later stages of lactation. Previous studies comparing the antioxidant properties of breast milk at different stages of the breastfeeding process have reported heterogeneous results. Many variables related to the methodology, as well as the number and characteristics of the samples in the studies, may cause this diversity. In various studies investigating the effect of storage conditions on the antioxidant capacity of milk, it was observed that fresh milk had higher antioxidant power, and milk at +4°C for 24 and 72 hours had a higher antioxidant capacity than frozen milk.31,32 Studies point out that nutrients in the diet of breastfeeding women may affect the macronutrient composition of breast milk and will be associated with oxidant–antioxidant factors.33,34
Total Antioxidant Capacity, Total Oxidant Capacity, and Oxidative Stress Index Values of Breast Milk at Different Stages
OSI: oxidative stress index (Arbitrary Unit; AU); TAC: total antioxidant capacity (µmol Trolox Eq/L); TOC: total oxidant capacity (µmol H2O2/L).
Values are presented as mean ± standard deviation. The limit of significance was accepted as p < 0.016. ▲: p < 0.001.
The potential effect of different stages of breast milk on in vitro wound healing was evaluated using the scratch test method. According to the scratch test results performed on L929 fibroblast cells, the wound closure percentage at 6 hours in the control group was determined as 48.7% (44–50%). However, this rate was found to be 56.4% (53–58%) in cells treated with colostrum, 70.4% (68–73%) in cells treated with transitional milk, and 81.6% (79–84%) in cells treated with mature milk (Fig. 2). These results suggest that different stages of breast milk have the potential to promote wound healing at the cellular level.
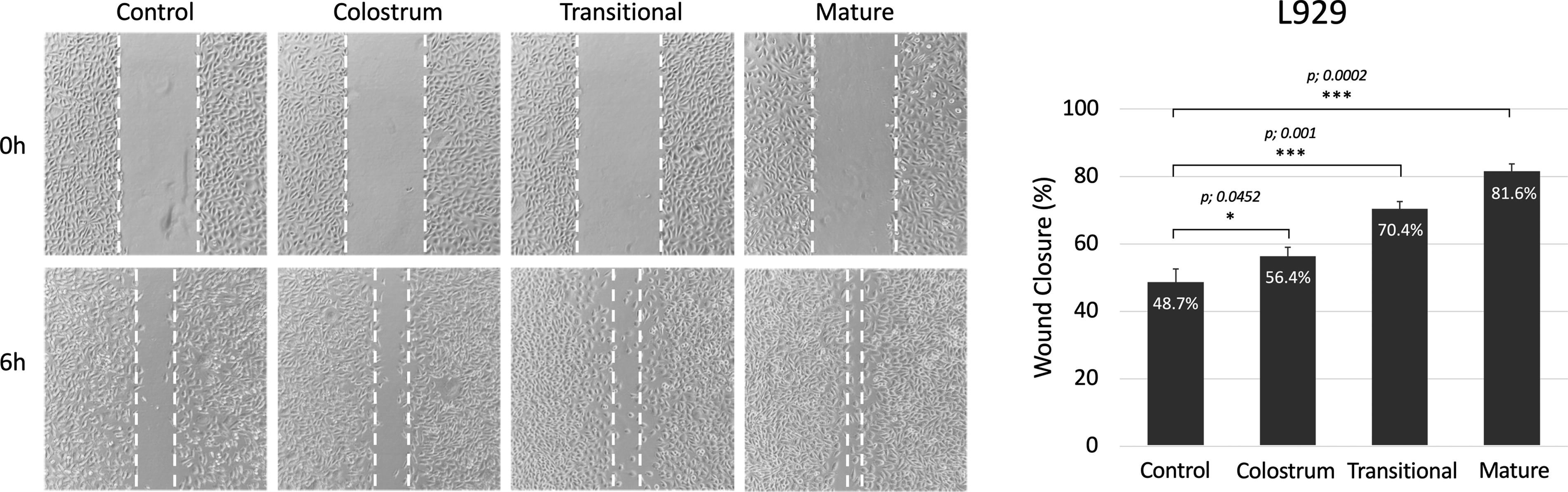
Images of scratch assay of L929 fibroblast cells and percentage wound closure graph of L929 fibroblast cells. Results are expressed as mean ± SEM (Standart Error of the Mean) (*p < 0.05 versus control; **p < 0.01 versus control; ***p < 0.001 versus control).
It has been reported in previous studies that the composition of breast milk varies with lactation stages and that colostrum, transitional milk, and mature milk exhibit different compositions of bioactive components. Colostrum is known for high concentrations of immunoglobulins, growth factors, and antimicrobial substances, which are crucial for providing passive immunity to newborns. Transitional milk contains higher levels of lactoferrin, lysozyme, and cytokines, which have antimicrobial and anti-inflammatory properties. Mature milk, on the other hand, is characterized by a stable composition that meets the nutritional needs of the growing baby. 35 It has bactericidal properties due to the presence of lactoperoxidase, lactoferrin, immunoglobulin A, and lysozyme. It also contains complimentary molecules, including fibronectin, interleukin 6, EGF, TNF-α, and compounds, which aid in the healing of epithelial and stromal wounds like TGF-β, IGF-1, lipids, and vitamins. These substances improve the phagocytosis of pathogens and cell migration in damaged tissues.36–38
Several studies have investigated the effects of breast milk on wound healing. In their study on 24 female experimental corneal epithelial defect mouse models, Asena et al. (2017) found that topical human breast milk drops led to faster and better healing of central corneal epithelial defects compared to serum drops, artificial tears, and the control group (p < 0.001). Breast milk (mature milk) was obtained from a breastfeeding mother with a 6-month-old term baby. 36 Kasrae et al. (2015) administered breast milk to 116 babies with atopic eczema and compared its efficacy to 1% hydrocortisone. The study showed that on day 21, the frequency of healed infants was 81.5% in the human breast milk group compared to 76% in the 1% hydrocortisone group (p < 0.24). 39 Farahani et al. (2013) topically applied breast milk to 152 infants with diaper dermatitis and found that it was as effective as 1% hydrocortisone. 40 Similarly, studies by Gozen et al. (2014) 41 and Seifi et al. (2017) 42 revealed that breast milk is effective in diaper dermatitis. In three separate studies, it was found that the umbilical cord drying time was shortened and the cord fell off faster in infants treated with topically applied breast milk.43–45 While the cited studies demonstrate the remarkable efficacy of breast milk in various wound healing scenarios, it is important to clarify that these findings primarily originate from animal models and observational studies. Direct clinical application in human populations requires more rigorous research through controlled clinical trials to confirm these promising results. From accelerating corneal epithelial defect healing to effectively treating conditions such as atopic eczema and diaper dermatitis, evidence consistently highlights the potential of breast milk as a natural medicine. Although our in vitro study confirms the wonderful properties of breast milk on wound healing, the lack of clinical application outside a limited number of clinical trials points to the need for further studies in this area.
In this study, in addition to the effects of breast milk on wound healing at different lactation stages, the levels of netrin-1, an important factor in inflammation and cell migration, were evaluated in L929 cells following breast milk applications. While the netrin-1 level in the control group L929 cells was determined as 490.1 ± 6.5 pg/mL, it was determined as 410.9 ± 2.0 pg/mL (p: 0.0142) in the colostrum applied group, 392.6 ± 1.5 pg/mL (p: 0.0051) in the transition milk applied group, and 376.6 ± 4.5 pg/mL (p:0.0003) in the mature milk applied group. It was observed that netrin-1 levels decreased significantly compared to the control in all three different stages of breast milk (Fig. 3).

Netrin-1 levels after application of breast milk from different lactation stages to L929 cells (*p < 0.05 versus control; **p < 0.01 versus control; ***p < 0.001 versus control).
Netrin-1 is a molecule that plays an important role in the inflammation process. Inflammation is a natural defense mechanism initiated by the body to repair damaged tissues and eliminate pathogens. Netrin-1 affects the course of inflammation by regulating a number of biological processes such as cell migration, cell adhesion, and cell signaling during inflammation. Interestingly, in this study, despite the decrease in netrin-1 levels, it was observed that the wound healing rate increased in the groups administered colostrum, transitional milk, and mature milk compared to the control. This finding highlights that wound healing is driven not just by a single molecule or mechanism but by the interaction of a number of different factors. Thus, it suggests that the complex components of breast milk may contribute to the wound healing process in a multiple and perhaps synergistic manner.
Netrin-1 was initially identified as controlling the guidance of neuronal axons in the central nervous system. It has since been reported that netrin-1 also plays key roles in immune cell migration, angiogenesis, and cell survival. Netrins have been identified as being strongly linked to wound healing through epithelial closure. This study suggests that macrophages also express ECM genes in vitro and in vivo, which potentially contributes to the structural support of wound tissue, and that macrophage-derived netrin-1 provides guidance signals to regulate wound healing. 46 Netrins are laminin-related proteins that regulate epithelial morphogenesis. Netrins can trigger the cellular mesenchymal–epithelial transition (MET) mechanism and reverse the effect of EMT-inducing factors. For example, Cripto-1 overexpressing mammalian mammary epithelial cells become invasive, but this can be ameliorated by exogenous netrin-1. It has been demonstrated that netrin pathways can control epithelial plasticity by regulating both mesenchymal motility and epithelial stability. Their effects on wound healing vary depending on the tissue or cell type. Netrins trigger the epithelialization of cutaneous wounds and maintain the homeostasis of skin tissue. 47 According to the findings of this study, breast milk treatment reduced netrin-1 production of L929 fibroblasts. This situation can be considered an advantageous situation in terms of preserving the mesenchymal properties of fibroblasts and reducing the MET process.
The immune system plays a central role in regulating the tissue healing process. In acute skin wound healing, cytokines such as TGF-β1 and PDGFs are secreted and play a critical role in the activation of fibroblasts, neutrophils, and macrophages. In this study, netrin-1 has regulatory roles in the migration of immune system cells. In the initial stage of wound healing, neutrophils are the first immune cells recruited to injured tissue. The third stage of wound healing begins with the recruitment of fibroblasts, keratinocytes, and epithelial cells to the injury site. 48 Netrin-1 has been identified as a potent inhibitor of leukocyte chemotaxis. Netrin-1 inhibits chemokine-mediated migration of these cells depending on the dose and can block leukocyte accumulation. It is known that the main inflammatory cytokines TNF-α and IFN-γ cause leukocyte accumulation. Netrin-1 expression decreases due to the increase in TNF-α and IFN-γ in acute inflammation. This indicates that netrin-1 is inversely related to inflammatory cytokine expression and leukocyte invasion in this tissue. 49 A recent study showed that netrin-1 augment chemokinesis of CD4+ T effector cells. According to the results, netrin-1 enhances 2.21-fold, 1.97-fold, and 1.47-fold the number of migrating T cells in netrin-1 concentrations of 0.1, 0.5, and 5 μg/ml, respectively, in microfluidic chamber. Accordingly, the more netrin-1 did not increase the chemotaxis rate of the cells. It is understood that the level of netrin-1 can affect the cellular regulation paracrinely in a dose-dependent manner. 50 In summary, proinflammatory cytokines suppress netrin-1 expression. According to the study’s findings, breast milk’s suppression of netrin-1 expression in L929 cells may be due to the presence of proinflammatory cytokines. The inflammatory environment that breast milk serves in wound healing should be clarified through further research.
Limitations
This study is based on in vitro experiments using only L929 fibroblast cells. Although this approach allows for controlled experiments, it may not fully reflect the complexity of in vivo wound healing where various cell types and physiological factors interact. The in vitro scratch assay used in the study provides a simplified model of wound healing compared to in vivo wound models. The results may not fully reflect the multifaceted aspects of wound healing observed in living organisms. The study focused on the effects of breast milk at different breastfeeding stages, but did not investigate the specific bioactive components responsible for the observed effects. Understanding the contributions of individual components may provide deeper insights into mechanisms of action. The use of a single cell line (L929 fibroblasts) may limit the generalizability of the findings. The inclusion of other relevant cell types involved in wound healing, such as immune cells or endothelial cells, may provide a more comprehensive understanding of the effects of breast milk.
Since the aim of our study was to investigate general trends and effects in different samples, using breast milk from three different mothers was considered a reasonable approach. If the study had aimed to detect smaller differences between the groups, it would have been useful to study a larger number of samples. Although the study demonstrates the potential benefits of breast milk on wound healing in a cellular model, its clinical relevance to wound management in patients needs to be determined through further in vivo and clinical studies. Addressing these limitations in future research may strengthen the understanding of the therapeutic potential of breast milk in wound healing and facilitate its translation into clinical practice.
Conclusion
In this study, wound healing, a complex process involving various cellular and molecular events aimed at restoring tissue integrity, was investigated. The potential wound healing properties of breast milk samples from different lactation stages were examined using an in vitro model. It has been found that mature breast milk, in particular, may have beneficial effects on wound healing processes, including cell proliferation, migration, and antioxidant activity.
Future investigations should prioritize in vivo experimental and clinical examinations to assess the safety of utilizing breast milk topically for wound healing, along with exploring its mechanisms of action.
Footnotes
Authors’ Contribution
Conceptualization: C.A.A. and H.I.T.; formal analysis and investigation: C.A.A., S.P., S.Y., and H.I.T.; writing—original draft preparation: C.A.A., S.Y., and H.I.T.; and writing—review and editing: S.P. and C.A.A. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No fund, grant, or other support was received.