
Abstract
Background:
Mothers of crying babies have difficulty adapting to their roles and problems with breastfeeding and attachment.
Objective:
This study aimed to assess the impact of the baby calming training provided to primiparous mothers on maternal role perception, maternal attachment, and breastfeeding self-efficacy.
Methods:
The study was conducted in a randomized controlled experimental design between March 2023 and March 2024 in the gynecology and obstetrics services of a public hospital in northeastern Turkey (Clinical Trial Number: NCT05594836). The research was conducted with a total of 84 primiparous mothers, including 41 intervention and 43 control groups, who met the inclusion criteria. The Baby Calming Training was administered face-to-face in the intervention group, utilizing a baby swaddling blanket, a sleep companion emitting white noise, and a training booklet. The control group received routine care. Data were collected through the Mother and Baby Introductory Information Form, Semantic Difference Scale—Me as a Mother, Maternal Attachment Inventory, Breastfeeding Self-Efficacy Scale-Short Form, and Infant Sleep Activity Record. The data were analyzed using descriptive statistics, Pearson’s chi-square test, independent samples t-test, Mann–Whitney U test, Wilcoxon test, mixed design ANOVA analysis, Cohen’s d, and 95% confidence interval (CI). This study adhered to CONSORT research guidelines.
Results:
Mothers in the intervention group exhibited higher mean scores on the perception of maternal role (mean ± SD: 70.37 ± 5.92, t: 8.590, 95% confidence interval [CI]: [1.347–2.375], d: 1.865, p < 0.001), maternal attachment (mean ± SD: 100.42 ± 1.52, U: 151.500, 95% CI: [0.732–0.892], d: 0.828, p < 0.001), and breastfeeding self-efficacy (mean ± SD: 64.00 ± 5.98, t: 8.109, 95% CI: [1.248–2.258], d: 1.757, p < 0.001) than the control group. It was determined that the total sleep time of the babies in the intervention group was higher, and the total crying duration was lower (p < 0.001).
Conclusion:
The study revealed that infant soothing training for primiparous mothers enhanced maternal role perception, maternal attachment, breastfeeding self-efficacy, and extended infants’ sleep duration. Furthermore, infants exhibited reduced crying.
Introduction
In the critical postpartum period, in which the newborn integrates with the family system, physical, emotional, and social changes occur in the life of a woman who becomes a mother for the first time, and she needs to acquire new roles in this respect. The addition of a baby to the family can be positive, satisfying, and strengthening for the family, but it can also be perceived as a crisis period for the family and the mother.1,2
Continuous crying of infants in the first 3 months following the delivery is among the health complaints that caregivers most frequently consult healthcare professionals. 3 Infants cry more following birth, reaching their highest level at about 5–6 weeks of age and reaching its peak at 8–9 weeks following birth, decreasing in the following 2 weeks. 4 When the literature was reviewed, it was found that mothers of constantly crying infants feel inadequate, their anxiety levels are high, and maternal attachment is negatively affected, and this may be a reason that triggers shaken baby syndrome.5,6 It was reported in a previous study that premature crying and sleep problems in infants may cause irregular attachment. 7 Also, mothers of infants who are difficult to calm have high levels of stress regarding the parenting role. Feedback from the baby, such as crying and insomnia, affects the mother’s self-efficacy negatively. 5
The stress and emotional intensity faced by primiparous mothers, as well as their efforts to adapt to their new roles, might affect the effective maintenance of breastfeeding and breastfeeding self-efficacy. 8 One of the effective calming methods preferred by mothers to comfort a crying baby is breastfeeding, but the crying of the infants causes mothers’ anxiety levels to increase. 9 In the postpartum period, depression and high anxiety levels of mothers are an important factor that affects breastfeeding negatively.10,11 Considering all these aspects, interventions to ensure that infants cry less should be implemented in the postpartum period.6,12
Developed as a method to calm infants, the “Five Basic Principles Method” is a calming practice that includes actions mimicking the conditions in the womb. 12 This method is applied by using the 5S (swaddling, side-stomach position, shushing, swinging, and sucking), which is an intervention that can calm infants’ restlessness and excessive crying, helping to prolong the baby’s sleeping time. In this technique, which can be applied by nurses and taught to parents through education, each step is applied gradually to crying infants. 13 When the literature was reviewed, it was found that the 5S technique taught to mothers in the postpartum period increased the self-efficacy levels of parents. 5 In another study, the 5S technique was used to calm infants’ crying, and it was reported that infants’ restlessness and heart rates decreased. 13 Studies were conducted to determine the effects of the 5S technique on infants’ crying and sleep.5,6,13 However, no studies were detected that evaluated maternal role, maternal attachment, and breastfeeding self-efficacy in this respect.
This study aimed to assess the impact of the baby calming training provided to primiparous mothers on maternal role perception, maternal attachment, and breastfeeding self-efficacy.
Research hypotheses
Baby calming training provided to primiparous mothers
a. Does not affect mothers’ perception of the maternal role, maternal attachment, and breastfeeding self-efficacy;
b. Has no effect on infants’ total sleep and crying times.
Baby calming training provided to primiparous mothers
a. Affects mothers’ perception of the maternal role, maternal attachment, and breastfeeding self-efficacy;
b. Affects infants’ total sleep and crying times.
Material and Methods
Design and setting
The study was conducted in a randomized controlled experimental design between March 2023 and March 2024 in the gynecology and obstetrics services of a public hospital in northeastern Turkey (Clinical Trial Number: NCT05594836). The hospital had a baby-friendly hospital certificate.
Sample size
The sample of the study was calculated by using the G*Power 3.1.9.7 program with two-way mixed ANOVA analysis, taking into account the study design with two groups (intervention group, control group) and two measurements (pretest, posttest). The results of Aluş Tokat and Okumuş’s study on breastfeeding self-efficacy were used to determine the effect size of the study. 14 In the calculation, the effect size was 0.20 (f = 0.20), 5% margin of error (α = 0.05), and 90% power (1−β = 0.90). The number of samples for each group was calculated as 40, and the study was planned to be conducted with 80 mothers. It was decided to collect the data from a total of 88 mothers (44 intervention, 44 control) by including a 10% backup sample in this number in case of possible data losses. This randomized clinical trial was based on the guidelines proposed by the Consolidated Standard of Reporting Trials-CONSORT 2017 (Fig. 1).
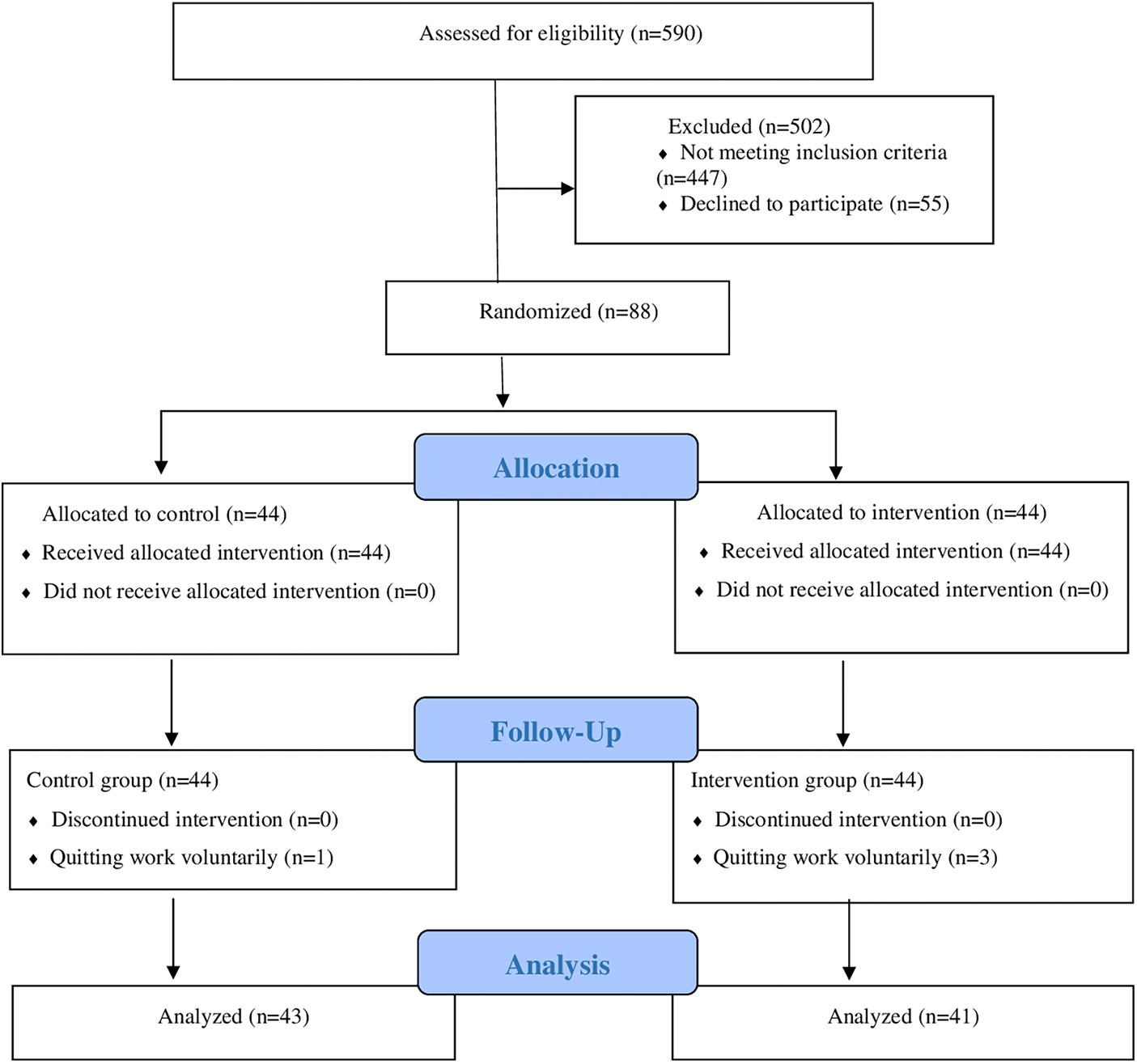
CONSORT flow diagram.
Randomization and blinding
Simple randomization of intervention and control groups was determined according to the recommendations given at the https://www.randomizer.org/ website. As the researcher was the person who actively implemented the intervention in the study, the researcher was excluded from blinding as the condition of blinding could not be met in the later stages. For this reason, participants in the intervention and control groups were blinded. All participants were told that training would be given by the researcher within the scope of the study, but the time of training was not disclosed.
Inclusion criteria
The inclusion criteria for the mothers were being primiparous, not having multiple pregnancies, not having a chronic disease that would prevent baby care, being over 18 years old, being within the first 24 hours following birth, being literate, and being open to communication and interaction. The criteria for infants were being older than the 37th week of gestation, being a naturally fed baby, and having a normal birth weight (between 2500 and 4000 g).
Exclusion criteria
The exclusion criteria for the infants were having a medical condition that might prevent breastfeeding.
Criteria for removal from the study
The criteria for the infants were having a disease diagnosed during the study period and having been admitted to the Neonatal Intensive Care Unit.
Data collection tools
Mother and baby introductory information form
In this form, which was prepared by researchers in line with the literature data,5,6,12,15,16 there were questions about the descriptive characteristics of the mother and the baby (age, place of residence, education level, family type, economic situation, working status, whether the pregnancy was planned or not, type of birth, week of birth of the baby, gender, who would assist the mother in the care of the baby, etc.).
Semantic difference scale—me as a mother
Walker et al. developed the scale to measure the dimensions of the concept of “me as a mother.” 17 The scale was adapted to Turkish society by Çalışır. 18 The scale consists of 11 items of opposite adjective pairs, which are distributed in 22 items. Each adjective pair is scored from 1 to 7. A high total score on the scale indicates a positive self-evaluation of motherhood. 17 The internal consistency coefficient of the scale was found to be between 0.81 and 0.85 by Walker and the Cronbach α internal consistency coefficient was found to be 0.73–0.74 by Çalışır. 18 The Cronbach α coefficient was found to be 0.78–0.90 in this study.
Maternal attachment inventory
The inventory was developed by Müller 19 to measure the attachment between the mother and the baby and was adapted to Turkish society by Kavlak and Şirin. 20 The scale has a 4-point Likert style consisting of 26 items. Each item is scored as 4 points (always) and 1 point (never). The lowest score that can be obtained from the scale is 26, and the highest score is 104. A high score indicates high maternal attachment. It is recommended to apply this scale twice, in the first and fourth months following the birth. In the original version of the scale, the Cronbach α coefficient in the 1st month was 0.85, and the Cronbach α coefficient in the fourth month was 0.76. 19 Kavlak and Şirin 20 determined the Cronbach α coefficient as 0.77 in the first month of its application and 0.82 in the fourth month. The scale was applied to mothers at 4 and 8 weeks postpartum, and the Cronbach α coefficient was found to be 0.77–0.83 in this study.
Breastfeeding self-efficacy scale-short form
The scale was developed by Dennis 21 and consists of 14 items. The Turkish validity and reliability study of the scale was conducted by Tokat et al. 22 Breastfeeding self-efficacy scale-short form (BSES-SF) is a 5-point Likert-type scale (1 = “I am not at all sure” and 5 = “I am always sure”). The minimum score that can be obtained from the scale is 14, and the maximum score is 70. The scale has no cut-off point, and a high score from the scale means that mothers have high breastfeeding self-efficacy. Cronbach’s α value of the scale was found to be 0.86. 22 The Cronbach α coefficient was found to be 0.93 (pretest) and 0.95 (posttest) in this study.
The infant sleep activity record
The infant sleep activity record (ISAR) was developed for the Nursing Child Assessment Satellite Training Program. 23 This form, which can be applied by the primary caregivers of infants, is filled out by recording the infants’ sleep, crying, and feeding activities for 1 week. Baby Sleep and Cry Diary consists of 12-hour sections, separate for day and night. Each hour unit is divided into four 15-minute intervals. Sleep is symbolized as “U” and crying as “A” in the diary. The baby’s behavior is recorded day and night. ISAR has been used previously in Turkiye and different countries.16,24
Intervention tool
Baby swaddling blanket
In applying baby calming training (5S technique), the first step is to swaddle the baby effectively and safely. For this purpose, a method developed by Karp (2015) and called “DUDU (Down-Up-Down-Up) technique” was used. 12
Sleeping companion emitting white noise
In the study, a material that was portable, suitable for use with infants, had an automatic shut-off timer (15, 30, and 60 minutes), had different white noise sounds, and could be easily used by parents. Mothers were trained to let their infants listen to whichever of these sounds calmed them down, and following the training, the materials were provided to the mothers to use at home.
Baby calming training booklet
The researcher received an educator certificate by participating in the online certification program “The Happiest Baby Educator Certification Program,” organized by the Happiest Baby Organization for the use of calming initiatives (5S). Baby Calming Training Booklet was prepared by researchers to calm crying infants, taking the book “The Happiest Baby on the Block” developed by Karp as a reference. 12 The opinions of 10 experts (lecturer, specialist nurse) were taken regarding the validity of the booklet in terms of information reliability (Kendall’s W a = 0.817, p = 0.000) and information quality (Kendall’s W a = 0.807, p = 0.000).
Procedure
Control group
No treatment was applied to the mothers in the control group other than the standard newborn care and breastfeeding training routinely given in the clinic. Pretest data were filled in with the Mother and Baby Information Form, Semantic Difference Scale—Me as a Mother, and BSES-SF face-to-face interview method at a time when the baby was sleeping and the mother felt well to primiparous mothers who were followed up in the gynecology ward in the postpartum period, and the Baby Information was given about when (week 4 and week 8) and how to fill out the Sleep and Cry Diary. Mothers were contacted by phone in the fourth week, the maternal attachment inventory (MAI) was filled out, and a reminder was provided to fill out the Baby Sleep and Cry Diary. At the end of the eighth week, the Semantic Difference Scale—Me as a Mother, BSES-SF, and MAI posttest data were administered to the mothers, and the Baby Sleep and Cry Diaries were received from the mothers.
Intervention group
Primiparous mothers who were followed up in the gynecology ward in the intervention group filled out the Mother and Baby Introductory Information Form, Semantic Difference Scale—Me as a Mother, and BSES-SF pretest data using face-to-face interview method at a time when the baby was sleeping and the mother was feeling well. Following the pretest, the first session of the Baby Calming Training, which lasted approximately 40 minutes, was implemented using face-to-face interview techniques and materials provided by the researcher (baby swaddling blanket, sensor sleep companion that provides white noise, and baby calming training booklet). The applications were first demonstrated and explained to the mother by the researcher, and then the mother was asked to apply all the steps and observed by the researcher. The educational tools used during the training were gifted to the mothers at the end of the training, and mothers were informed that the educational content should be applied at home as well. Then, the mothers were informed about how to fill out the Baby Sleep and Cry Diary.
Mothers were contacted through phones, and reminder training was provided, feedback was received on whether they had any difficulties with the application, and questions were answered in the fourth week following birth. Also, by filling out the MAI, a reminder was provided to fill out the Baby Sleep and Cry Diary. At the end of the eighth week, Semantic Difference Scale—Me as a Mother, BSES-SF, and MAI posttest data were collected from the mothers, and Baby Sleep and Cry Diaries were received from the mothers.
Data analysis
The data were sent to a statistician after being blindly coded (so the statistician would not know which participants belonged to the control and intervention groups). The data were analyzed with the SPSS for Windows 22 package program. Number, percentage, mean, standard deviation, and chi-square were used in the analysis of the data. The compliance of the data with the normality assumption was calculated with the “Kurtosis” and “Skewness” coefficients (±2). In comparing pairwise groups, the independent groups t-test was used for normally distributed data, and Mann–Whitney U test was used for non-normally distributed data. The t-test was used for dependent groups for normally distributed data in intragroup comparisons of binary groups, and Willcoxon analysis was used for non-normally distributed data. Mixed-order ANOVA analysis was used to compare the measurements according to groups. The Bonferroni correction was applied to compare the main effects in mixed-order ANOVA analyses. Cohen’s d and 95% confidence intervals (CIs) were used to evaluate the effect size, while partial eta squared was used for effect size, and p < 0.05 was considered statistically significant in the study.
Ethical principles
Ethical approval (29/09/2022 dated B.30.2.ATA.0.01.00/592 numbered) and official permission from the relevant institution were obtained to conduct the study. The purpose of the study was explained to the mothers who met the inclusion criteria, their questions were answered, and their verbal and written consent was obtained. Ethical principles were adhered to in the study.
Results
It was found that the intervention and control groups were distributed similarly in terms of the variables of mothers’ age, place of residence, educational status, family type, economic status, employment status, health problems during pregnancy, whether the pregnancy was planned, and the person who assisted baby care, and the infants’ gender and week of gestation (p > 0.05, Table 1).
The Inter-Group Comparison of the Descriptive Characteristics of the Mothers and Babies (n = 84)
The pretest BSES-SF mean score of the intervention group (52.10 ± 8.82) was higher than the pretest BSES-SF mean score of the control group (43.84 ± 10.08), and the difference between the groups was determined to be statistically significant with a high effect size (d = 0.871, p < 0.001). The posttest Semantic Difference Scale (70.37 ± 5.92), MAI (100.42 ± 1.52), and BSES-SF (64.00 ± 5.98) mean score of the intervention group was higher than the control group, and the difference between the groups was determined to be statistically significant with a high effect size (d = 1.865, p < 0.001; d = 0.828, p < 0.001; d = 1.757, p < 0.001, Table 2).
The Inter- and Intra-Group Comparison of the Mean Semantic Difference, Maternal Attachment, and Breastfeeding Self-Efficacy Scores of the Mothers in the Intervention and Control Groups (n = 84)
CI, confidence interval; d, Cohen’s d; η2, eta square; F, mixed pattern ANOVA; SD, standard deviation; t, independent groups t-test; t*, paired samples t-test; U, Mann Whitney U test; Z, Wilcoxon test.
When the intragroup comparison results were evaluated, the mean posttest Semantic Difference Scale, MAI, and BSES-SF scores in the intervention group were found to be higher than the pretest, and the intragroup difference was statistically significant with a high effect size (d = −1.721, p < 0.001; d = −1.284, p < 0.001; d = −1.428, p < 0.001). The difference between the pretest and posttest Semantic Difference Scale mean scores in the control group was statistically significant, similar to the intervention group, but the effect size of the difference was medium (d = −0.683, p < 0.001). The intragroup difference between the pretest and posttest BSES-SF mean score values in the control group was statistically significant with a high effect size (d = −0.958, p < 0.001, Table 2).
In the study, when the joint (group × time) effect of group and time on the Semantic Difference Scale (η2 = 0.347, p < 0.001) and MAI (η2 = 0.267, p < 0.001) score was examined, the group-time interaction had a statistically significant and high level of effect. When the common (group × time) effect on the BSES-SF score was examined, it was found that the group–time interaction had a statistically significant and moderate effect (η2 = 0.075, p = 0.012, Table 2).
The pretest total sleep times average of the intervention group (776.76 ± 40.90) was higher than the control group (691.64 ± 48.59), the pretest total crying times (101.60 ± 15.26) average was lower than the control group (123.29 ± 18.42), and the difference between the groups was statistically significant with a high effect size (d = 1.891, p < 0.001; d = −1.279, p < 0.001). It was also found that the posttest total sleep times average in the intervention group (614.37 ± 27.59) was higher than the control group (592.18 ± 24.36), and the difference between the groups was statistically significant with a medium effect size (d = 0.854, p < 0.001). Posttest total crying times in the intervention group (136.82 ± 13.74) were found to be lower than the control group (160.66 ± 15.72), and the difference between the groups was determined to be statistically significant with a high effect size (d = −1.611, p < 0.001, Table 3).
The Inter- and Intra-Group Comparison of the Mean Total Sleep and Crying Time Scores of the Babies (n = 84)
CI, confidence interval; d, Cohen’s d; η2, eta square; F, mixed pattern ANOVA; SD, standard deviation; t, independent groups t-test; t*, paired samples t-test.
When the intragroup comparison results were evaluated, it was found that the posttest total sleep times average in the intervention group was lower than the pretest, the total crying times were higher than the pretest, and the intragroup difference was statistically significant with a high-level effect size (d = 3.125, p < 0.001; d = −1.794, p < 0.001). In the control group, the intragroup difference between the pretest and posttest total sleep times and total crying times mean values were determined to be statistically significant with a high effect size (d = 1.844, p < 0.001; d = −1.474, p < 0.001, Table 3).
It was also found that the group–time interaction on total sleep time had a statistically significant and high level of effect (η2 = 0.265, p < 0.001), and the group–time interaction on total crying time was statistically similar (F = 0.145, p = 0.704, Table 3).
Discussion
Based on the findings of the present study, it was found that the baby calming training provided to primiparous mothers increased their perception of the maternal role, maternal attachment, and breastfeeding self-efficacy. These findings confirm the H1a hypothesis.
In the literature, the number of studies conducted on the perception of the maternal role of baby calming training provided to primiparous mothers is limited. 5 It was found that the education and counseling services provided to primiparous mothers in the postpartum period increase the perception of the maternal role and facilitate the mother’s adaptation to the new role. 2 In Botha et al.’s 5 study, mothers were given behavioral baby calming training, and it was found that the parental self-efficacy of the mothers in the training group improved significantly. Studies reported that improving mothers’ self-efficacy can also increase their maternal role competence.25,26 The results of the present study are similar to the results of other studies in the literature, and it can be argued that the educational interventions provided to primiparous mothers following birth are an effective initiative to increase the maternal role.
When studies evaluating the maternal attachment of primiparous mothers were evaluated, evidence was found that mothers experiencing motherhood for the first time avoid contact with their infants, feel unprepared for baby care15,27 and that these situations can be strengthened with educational programs and kangaroo mother care.15,28,29 In a study, face-to-face health promotion training was provided to mothers, and at the end of the training, maternal attachment was found to be higher in the experimental group. 30 The results of the present study are similar to the results of other studies in the literature, and it can be argued that educational interventions provided to primiparous mothers following birth are an effective intervention in increasing maternal attachment.
Aktaş and Küçük Alemdar reported that baby crying is an important factor that reduces mothers’ breastfeeding self-efficacy and breastfeeding success. 31 A study reported that mothers who were less disturbed by their baby’s behaviors had higher breastfeeding self-efficacy. 32 Brockway et al. 33 found that interventions for breastfeeding self-efficacy were effective in increasing postpartum mothers’ breastfeeding self-efficacy. The importance of integrating educational interventions to promote breastfeeding into postpartum care and randomized controlled studies has been emphasized in the literature.34,35 In the present study, the findings, which support the literature data, show that the training program provided to mothers in the postpartum period is extremely important and that the breastfeeding self-efficacy of primiparous mothers who are inexperienced in baby soothing can be increased with this training. Also, it was considered in this study that there was an increase in the breastfeeding self-efficacy of the mothers in the control group, and this may be because of the provision of breastfeeding education to all mothers in the postpartum period in routine care.
In the present study, it was found that baby calming training provided to primiparous mothers increased the total sleep times of the infants and decreased the total crying times. These findings confirm the H1b hypothesis.
In their study, Sweeney et al. applied behavioral–educational sleep intervention to primiparous mothers following birth and found that the sleep duration and quality of the infants increased. 36 In another study, baby calming training, including the 5S technique, was applied face to face to mothers with healthy infants, and it was found that there was an increase in the total sleep times of the infants in the intervention group. 16 The results of the present study are similar to those in the literature, suggesting that baby calming training provided to parents is effective in increasing infants’ total sleep times.
The difference between studies reporting that interventions for infants reduce crying and the present study is the use of one or more of the interventions related to the 5S technique37,38 and the use of 5S interventions by healthcare staff during an invasive procedure.39–41 When the literature was reviewed, evidence was found that the 5S technique reduces crying times during invasive interventions.13,40
In a previous study, the 5S technique was applied by the parents of infants under 6 months of age to calm them, and it was found that crying decreased. 42 In a study that was conducted on primiparous mothers, various behavioral interventions, including the 5S technique, were taught to mothers, and it was found that these positively affected crying. 43 In another study, baby calming training was given, and parents were asked to keep a diary regarding their baby’s sleep, crying, and feeding, and it was found that the infants in the intervention group cried less. 16 These results are similar to the findings of the present study. Also, the study results are similar in that they are based on mothers’ reports. In the present study, unlike this study, the mother was given baby calming training in the early postpartum period, and the mothers’ practices at home were tried to be supported by using materials appropriate to the content of the training.
Limitations
The limitation of the study was that it was conducted in one single city in the northeast of Turkiye. Also, the fact that the training was administered by the researcher in the intervention group and the researcher could not be blinded during the intervention was another limitation of the study.
Conclusion
It was found that the 5S technique, which is taught to primiparous mothers to calm their infants, increased the mothers’ perception of the maternal role, maternal attachment levels, and breastfeeding self-efficacy, extended the infants’ sleep times, and reduced the crying times. The intervention used in this study demonstrated positive effects on maternal and infant health outcomes. Nurses can benefit from this intervention to support maternal and infant well-being in the postpartum period and reduce hospital admissions due to crying. It is also thought that this intervention can be used in primary health care.
Footnotes
Acknowledgments
The authors would like to thank all the babies and their precious mothers participating in the research.
Authors’ Contributions
G.A..: Conceptualization, formal analysis, methodology, data curation, supervision, and writing—original draft. A.S.: Conceptualization, methodology, project administration, data curation, supervision, and writing—review and editing.
Ethical Considerations
This study received B.30.2.ATA.0.01.00/592 numbered approval dated 29/09/2022 from Atatürk University Faculty of Medical Clinical Research Ethics Committee. All participants were informed, and each provided written informed consent.
The clinical trial registration number is NCT05594836.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This work was supported by the Atatürk University Scientific Research Projects [