
Abstract
Background:
The aim was to examine the associations between breastfeeding intensity and changes in concentrations of mammary gland involution markers (protein and lactose) among mothers participating in federal food assistance programs.
Methods:
Pregnant women in their third trimester who planned to breastfeed were recruited from local prenatal clinics (n = 25). After delivery, six weekly home visits were conducted to collect human milk samples and 24-hour infant feeding recalls. Milk protein and lactose concentrations were measured utilizing Bicinchoninic Acid and Megazyme assays, respectively. Bivariate tests were carried out using a statistical significance of p < 0.05.
Results:
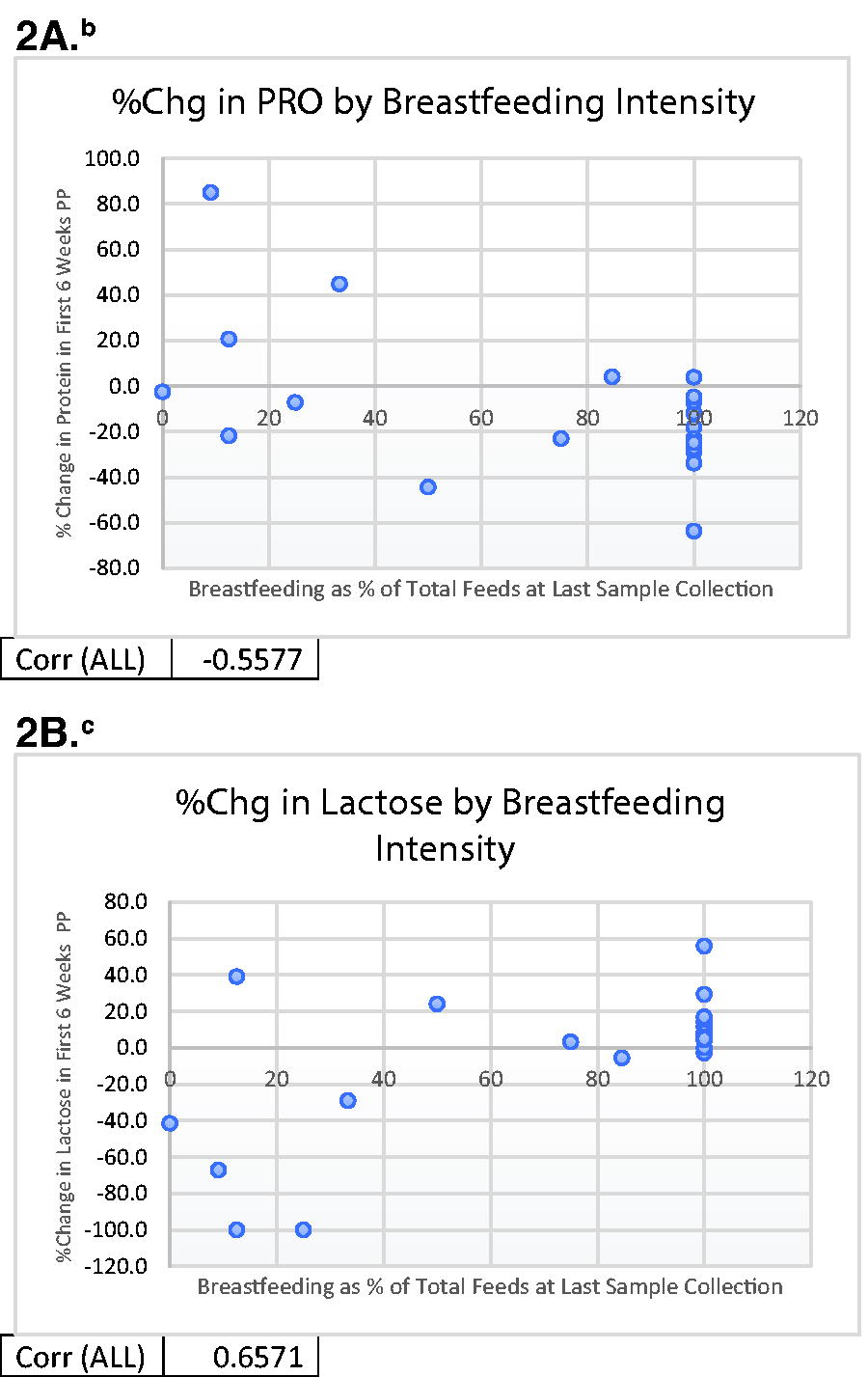
Majority (84%) of our participants were either African American or of Latino origin. About one-fourth of our participants were primiparous and the average monthly household income was $3,150 with an average household size of 4. In week 2 postpartum, 18 mothers had a 100% breastfeeding intensity, while in week 6 it decreased to 16 mothers. A significant difference in milk protein concentration was seen between exclusive and mixed-feeding mothers from weeks 2 to 6; meanwhile, for lactose concentrations, the significant differences were seen only in weeks 3 and 4 (p < 0.005). Protein changes were negatively associated with breastfeeding intensity (as breastfeeding intensity went up, protein decreased), while lactose changes were positively associated with breastfeeding intensity (protein r = −0.5578; lactose r = 0.6571).
Conclusions:
Significant associations between intensity of breast milk feeding and mammary gland involution markers highlight the sensitivity of the mammary gland to mixed feedings in the early postpartum period.
Introduction
Significant disparities in breastfeeding rates by income level exist in the United States. 1 Mothers who are living in poverty are less likely to breastfeed than mothers with higher incomes. 2 Lower rates of breastfeeding are associated with increased risks for infant premature death and poor health outcomes. 3 Exclusive breastfeeding is known to enhance infant cognitive development and help prevent lung and gut infections.4,5 Due to these benefits, the World Health Organization recommends exclusive breastfeeding until an infant reaches 6 months of age and incorporating breast milk into their diet until the age of 2 years old. 5 Increasing rates of breastfeeding have been endorsed as an important strategy to reduce health care costs and reduce obesity risk for both infants and mothers.6,7
The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) was established to aid pregnant and postpartum women, infants, and children at nutritional risk and living in low-income households (<185% federal poverty line). 8 About 50% of U.S. infants (1.5 million) receive WIC benefits, and African American and Latino infants constitute about 50% of program participants. 9 WIC offers three food assistance options for mothers and infants for the first 6 months: only formula feeding, mixed feeding, and exclusive breastfeeding. To improve and support breastfeeding, WIC revised food assistance in 2009 and increased food benefits for the exclusive breastfeeding package. 10 Nonetheless, exclusivity and continuation of breastfeeding remain a challenge among WIC participants. 8 One of the key obstacles to meeting breastfeeding goals has been an introduction to commercial infant formula during the neonatal period. A systematic review and meta-analysis indicate that avoidance of formula feeding in the first week is associated with longer breastfeeding duration and high likelihood of continuation of exclusive breastfeeding for up to 3 months. 11 The 2009–2015 National Immunization Survey indicated that this early formula supplementation is a common practice, with approximately one-fourth of infants in the United States being introduced to formula during their hospital stay or within the first couple of days after birth. 12
Early supplementation of formula (e.g., mixed feeding of breast milk and formula) may interrupt the supply-demand cycle necessary to establish lactation and may contribute to the early cessation of breastfeeding. The mammary gland begins to involute—the process of returning to the nonmilk-making state—as the frequency of breast stimulation declines. Involution is marked by changes in milk composition including an increase in protein and sodium and a decrease in lactose. 13 Whether the mixed breastfeeding practices during the early postpartum period are associated with changes in mammary gland involution markers remains to be explored. With the goal of gaining an understanding of the relationship between breastfeeding intensity in the first few weeks postpartum and continuation of breastfeeding, the objective of the study was to examine associations between breastfeeding intensity and changes in concentrations of mammary gland involution markers (protein and lactose) among a racially and ethnically diverse group of mothers participating in federal food assistance programs. We hypothesized that mixed feeding would be associated with alterations in longitudinal protein and lactose kinetics in breast milk compared with those seen during exclusive breastfeeding, reflecting biological changes in the mammary gland related to involution.
Methods
We conducted a longitudinal, observational study that collected weekly infant feeding practices and weekly breast milk samples during the first 6 weeks postpartum. This study was approved by the Institutional Review Board of UNC Greensboro. Potential participants were pregnant women recruited between November 2022 and May 2023 from two local prenatal clinics.
Eligibility criteria were as follows: participating in federal food assistance programs such as WIC or Supplemental Nutrition Assistance Program (SNAP); fluent in English or Spanish; 18 years or older; expecting a singleton pregnancy; intending to breastfeed for more than 2 months; and lacking any health conditions likely to affect milk production, such as gestational diabetes, hypertension, thyroid disorders, or polycystic ovary syndrome.
Based on the clinic’s daily appointment schedule, women in their third trimester were approached in the clinic’s waiting room by trained bilingual research assistants who provided study information. Recruitment in the third trimester was chosen to prevent an extended period between recruitment and delivery and reduce the burden of maintaining contact with participants.
Potential participants were informed that the study participation involved six weekly home visits after birth for interviews, and collection of breast milk samples. Upon indication of interest and initial confirmation of eligibility, mothers were asked to provide written consent for study participation. Women were also asked to sign a Health Insurance Portability and Accountability Act form to allow us to track their delivery date through medical records and contact them to set up postpartum home visits. These forms were available in both English and Spanish. Following enrollment, a brief interview was conducted to collect sociodemographic information, including maternal age, education, race/ethnicity, household size, and income.
Mothers were contacted by phone to set up the first home visit within 4 or 5 days after birth. If this was not feasible, a home visit 8–14 days after birth was scheduled. Home visits were conducted weekly for up to 6 weeks after birth. Each home visit was carried out between 8 and 9 a.m. to collect breast milk samples and conduct 24-hour infant feeding recalls, which estimated the frequency of breast milk (direct or expressed) and formula feeding in the past 24 hours. Participants were given grocery store gift cards after completing all home visits starting from week 1 or week 2 after birth.
Bilingual research assistants were trained in study procedures, including milk collection and 24-hour feeding recalls, using workshops, practice sessions, and simulation exercises. Training continued until they achieved >95% reliability in conducting all study procedures.
Measures
Milk collection
Each week, a 5 mL breast milk sample was collected. A breast opposite to the mother’s dominant hand was selected for milk collection. Two hours prior to the scheduled home visit, participants were instructed to avoid using the sample breast until the milk sample was collected. Participants were reminded that they could offer the other breast to feed the baby during the 2-hour window. At the time of milk collection, participants were asked to either pump the foremilk for 2.5 minutes or offer the sample breast to the infant and record the time once the infant begins swallowing actively. At the end of the 2.5 minutes, the mother was instructed to remove the infant from that breast, continue feeding from the other breast, and express 5 mL of milk (either manually or with a breast pump). The research assistant then transferred the milk to a sterile container and placed it in ice in a cooler for transportation to the lab. At the lab, samples were aliquoted in volumes ranging from 0.5 to 1.1 mL and stored in a −80°C freezer for future analysis.
Protein concentration measurement
Protein was measured using a PierceTM Bicinchoninic Acid kit (P/N P123225, Fisher Scientific, Waltham, MA) and spectrophotometry. This method is reliable for measuring protein compared with Kjeldahl as a reference method (R2 = 0.99), though protein is over-reported by approximately 0.3 g/dL. 14 Milk samples were diluted 1:40 with deionized (DI) water, and bovine serum albumin served as the standard. A 96-well plate was loaded with 25 µL of standards and diluted milk samples. Overall, 200 µL of working reagent was added to plate and gently agitated for 30 seconds and then incubated for 30 minutes at 35–37°C, before being placed on ice to cool for 10 minutes. Immediately after cooling, the plate was read at 562 nm using Bio-Tek Synergy 96 well plate reader (Agilent, Santa Clara, CA). All samples were run in triplicates and coefficients of variation (CV) were reported.
Lactose concentration measurement
Lactose was measured using a Megazyme enzymatic assay (P/N K-LACGAR, Megazyme International, Bray, Ireland) that has been validated as being accurate and reliable for measuring lactose in human milk. 15 Samples were first prepped to a 1:100 dilution using Carrez I (P/N SC9101500, Fisher Scientific) and Carrez II (P/N SC912500, Fisher Scientific) to remove protein and fat, which can interfere with the assay. Diluted samples were filtered using a Whatman #1 filter (P/N 09-920-115). Samples were run in duplicate per the manufacturer’s instructions and lactose-monohydrate (P/N 64044-51-5, Fisher Scientific) served as the standard.
Milk-feeding status and intensity of breast milk feeding
During the weekly home visits, 24-hour feeding recalls were conducted using the Nutrition Data System for Research software version 2020 (Nutrition Coordinating Center, University of Minnesota, Minneapolis, MN). The multiple-pass method was used to do the recall. In the first pass, mothers were asked to report the time of each feed from midnight to midnight of the previous day. In the second pass, these times were read aloud so mothers could revise information as needed. In the third pass, mothers noted whether the feeding was direct breastfeeding, expressed breast milk, or formula. Based on this information, milk-feeding status was determined for each week (i.e., exclusive breastfeeding, mixed feeding, fully formula feeding). If mothers were breastfeeding, the intensity of breast milk feeding was calculated as the number of breast milk feedings divided by the total feedings in the past 24 hours. Both direct breastfeeding and expressed milk were counted in calculation of milk-feeding status and intensity. For example, a feeding recall that identified 10 feedings the prior day, with 5 feedings of breast milk (direct at the breast or expressed milk), would have an intensity of breast milk feeding equal to 0.5 (5/10), while a recall that had 10 total feedings with all 10 using breast milk would have an intensity of 1 (10/10).
Statistical analyses
The analyses followed a prespecified statistical plan and were performed using BM SPSS Statistics for Windows (Version 28.0). Descriptive statistics were used to examine sociodemographic characteristics and milk-feeding status for each week. The association between milk-feeding status at week 2 and week 6 was tested using chi-square test. Protein and lactose concentrations in milk were plotted by milk feeding status (exclusive breastfeeding versus mixed feeding) and compared using t-test. Pearson correlation was conducted to examine the relationship between changes in milk protein and lactose concentrations over the study duration and the intensity of breastfeeding. Changes in protein and lactose were computed as (concentration of last milk sample collected—concentration of first sample collected)/concentration of first sample collected. Thus, a negative percent change would mean the milk concentration had decreased, while a positive percent change would mean the milk concentration had increased between the first and the last sample collection. We chose to report involution marker changes as percentages instead of as absolute changes because of the high interindividual variability in many compounds in human milk. 16 Statistical significance was considered marginal at p < 0.10 and significant at p < 0.05.
Results
Of the total 25 participants, 17 completed 6 home visits starting from week 1 after birth, while the remaining participants started home visits from week 2 after birth. Table 1 shows the demographic characteristics of the sample. Majority (84%) of our participants were either African American or of Latino origin. The mean monthly income of participants was $3,150.00 with an average household size of 4. Most participants had a vaginal delivery. A majority of our participants were enrolled in the WIC (84%), and over half (60%) were enrolled in SNAP.
Sociodemographic Characteristics of Mother–Infant Dyads (n = 25)
21 out of 25 participants reported monthly household income estimate. Those who did not know their monthly household income, did not report an estimate.
17 of 25 mothers participated in home visits for milk collection, recall, and interview from week 1 (i.e., within 7 days after delivery or 4 or 5 days after hospital discharge), while remaining started from week 2.
WIC, Special Supplemental Nutrition Program for Women, Infants, and Children; SNAP, Supplemental Nutrition Assistance Program.
As shown in Figure 1, in week 2 after birth, 18 out of 25 mothers were exclusively breastfeeding (e.g., breastfeeding intensity of 100%). At week 6, the number of participants exclusively breastfeeding had decreased to 16. The number of mothers doing predominant (e.g., breastfeeding intensity of 50–99%) to partial (e.g., breastfeeding intensity of 1–49%) breastfeeding went from six participants at week 2 to five participants at week 6. Meanwhile, mothers exclusively formula feeding (e.g., breastfeeding intensity of 0%) their infants increased from 1 at week 2 to 4 at week 6.
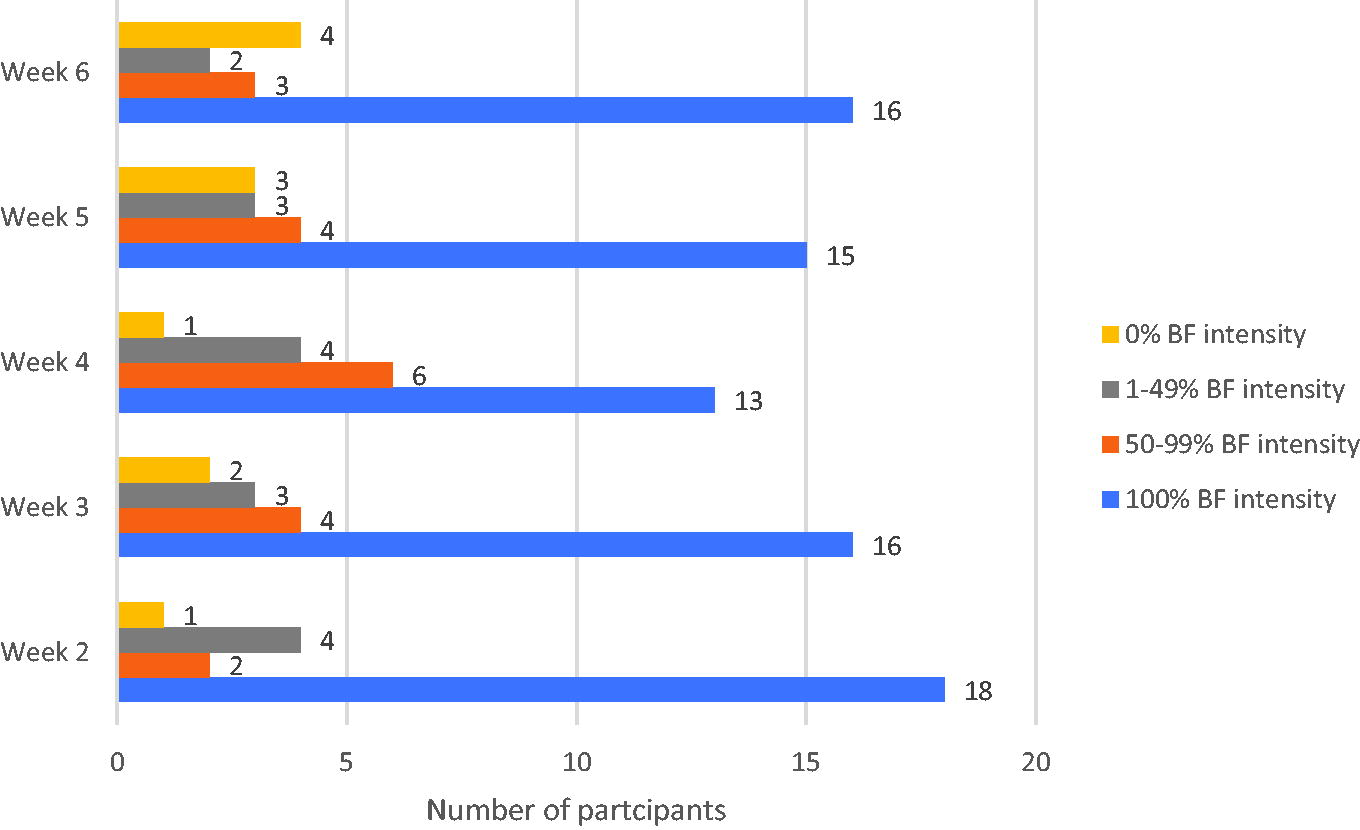
Breastfeeding intensity status and changes from weeks 2 to 6 among participants (n = 25). aBreastfeeding (BF) intensity was determined by conducted 24-hour feeding recalls. Participants with a 100% BF intensity were exclusively feeding their infant only breast milk. Exclusive refers to exclusive breast milk feeding either direct or expressed. Mixed feeding was practiced among participants with a BF intensity from 1% to 99%. A 0% BF intensity indicated only formula feeding. Week 2 was utilized as a starting point since multiple participants skipped the week 1 visit, while all 25 participants had completed a week 2 visit.
A total of 124 milk samples were included in this analysis with 12 participants providing 6 samples, 7 participants having 5 samples, 2 participants providing 4 samples, 1 participant having 3 samples, and 3 participants providing 2 samples. The average CV for replicate protein measurements was 3.4% and the average CV for replicate lactose measures was 2.6%. In comparing differences in involution markers, significant differences in breast milk protein concentrations by milk-feeding status were found (Table 2). Protein concentrations were significantly lower in milk samples of exclusively breastfeeding mothers at most time points starting from week 2 to week 6 after birth compared with participants practicing mixed feeding. In case of lactose concentration in milk samples, lower concentration was seen in mixed feeding. In weeks 3 and 4, lactose concentrations were significantly lower in milk samples of mothers who were doing mixed feeding.
Differences in Protein and Lactose Concentrations in Breast Milk Sample by Milk-Feeding Status in the First 6 Weeks Postpartum After Birth a
t-Test.
Data represent mean + standard deviation (# of samples).
p < 0.05 when comparing exclusive breastfeeding to mixed feeding at each time point.
BF, breastfeeding.
When comparing breastfeeding intensity at the last study visit to the percent change in milk composition between the first and last milk sample collection, we found a significant negative correlation between breastfeeding intensity and the rate of protein change (r = −0.5578, p = 0.0038, Fig. 2A), and a significant positive correlation with rate of lactose change (r = 0.6571, p < 0.001, Fig. 2B). These findings suggest that a high intensity of breastfeeding was associated with greater decreases in protein and greater increases in lactose longitudinally within a subject. Or conversely, a low breastfeeding intensity (e.g., more mixed feeding) was associated with lesser decreases in protein and lesser increases in lactose longitudinally within a subject.
(
Discussion
Our study indicates that initiating mixed feeding or formula supplementation in early postpartum is common and it is associated with breast milk composition changes similar to those seen in involuting mammary gland. 13 Specifically, lower breastfeeding intensity was associated with less decline in protein concentrations in the early postpartum period. This aligns with what has been previously reported by Hoban et al. among exclusively pumping mothers of preterm infants. The mothers who pumped less frequently and produced lower daily volumes of breast milk (<150 mL) had a less dramatic drop in protein concentration than the mothers who pumped more frequently and attained daily volumes >500 mL. 17
Our study demonstrates that mixed feeding in the first few weeks is associated with involution of the mammary gland assessed using common biomarkers, which may increase the risk for early breastfeeding cessation driven by decreasing milk production.
While we did not collect information on the reasons for mixed feeding, evidence suggests that the practice of feeding formula can be influenced by a combination of sociocultural and traditional beliefs, and environmental factors. In examining predictors of breastfeeding, it is noted that lower self-efficacy, distribution of formula during the hospital stay, and going back to work increase the risk for reduced intensity of breastfeeding. 18
Earlier discontinuation of breastfeeding is also associated with lack of access to breastfeeding support, cultural shame of breast exposure, and lack of breastfeeding information. 19 National level data indicates that about 19% of breastfed infants in the United States are supplemented with formula within the first 2 days after birth compared with the 28% we observed in our study. 20 A recent survey of 70% of U.S. hospitals providing maternity care noted that the two most common reasons for in-hospital formula supplementation included low self-efficacy and maternal requests/preference.20,21
Successful establishment of breastfeeding relies upon a complex biobehavioral orchestration involving secretory activation in the first few days postpartum accompanied by prompt initiation of breastfeeding after birth, and proper infant positioning and latching to achieve efficient milk removal and continued frequent nursing. Given this interactive nature of breastfeeding, optimal support and maternal health and well-being are critical for breastfeeding success. If emptying of the breast is partial or infrequent, milk accumulates in the ducts, and concentrations of protein increase in milk, signaling inhibition of milk production. Hence, high concentrations of protein in breast milk are often utilized as a marker of lactation cessation or mammary gland involution. 22 Our study results indicate that intensity of breastfeeding was significantly associated with milk production markers at all three stages of lactation; colostrum (week 1), transitional milk (weeks 2 and 3), and mature milk (weeks 4–6). Our findings have clearly demonstrated significant dose–response relationships between intensity of breast milk feeding and protein and lactose levels in milk. Compared with milk samples of exclusive breastfed mothers, milk samples of mixed-fed mothers had significantly higher protein content as early as in the second week postpartum. Our findings were akin to those of Dutta et al., though they studied the breast milk of mothers who delivered preterm. On average, the preterm infant mothers who exclusively breastfeed at 6 months had lower concentrations of protein and higher milk lactose content than mothers who introduced mixed feeding by 6 months. 22
While protein concentrations in breast milk are known to increase during mammary involution, lactose has been seen to have an opposite relationship. Lactose concentrations decrease fivefold during involution. 13 Similar to Nommsen et al. study, our study also found that mothers who had higher intensity of breastfeeding (exclusive breastfeeding) had a higher concentration of lactose. 23 Difference in lactose levels by breast milk feeding status, that is, exclusive versus mixed feeding, was statistically different in weeks 3 and 4. In weeks 1 and 2 or later during the mature milk phase (weeks 5 and 6), we did not see a significant difference in lactose concentration by milk-feeding status. Overall, lactose concentrations in breast milk have lower variation between women compared with other macronutrients. 24 On average, 6.4–7.6 g/dL of lactose concentration is seen in milk samples of full-term mothers. Colostrum is known to have the lowest amount of lactose, and then lactose concentrations stabilize in mature milk. 25 An earlier study found a lactose concentration mean of 5.6 g/dL on day 4 of lactation increasing up to 6.9 g/dL on day 120, which is similar to the range of lactose that we observed between 1 and 6 weeks postpartum. 26
Our study has some limitations. The study had a small sample size, hence differences in milk composition by maternal Body Mass Index (BMI), parity, and other characteristics such as stress were not assessed. Especially, in recent study, Ziomkiewicz et al. demonstrated low lactose concentrations in milk were associated with high psychosocial stress. 27 About one-third of our participants were already doing mixed feeding in week 1, but we did not collect information on reasons for mixed feeding. In the future, information on in-hospital practice, use of lactation services, and breastfeeding self-efficacy is warranted to fully understand what leads to mixed feeding and how changes in these predictors can help improve intensity and continuation of breastfeeding.
Conclusion
In summary, our study demonstrates dose–response relationship between intensity of breastfeeding and mammary gland involution markers during the early postpartum period in a population of low-income women. This indicates that a biobehavioral interrelationship exists between formula supplementation during early postpartum, and involution of mammary gland, potentially negatively affecting milk production and continuation of breastfeeding. A significant negative correlation in protein breast milk content and a significant positive correlation in milk lactose were found regarding intensity of breastfeeding. Future studies are needed to examine whether these changes in mammary gland involution markers continue past 6 weeks postpartum, and if they can be reversed through increasing breastfeeding intensity. This study promotes the need for further research on the relationships between early postpartum breastfeeding experiences, professional lactation and family support, maternal stress, and breastfeeding self-efficacy, to fully understand and develop tailored breastfeeding intervention for low-income households.
Footnotes
Acknowledgments
The authors would like to thank the prenatal clinical staff for their assistance in their participant recruitment and their study participants for their time.
Authors’ Contributions
J.M.D. was the principal investigator and coordinated study activities. M.P. coordinated lab analysis for milk composition. D.M.R. was involved in the data collection, assisted with the lab analysis, and wrote the first draft of article.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the NIH-NICHD grant (