
Abstract
Introduction:
Lithium remains a gold standard treatment for bipolar disorder including during peripartum. Historically, guidelines advised against breastfeeding while taking lithium though recent data suggest it is acceptable for a healthy infant. Lack of awareness of acceptability contributes to decreased patient and clinician comfort and low breastfeeding rates. We report current breastfeeding rates, monitoring practices, and infant outcomes with lithium exposure in breastmilk at our institution.
Methods:
A retrospective chart review was conducted at a single academic medical center using records from 2013 to 2023. Electronic medical records were queried to identify patients prescribed lithium postpartum. Data were collected on timing of lithium initiation, lithium dose and concentration, breastfeeding status, and infant outcomes.
Results:
A total of 18 cases of lithium use in the postpartum period were identified. A total of 39% (n = 7) of patients taking lithium postpartum breastfed. Most patients, 61% (n = 11), initiated lithium prior to pregnancy, 11% (n = 2) initiated during pregnancy and 27% (n = 5) started postpartum. Four infant charts were reviewed with no reports of adverse events. Of these infants, average maternal lithium dose was 750 mg daily, with an average maternal serum lithium concentration of 0.62 mmol/L and average infant serum lithium concentration of 0.16 mmol/L.
Conclusion:
Our data demonstrate most patients using lithium postpartum have been taking lithium long-term and are not breastfeeding. Lithium exposure in breastmilk appears to be tolerated by healthy infants. There is a need for ongoing research and education on acceptability and infant monitoring recommendations to support patients who would like to breastfeed while on lithium.
Introduction
Bipolar disorder is a chronic illness, affecting 4.4% of the population in the United States, with similar rates in men and women. 1 With an average onset age of 18 years, people with potential for pregnancy are impacted by the disorder and by treatment efforts throughout most of their reproductive years. Peripartum is a vulnerable time for patients with bipolar disorder, with increased risk of mood episodes and hospitalization. 2
Pharmacotherapy is the primary treatment for bipolar disorder. Most patients are advised to continue effective mood stabilizing medications throughout pregnancy and postpartum, with the exception of valproic acid, which is avoided during pregnancy due to a high risk of birth defects and developmental delays. 3 Lithium remains a reasonable and often recommended treatment for patients with bipolar disorder during pregnancy, acknowledging a risk of fetal cardiac abnormalities when taken in the first trimester.4–6 Potential risks of lithium use during lactation are not well described. Lithium transfer to breastmilk is variable, with an estimate of 50% of the maternal serum concentration present in breastmilk. 7 Clinician recommendations around breastfeeding and lactation are also variable. Some clinicians suggest noninvasive monitoring of infants exposed to lithium via breastmilk by tracking infant weight and feeding habits, 8 while other guidelines advise a higher level of concern, describing the exposure as potentially dangerous to infant health and recommending patients avoid breastfeeding while taking lithium.9–11 Hale and colleagues advise that infant lithium exposure through breastmilk is acceptable in a healthy term infants and recommend lab monitoring in the infant at 6 weeks of age. 12 The relative paucity of lactation data related to lithium exposure likely contributes to inconsistency in the infant monitoring guidelines and varying clinical practices. Breastfeeding is generally recommended due to the numerous short- and long-term health benefits for the breastfeeding person and the infant. 19 Conflicting information regarding potential concerns with lithium exposure and reported benefits of breastfeeding can contribute to distress for patients when considering feeding plans. In this study, we assessed the rates of breastfeeding during the use of lithium and associated outcomes.
Methods
A retrospective chart review was conducted at a large, 2,000-bed academic medical center in the Midwest, United States between January 1, 2013, and December 31, 2023. This research was reviewed and deemed exempt by the Mayo Clinic Institutional Review Board. Inclusion criteria included any female patient prescribed lithium in the postpartum period. An electronic retrieval tool was used to search patient medical records for the key terms “lithium” and “pregnancy.” Infants of the postpartum individuals were also included. Patients were excluded if they did not consent to the use of their data for the purpose of medical research. For patients included, the variables abstracted included demographics, indication for lithium, timing of initiation of lithium, the daily dose of lithium postpartum, lithium formulation, parent and infant lithium levels, and whether the postpartum individual provided breastmilk to their infant. Data collected from infants’ charts, where available, included laboratory studies, reported adverse outcomes, and developmental concerns up to the first year of life.
Results
Eighteen cases of lithium use in the postpartum period were identified for inclusion (Table 1). The average age (± standard deviation [SD]) at delivery was 30.5 (5.05) years and all participants identified as female. Ninety-four percent of participants identified as White. The most common indication for treatment with lithium was bipolar disorder type I (67% [n = 12]) followed by bipolar disorder type II (28% [n = 5]) and postpartum psychosis (5% [n = 1]) (Table 1). A total of 39% (n = 7) of patients taking lithium postpartum provided any amount of breastmilk to the infant. Most patients (61% [n = 11]) initiated lithium prior to pregnancy, 11.% (n = 2) initiated lithium during pregnancy, and 28% (n = 5) started postpartum (Fig. 1). Among all patients who breastfed, the mean daily lithium dose (± SD) was 857 (207) mg. Patients were more likely to breastfeed when lithium was initiated prior to the pregnancy (54%) as compared with when lithium was initiated postpartum (20%). Neither of the two patients who started lithium during pregnancy breastfed.
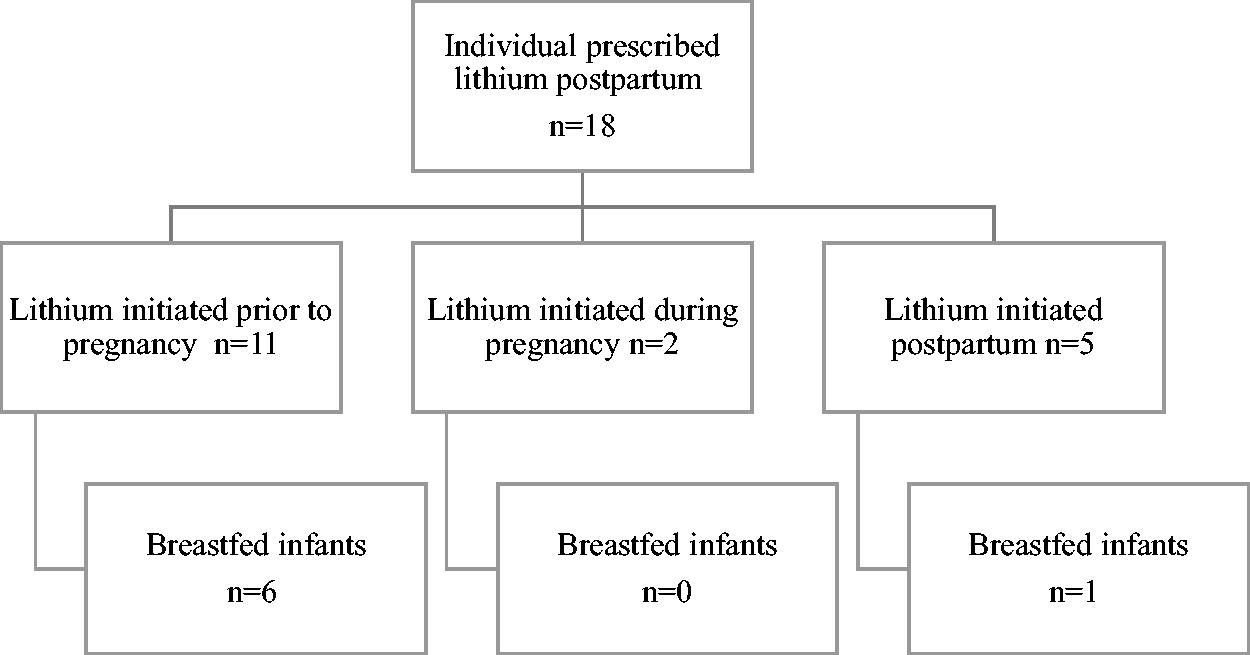
Feeding plan trajectories of individuals prescribed lithium postpartum.
Descriptive Statistics of Women Prescribed Lithium Postpartum (n = 18)
Seven infants were exposed to lithium through breastmilk. Six infants were delivered at term with one infant born preterm at 34 weeks and 4 days gestational age. Six of the seven were also exposed to lithium in utero, with one patient initiating lithium postpartum. Four of the infant charts were available and reviewed through the first year of life, during which time, breastmilk is a primary source of nutrition for infants. Two infants were exclusively breastfed, and two infants received a mix of breastmilk and formula. Specific details of each feeding plan were not documented. Laboratory monitoring recommendations for each infant varied, though all clinicians recommended serial laboratory studies (thyroid stimulating hormone [TSH], blood urea nitrogen [BUN], creatinine [Cr], lithium level) every 3–4 or 4–6 weeks during exposure to lithium via breastmilk. None of the infants received more than two blood draws, despite clinician recommendations for more frequent laboratory monitoring. Of the four available infant charts, three infants were exposed to lithium both in utero and via breastmilk. The average maternal lithium dose (± SD) was 750 (150) mg daily, with an average maternal serum lithium concentration (± SD) of 0.62 (0.23) mmol/L and average infant serum lithium concentration (± SD) of 0.16 (0.17) mmol/L. All infant lithium levels fell below 0.1 mmol/L within the first 2 weeks of life (Table 2). Maternal and infant lithium levels were not drawn simultaneously. There were no adverse events noted in the infant medical records related to lithium exposure including no diagnosed development delays, no cases of lithium toxicity, and no renal or thyroid abnormalities.
Infant Exposure to Lithium via Breastmilk with Reported Maternal and Infant Serum Lithium Concentrations
IR, immediate release; L, liter; mg, milligram; mmol, millimole; n/a, not available; SD, standard deviation; SR, sustained release.
Discussion
Lithium is a commonly prescribed mood stabilizer that patients take for long-term management of psychiatric illness. Many patients prescribed lithium will become pregnant and may want to breastfeed. In contrast to other medications commonly used to treat psychiatric illness, such as lamotrigine and antipsychotics, there are fewer data available on lithium during lactation. There are conflicting recommendations on the acceptability of lithium during lactation, which contributes to clinician and patient unease. The breastfeeding rate in this study cohort was 39% of infants receiving any amount of breastmilk, which is substantially lower than the national average of 83.1% of infants in the United States ever receiving some breastmilk. 13
Common themes noted during chart review highlight potential current barriers to breastfeeding in this patient population. The following themes were present in two or more cases. (1) Clinicians provided inconsistent information to patients regarding the safety of providing breastmilk while taking lithium. Once a cautionary recommendation was received, breastfeeding was unlikely to be pursued, even if additional education was later provided regarding acceptability. (2) Risk versus benefit discussions were not routinely documented in the medical record regarding lithium exposure in lactation. (3) Patients expressed guilt if they were told they should not breastfeed related to taking lithium. In one of these cases, the patient expressed fear she was “not a good enough mother” and shared how this contributed to ongoing depressive symptoms postpartum. (4) Infant monitoring recommendations were inconsistent for infants exposed to lithium in the breastmilk as is outlined in Table 1. This resulted in the infants exposed to lithium undergoing laboratory monitoring and follow-up visits at varying times. In one case, a pediatrician evaluated the infant every 3 days during office visits, and in another instance no infant monitoring labs were obtained for several months after exposure.
Lithium use during lactation is often not recommended by health care providers out of caution and a desire to avoid harm to the infant. However, there are still limited data on healthy term infants to support this concern. While case reports with potential adverse infant outcomes have been cited, larger case series have been reassuring and most early infancy concerns have been attributed to in utero exposure to lithium, rather than to breastmilk exposure.7,15–18 Imaz and colleagues followed eight infant pairs with exposure to lithium during pregnancy and during exclusive breastfeeding. 16 They noted that although umbilical cord lithium concentrations were slightly higher than maternal plasma concentrations, infant lithium concentrations decreased with time while exclusively breastfeeding. While cases of hypotonia and fetal acidosis at delivery were posited as potentially related to in utero lithium exposure, there were no concerns reported in the study about lithium exposure in breastmilk. By 1 week of age, all infants had normal serum Cr and TSH concentrations. There were no growth or developmental concerns reported for any of the infants. Lithium transfers to breastmilk and can result in measurable infant levels. At the same time, the health benefits of breastfeeding for lactating individuals and their infants have been well established. 19 The majority of reported infant-related adverse effects have been attributed to in utero exposure and have not been consistently linked to transfer through breastmilk.
Clinicians routinely lead discussions with patients regarding potential risks of continuing pharmacotherapy during pregnancy and potential risks of undertreated or untreated psychiatric illness if they were to discontinue treatment. We suggest a similar approach with lithium and lactation, allowing the existing evidence, patient values, clinical stability, and infant health to guide decision-making. A third trimester lactation consult should be offered to review feeding options with an emphasis on protecting parental sleep to support mood stability. 20 Breastfeeding can be compatible with parental sleep. Several studies have reported that evening or overnight breastfeeding may be associated with an average of 40–45 minutes more sleep for parents compared with formula feeding. 14 ,21 Maternal lithium levels should be monitored during pregnancy and postpartum, ensuring a plan for dose adjustments after delivery, as elevated maternal levels will lead to elevated infant levels. If a parent chooses to breastfeed while on lithium, Hale and colleagues recommend infant laboratory results be obtained at 6 weeks of age including serum lithium concentration, BUN, Cr, and TSH. 12 If there are concerns about difficulty with feeding, poor infant weight gain, lethargy, hypotonia, or delayed developmental milestones, there should be a low threshold to supplement with human donor milk or formula and to check infant levels at that time, along with comprehensive assessment of the infant by a health care professional trained in pediatric care. For a patient to successfully breastfeed while taking lithium, the patient, prescribing clinician, lactation team, and pediatrician, or infant clinician all require a level of familiarity and comfort with lithium use during lactation.
There are several limitations of this study. First, we present a small sample size of mother–infant dyads. Due to limitations of the study and the medical record system, we were not able to access all infant records. Second, we cannot report on the specific details of infant feeding plans or the length of breastfeeding, as these were not well documented in the medical record.
Conclusion
In our study, postpartum patients who take lithium have taken it continuously since prior to conception, indicating that they have found it helpful for maintaining mood stability. In this 10-year case series from a large midwestern academic medical center, most patients taking lithium did not breastfeed, regardless of when they initiated the medication. Most of these patients also did not receive documented education regarding risks and benefits of breastfeeding while taking lithium, with mixed levels of clinician support for breastfeeding while on lithium. Among the four infants whose histories were accessible for review, there were no reports of adverse outcomes within the first year related to lithium and no toxic infant lithium levels. Patients’ desire to breastfeed while taking lithium may be supported by medical professionals while providing supervision of infant growth, feeding, and development.
Footnotes
Authors’ Contributions
M.N.K.: Conceptualization, investigation, resources, methodology, writing—original draft; J.G.L.: methodology, resources, writing—review and editing; L.A.K.: writing—review and editing; K.M.M.: conceptualization, resources, writing—review and editing; R.L.H.: conceptualization; H.N.B.: supervision, conceptualization, resources, writing—review and editing.
Author Disclosure Statement
The authors report no competing interests.
Funding Information
No financial support for this work.