
Abstract
Objective:
To analyze the factors associated with weaning in infants with cow’s milk allergy (CMA) treated at a food allergy reference center in a state in the northeast of Brazil.
Method:
A prospective cohort study, with a case group (children with CMA) and two control groups (symptomatic nonallergic children [SC] and asymptomatic [AC]). At the beginning of the study, 30 children comprised the CMA group, 84 the SC group, and 52 the AC group. Survival analysis was performed to compare breastfeeding time between the three groups and an adjusted linear regression model to verify the factors associated with breastfeeding time.
Results:
At the beginning of the study, 33.3% of children in the CMA group, 17.1% in the SC group, and 69.6% in the AC group were exclusively breastfeeding (p = 0.005). The most common factors for weaning in children with CMA were the cow’s milk elimination diet (30%), allergic symptoms in the child (20%), and breast engorgement (20%). Children who used a cup as a means of offering infant formula spent 281 more days breastfeeding compared with those who used a baby bottle (Bstd = 1.39; p = 0.031).
Conclusion:
Children with CMA and nonallergic gastrointestinal complaints weaned earlier compared with asymptomatic children. The main causes of weaning in CMA children were maternal difficulty adhering to the elimination diet, breast engorgement, and allergic symptoms in the child. Using a cup was the main factor associated with longer breastfeeding duration, regardless of gastrointestinal symptoms and socioeconomic factors.
Introduction
The World Health Organization (WHO) recommends breastfeeding for at least 2 years of age and exclusively until the sixth month. 1 Breastfeeding is globally recognized as one of the best public health strategies for child survival to reduce the risks of diseases in adulthood and health care costs.2,3 However, in low- and middle-income countries, exclusive breastfeeding (EBF) is present in only 37% of children aged 0–6 months. 4 In Brazil, data from the latest Estudo Nacional de Alimentação e Nutrição Infantil report a prevalence of 45.7% of EBF, and the Northeast region has the lowest rate in the country (39%).5,6 In Brazilian children up to 2 years of age, the prevalence of breastfeeding is 60.3%, but, in children with cow’s milk allergy (CMA), which is an immune system response to cow’s milk proteins, the prevalence is 0.5% in the same age group.6,7
Interruption of breastfeeding can occur for a variety of reasons. Parents’ concern regarding the behavioral instability of newborns (crying, irritability, unstable sleep, etc.), the insufficient production of breast milk (BM) reported by mothers, the early introduction of other foods and infant formulas in the first days of the baby’s life, the marketing of infant formula industries, limited public policies encouraging breastfeeding, and the suspicion of allergies and reactions to BM are described as causal factors for weaning in low- and middle-income countries. 8
In recent decades, the prevalence of food allergies has been increasing, 9 but information about their prevalence is still based on estimates. Cow’s milk is one of the main food allergens in childhood and, in developed countries, it is estimated that the prevalence of CMA is around 0.5–3% of children in the first year of life. 10 In Brazil, an observational study conducted with pediatric gastroenterologists reported a prevalence of 5.4% and an incidence of 2.2% of CMA in children aged 24 months or less, treated in health services across 20 municipalities in the 5 Brazilian regions (North, Northeast, South, Southeast, and Central-West).9–11 In a cross-sectional study carried out in the city of Limoeiro, in northeastern Brazil, the prevalence of CMA in preschool children was 1.7%. 12 CMA is considered a global public health problem, 13 with social and economic repercussions for both families and governments. Expenses related to food allergies are considerable, varying in each country depending on funding and health policy. 14
Food allergy manifests itself with nonspecific symptoms, which are often difficult to distinguish from gastrointestinal disorders and can also affect the respiratory, skin, cardiovascular, and neurological systems.9,15 Treatment consists of excluding cow’s milk and derivatives from the child’s and mother’s diet (when the infant presents reactions to cow’s milk through BM), with the inclusion of hypoallergenic or nonallergenic infant formulas, when breastfeeding is unfeasible or insufficient.9,15
The exclusion diet for the treatment of CMA may be a risk factor for malnutrition 10 and for weaning from BM, although studies evaluating the rates and reasons for weaning in infants with this disease are still scarce. Children on EBF have lower rates of CMA, probably due to the lower allergenicity of proteins contained in BM, the presence of immunoregulators in human milk, and the promotion of intestinal microbiota that favors oral tolerance.9,15
Although current guides for the treatment of CMA reinforce the importance of maintaining breastfeeding in managing the disease, 16 weaning rates in this group of children are still high. 7 Therefore, it is essential that health professionals understand this relationship and use health education as a transformative instrument of specialized guidance to support mothers of children with CMA and continue breastfeeding.17,18
Specialized health services with established clinical protocols, such as the Reference Center for Food Allergy of Sergipe (RCFAS), 19 are important for managing this disease and reducing public costs with special formulas. However, more evidence is required to enable clinicians from food allergy specialized health services to make decisions to prevent weaning in cow’s milk allergic children.
Therefore, this study aims to analyze the factors associated with weaning in infants with CMA assisted at the RCFAS.
Methods
A prospective cohort study was carried out in the state of Sergipe/NE-Brazil to describe the causes of weaning from the maternal perspective and investigate the factors associated with weaning from BM in children with CMA group compared with symptomatic infants with a negative oral food challenge (OFC) (symptomatic control group [SC]) and to infants without symptoms (asymptomatic control group [AC]), during a follow-up period of 18 months. The diagnosis of CMA was made by the medical team at the RCFAS, at the Federal University of Sergipe, by performing OFC after 4–8 weeks of a cow’s milk exclusion diet. Breastfeeding infants underwent the reintroduction of cow’s milk into the maternal diet, according to an internationally established protocol. 20
Participants
The study included all children aged 0–6 months, with suspected CMA admitted to RCFAS between February 2019 and February 2021, and asymptomatic children recruited from the Institute for Promotion and Health Assistance for State Servants of Sergipe and at Maternity Santa Isabel from July 2020 to March 2021. Sampling was for convenience, with children cared for in these institutions being invited to participate in the study during the aforementioned periods.
The exclusion criteria for all children studied were prematurity (<37 weeks of gestation), the presence of inflammatory bowel disease, celiac disease, cystic fibrosis, autoimmune disease, chromosomal abnormalities, developmental delay, and other presumed or diagnosed chronic diseases.
Study variables
Socioeconomic and demographic data, as well as the age at breastfeeding initiation and termination, were collected. Additional data included the type of breastfeeding at the beginning of the study, use of infant formulas, maternal reasons for weaning from breast milk, and the child's anthropometric data at the start of the study.
Instruments and data collection
The study variables were collected through a structured questionnaire with questions about maternal education level and child nutrition. Information on ownership of household assets, parental income, water, and sanitation was used to construct a wealth index by using the method of Brazilian Association of Research Companies (ABEP), where a higher index means better socioeconomic status. 21
Anthropometric measurements of the children’s weight and height were also taken, according to standardized protocols.22,23Anthropometric indices of height/age (HAZ), weight/height (WHZ), weight/age (WAZ), and BMI/age (BMIZ) were measured in Z-score using the WHO ANTHRO version 2.0.2 program. Children were classified as stunted if HAZ < −2 Z-score. Children with WAZ < −2 Z-score were classified as underweight and with WHZ and BMIZ < −2 Z-score were classified as thin. It was considered overweight when WAZ, WHZ, and BMIZ were >2 Z-score. 23
Data analysis
Data were analyzed using SPSS version 22.0. Student’s t, Pearson’s Chi-square, Mann–Whitney, Fisher’s exact, and survival analysis tests were used as methods for comparative analysis of variables between the three study groups. The mothers’ responses about the factors that motivated weaning from breastfeeding were separated by study groups and treated for standardization, and then a program was produced in Python programming language to automate the counting of these responses.
Categorical variables were described using absolute and relative frequency. Survival curves for continued breastfeeding were estimated using the Kaplan–Meier method. The hypothesis of equality of survival curves for continued breastfeeding was tested using the Gehan–Breslow test (generalized Wilcoxon).
Continuous variables were described using mean, median, standard deviation, and interquartile range. The hypothesis that continuous variables adhere to normal distribution was tested using the Shapiro–Wilks test. When confirmed, the hypothesis of equality of means between two independent samples was evaluated using the t test; otherwise, the hypothesis of equality of medians between two independent samples was evaluated using the Mann–Whitney test. To evaluate factors associated with breastfeeding time, linear regression models were estimated, and crude and adjusted regression coefficients were estimated for the study groups and relevant variables. The software used was R Core Team 2022 (Version 4.1.2), and the significance level adopted throughout the study was 5%.
Ethical aspects
This study was approved by the Research Ethics Committee of the Federal University of Sergipe (CAAE 97662918.0.0000.5546) and respected the ethical principles of research with human beings, with the voluntary written consent of the participating guardians.
Results
Of the 207 children initially included in the study, 155 made up the case group (children suspected of having CMA), and 52 children made up the AC group. Of the children in the case group, 114 (73.5%) underwent the OFC, of which 30 (26.3%) presented positive OFC and were allocated to the CMA group, and 84 (73.7%) remaining children with negative OFC comprised the SC group.
Due to the COVID-19 pandemic, there was a sample loss during follow-up in the SC and AC groups due to voluntary withdrawal and abandonment by parents, not returning to the research site, and not responding to researchers’ phone calls. Thus, at the end of the 18-month follow-up, the total sample was 94 participants. The CMA group remained with 30 (32%) participants, the SC group totaled 41 (44%), and the AC group had 23 (24%) children. In the CMA group, 90% of children had gastrointestinal symptoms.
No statistically significant differences were detected in age, sex, type of infant feeding, socioeconomic status, and anthropometric parameters at the beginning of the study between children who remained and those who were lost to follow-up (p > 0.05).
Of the total number of children evaluated, 2 (2.1%) were short (H/A < −2) and 3 (3.2%) (W/A >2) were overweight for their age at the beginning of the study. The overall average age of the three groups of children was 2.9 months. Regarding socioeconomic level, 40 (42.1%) families had low middle income, according to criteria from the ABEP, 21 with no statistical difference between the groups (p = 0.372). The SC group was the group with the lowest rates of breastfeeding (34.1%) upon admission to RCFAS, with a greater number of children who received formula in the maternity ward (43.9%), who were using pacifiers (70%) and who started complementary feeding earlier (at 120 days of the child’s life).
Breastfeeding rates and duration
At the beginning of the study, 70 (74.4%) children were breastfed, and 33 (35.1%) children were exclusively breastfed. Children in the asymptomatic control group had higher rates and duration of EBF. Sixteen (69.6%) children in the asymptomatic control group were exclusively breastfed until the time of the first evaluation, whereas 10 (33.3%) children in the CMA group and 7 (17.1%) children in the symptomatic control group were exclusively breastfed during the period beginning of the study (p = 0.005; Table 1). At the end of the study, 51 (54.2%) breastfeeding women continued to breastfeed their children, of which 18 (78.3%) were in the AC group, 17 (56.7%) in the CMA group, and 16 (39.0%) in the SC group (p = 0.009; Table 2).
Length of Exclusive Breastfeeding at the Beginning of the Research by Study Group
Group with cow’s milk allergy.
Symptomatic control group.
Asymptomatic control group.
Prevalence of Breastfeeding at the Beginning and End of Follow-up
Group with cow’s milk allergy.
Symptomatic control group.
Asymptomatic control group.
Interquartile range.
Absolute frequency.
Percentage relative frequency.
Distinct subgroups at the 5% level for the Bonferroni Z test (proportions) or Dunn (medians).
Kruskal–Wallis test.
Pearson Chi-square test.
The survival analysis illustrates the curve of breastfeeding time throughout follow-up (Fig. 1). The CMA group presented a design in the breastfeeding proportion curve similar to the SC group, demonstrating a drop in the continuity of breastfeeding at 4 months of follow-up and maintaining the curve in decline until around 10 months of follow-up, when, then, the curve stabilizes.
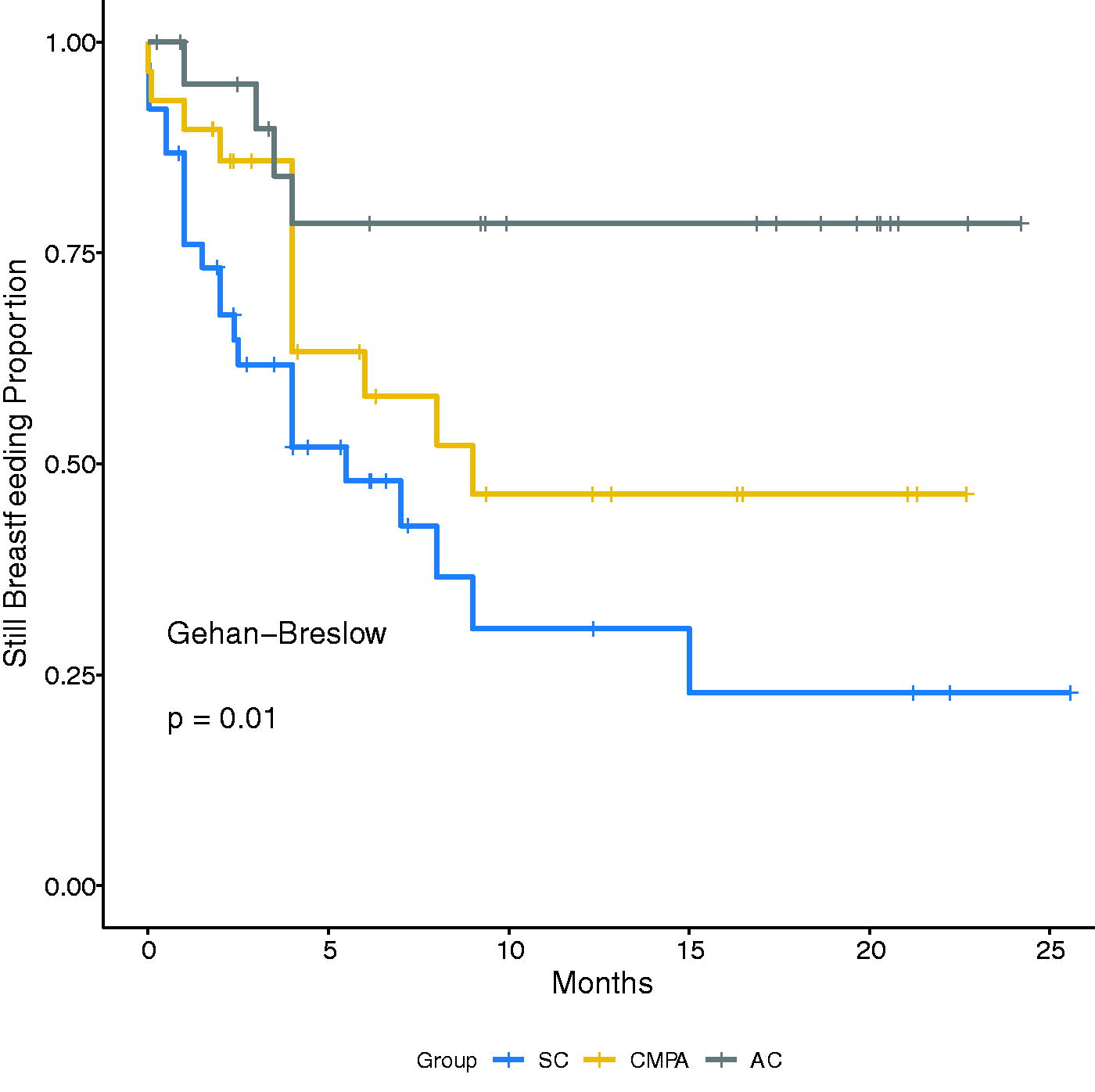
Survival curve of breastfeeding time by group of children. AC, asymptomatic control group; CMPA, group with cow’s milk allergy; SC, symptomatic control group.
Causes of weaning from the maternal perspective and factors associated with breastfeeding duration
The causes of weaning reported by mothers are described in Table 3. The most frequent responses in the CMA group were the difficulty in continuing breastfeeding while following the cow’s milk and derivatives exclusion diet (30%) and, with equal rates (20%), allergic symptoms in the child and breast engorgement. In the SC group, insufficient production of BM and the child’s refusal to breastfeed predominated in an equal percentage (20%), as well as the dairy exclusion diet in the diagnostic investigation phase of CMA (10%) and the symptoms presented by the child (10%). Only one mother in the AC group had weaned, reporting that the child refused BM.
Causes of Weaning from the Maternal Perspective
Group with cow’s milk allergy.
Symptomatic control group.
Asymptomatic control group.
Absolute frequency.
Percentage relative frequency. Note: Children who were not weaned were not included in the table: 20 (21.3%) CMA, 21 (22.3%) SC, and 22 (23.4%) AC.
In the linear regression analysis to verify the main factors associated with breastfeeding time (Table 4), it was observed in the adjusted analysis that children who used a cup as a means of offering infant formula spent approximately 281 more days breastfeeding compared with children who used baby bottles (p = 0.031), with an expressive standardized beta result (Bstd = 1.39). Children from families with better socioeconomic conditions weaned earlier in the unadjusted analysis (p = 0.016), losing this association in the adjusted analysis. The presence of CMA or nonallergic gastrointestinal symptoms was not associated with breastfeeding duration in the adjusted linear regression.
Factors Associated with Breastfeeding Duration in Infants with and Without Allergies to Cow’s Milk: Unadjusted and Adjusted Associations
Adjusted model: R²: 0.354. R² adjusted: 0.134. RMSE (Root Mean Square Error): 162. Shapiro–Wilk: p = 0.119. Breusch–Pagan: p = 0.303. Durbin–Watson: p = 0.900. VIF (Variance Inflation Factor): 1.12–2.38.
95% confidence interval.
Regression coefficient.
Lower limit.
Upper limit.
Standardized regression coefficient.
Group with cow’s milk allergy.
Asymptomatic control group.
Symptomatic control group.
Discussion
The present study is a pioneer in Brazil in the evaluation of breastfeeding in infants from low- to middle-income regions with CMA, comparing infants with nonallergic gastrointestinal symptoms and healthy children. We observed that children without gastrointestinal symptoms remain breastfed for longer and children with nonallergic gastrointestinal symptoms are weaned earlier. The persistence of gastrointestinal symptoms in this group of children may have contributed to the use of pacifiers and formulas with the aim of reducing symptoms and, consequently, negatively influenced the continuity of breastfeeding.24–28
Parents of children with gastrointestinal symptoms may be more susceptible to the appeal of the industry advertising infant formulas as a solution for such symptoms. It is likely that the parents of symptomatic nonallergic children in the present study were influenced by this marketing in the hope of improving their children’s clinical condition.29,30 However, as this is an observational study, it is not possible to establish a causal relationship and, therefore, the early introduction of infant formula might be the reason for the symptomatology in groups, as only 33% and 17% were exclusively breastfed from 0 to 6 months of age in the CMA and CS groups, respectively. Survival analysis demonstrated a significant linear decline in breastfeeding rates around the fourth month of follow-up in the three study groups. Although only one mother reported that returning to work was the cause of weaning, the Brazilian maternity leave is up to 4 months, which may probably have an impact on breastfeeding in the overall studied population, although misperceived by mothers.24,26,31,32 A recent review and meta-analysis demonstrated that women’s return to work is one of three main causes of weaning, negatively affecting the initiation and duration of breastfeeding, as well as the prevalence of EBF, with the introduction of infant formulas, especially if the mother works full-time. 33
In the analysis of maternal perception about the reasons for weaning, it was observed that the main reasons in symptomatic nonallergic children were perceived insufficient maternal milk production, the symptoms presented by the child, their refusal to breastfeed, and the cow’s milk elimination diet during the CMA investigation period, and the latter was also described by the group of children with CMA. Maternal stress, baby crying, lack of guidance on breastfeeding, and lack of family and social support influence BM production, negatively interfering with breastfeeding.24–26
Functional gastrointestinal disorders (FGIDs) resulting from the immaturity of the immune and gastrointestinal systems affect 50% of babies from 0 to 6 months of age, with the most frequent symptoms being regurgitation, colic, and intestinal constipation. 34 Such symptoms generate suffering in children and anxiety in parents, reduce the family’s quality of life, and can cause depressive symptoms in the mother and fragility in the mother–child bond, thus reducing the duration of breastfeeding. Therefore, the diagnosis of FGIDs should be confirmed when gastrointestinal diseases and food allergies are ruled out, with appropriate guidance for the child’s parents so that breastfeeding can be continued.34,35
Possibly, the persistence of symptoms, the lack of definition in the diagnosis, the maternal elimination diet, anxiety, and concern related to the baby’s health may also have culminated in the interruption of breastfeeding by the mother of children with nonallergic symptoms.36,37 Carrying out OFC to confirm the diagnosis of CMA is of fundamental importance to reduce the time on the cow’s milk elimination diet in nonallergic patients and can minimize the challenges for continuing breastfeeding. 20 Only 26.3% of the 155 children in our study who underwent OFC testing had positive results, similar to the prevalence observed by Vasconcelos et al., 38 which demonstrates the importance of OFC for the diagnostic elucidation of CMA and the reduction of the duration of cow’s milk elimination diets in nonallergic patients, thus minimizing the challenges to the continuation of breastfeeding. It was also observed that the weaning rate in the CMA group was lower when compared with symptomatic nonallergic children. A possible explanation for this finding is due to the fact that symptomatic children are discharged from RCFAS after negative OFC, unlike children with positive OFC, who are maintained in this reference center for the treatment of food allergies. The RCFAS team more strictly follows national and international clinical protocols for the management of gastrointestinal diseases, providing family support to maintain breastfeeding.9,19,35,39 Furthermore, most children with suspected food allergies arrive at their first RCFAS appointment with a treatment formula for CMA, prescribed by the responsible pediatrician. The low adherence of Brazilian pediatricians to consensus and guidelines for gastrointestinal diseases can lead to less than optimized assistance for these complaints and consequent weaning. 40
Regarding the main factors associated with the duration of breastfeeding in the 18 months of follow-up of children, the use of a cup was the route of offering dairy supplementation that demonstrated greatest protection in the continuation of breastfeeding. The cup technique is a low-cost feeding strategy, which reduces weaning rates because it prevents nipple confusion that may lead to early weaning.41,42
The high loss to follow-up was a limitation of the present study. Greater losses occurred due to the COVID-19 pandemic, despite the use of strategies to maintain data collection, such as telephone communication with parents and optimization of children recruitment in the final stage of the study for individualized care, following the rules for using masks, hand hygiene, and controlling crowds. Survival analysis was a methodological strategy that minimized the loss of data on breastfeeding time and was able to show that the biggest drop in breastfeeding occurs from 4 months onward and then stabilizes at 10 months, but the CMA group had twice as many breastfed children as the SC group.
The advantages of this study include the homogeneity in socioeconomic level between the groups evaluated, the inclusion of control groups for comparison with children with CMA, and the performance of the oral provocation test to confirm the diagnosis of CMA.
Conclusions
Children with mainly nonallergic gastrointestinal complaints but also those with CMA were weaned earlier compared with asymptomatic children. The main reasons cited for weaning from the maternal perspective in the CMA group include the cow’s milk elimination diet, breast engorgement, and allergic reactions presented by the child. The use of a cup to supplement BM was the main factor associated with longer breastfeeding duration in the entire group of infants evaluated, regardless of socioeconomic level and the presence or absence of gastrointestinal symptoms.
Footnotes
Authors’ Contributions
T.G.M.: Conceptualization, data curation, investigation, methodology, project administration, resources, supervision, visualization, writing—original draft preparation, and writing—review and editing. A.J.B.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, supervision, and writing—review and editing. J.M.F. and S.C.F.V.: Conceptualization, investigation, resources, and writing—review and editing. B.F.P.: Conceptualization, investigation, and resources. D.d.S., S.A.d.S., and P.M.d.S.O.: Conceptualization and investigation. I.D.d.C.B.: Conceptualization and formal analysis. R.Q.G.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, supervision, and writing—review and editing.
Disclosure Statement
The authors have no financial conflicts of interest.
Funding Information
The financial support was received from Programa de Pesquisa para o SUS (PPSUS)/Fundação de Apoio à Pesquisa e à Inovação Tecnológica do Estado de Sergipe (FAPITEC/SE, Brazil).