
Abstract
Aims:
This study aimed to analyze and compare the quantity of energy and fat using the infrared analysis and creamatocrit method in pasteurized human milk (HM) samples.
Methods:
This cross-sectional study analyzed 1,858 pasteurized human samples from 317 mothers at a single center. Infrared transmission spectrophotometry (Miris, Human Milk Analyser [HMA], Uppsala, Sweden) and the creamatocrit method were used to evaluate the quantity of energy and fat in pasteurized HM samples.
Results:
The average age of donor mothers was 29.7 ± 5.1 years, and the median duration of lactation was 22 days (interquartile range [IQ]: 7.7–59.2). Full-term births were observed in 196 (95.1%) of the women. The values of energy (difference: +8.96 kcal/dL, 95% CI: 8.52–9.44 kcal/dL; p < 0.001) and fat (difference: +0.40 g/dL, 95% CI: 0.35–0.45 g/dL; p < 0.001) in HM samples obtained by Miris were higher than those by the creamatocrit method. The energy calculated and the fat measured by Miris in the HM samples correlated moderately and directly with the obtained by creamatocrit (fat, r = 0.585; p < 0.001 and energy, r = 0.591; p < 0.01). The linear regression, adjusted for maternal age and lactation time, showed that the energy values calculated by creamatocrit were directly associated with those of Miris (energy kcal/dL = 38.43 + [0.516 × kcal/dL of creamatocrit]).
Conclusion:
The energy and fat quantity of pasteurized HM samples obtained by the creamatocrit and infrared methods were significantly correlated. However, the values calculated by the creamatocrit method were significantly lower than those by the infrared analyzer.
Introduction
Advances in perinatal care have significantly reduced early infant mortality. However, premature birth still occurs with a high frequency worldwide. 1 In Brazil, approximately 10–12.5% of children are born preterm, and a quarter of these children are born at less than 33 weeks. 2
There are many challenges in treating preterm newborns (PTNBs), including the immaturity of organs and systems, prolonged hospitalization, diseases associated with prematurity, and the use of invasive procedures to maintain life, such as ventilatory support, intravenous therapy, antibiotic therapy, and phototherapy. In addition to reducing mortality, short- and long-term morbidities can be decreased by adjusting the treatment of these neonates during their period of hospitalization. These advances are related to promoting adequate physical growth and neuropsychomotor development and reducing the risk of chronic noncommunicable diseases throughout life.1–3
Human milk (HM) in nutritional therapy for PTNBs represents one of the main protective factors against complications in these infants.4,5 Recent publications have confirmed that infants who receive HM in the neonatal unit have a lower risk of developing necrotizing enterocolitis and sepsis. 4 After hospital discharge, the advantages of breastfeeding remain, especially in neuropsychomotor, pulmonary, and bone development. 5 In adulthood, there is a reduced risk of hypertension and dyslipidemia.6,7
Preterm infants take longer to develop the ability to suck and swallow entirely, so there is often a need to feed them through tubes. At this stage, the preferred food is the mother’s milk, and if this is not possible, pasteurized HM or a donor can be used.8,9
The composition of breast milk is highly variable, changing with each lactation period and from one feed to the next. Factors such as gestational age, nutritional status, diseases, and maternal diet can influence its composition, especially the distribution of energy and macronutrients.10–12
The creamatocrit technique estimates HM’s energy value based on fat quantification. Despite its practicality and low cost, this calculation needs to consider the amount of protein and carbohydrate in the samples. 10 Today, more accurate methods are available for calculating energy and macronutrients in small samples of HM. However, the equipment used for this measurement is expensive, requires frequent maintenance, and needs to be more practical for inclusion in the HM bank (HMB) routine. On the contrary, better knowledge of pasteurized HM composition can help plan nutritional therapy for PTNBs, including reducing the risk of inadequate use of infant formula.13,14
Because of the relevance of HMB in enabling the use of HM for hospitalized PTNBs who cannot receive mother’s milk exclusively, it is essential to know more about its composition, especially regarding the amount of macronutrients. This study aimed to analyze and compare the energy and fat content in pasteurized HM samples using the infrared analysis and creamatocrit method.
Materials and Methods
Study design
A cross-sectional study analyzed 1,858 samples of pasteurized HM from 317 donor mothers at the HMB of the Hospital da Mulher de São Bernardo do Campo-HM-SBC, São Paulo, Brazil, from January 2022 to December 2023.
HM-SBC has an HMB that follows the quality standards recommended by the National HMB Network10, from donor collection to dispensing HM to newborns in raw or pasteurized HM. The HMB is also a source of information on breastfeeding and receives nurses who are hospitalized or with their children at home.
The study included healthy, single-pregnancy mothers who were breastfeeding their own child born at term or preterm, who had exceeded breast milk and contacted the HMB in person, by telephone, or by text messages to donate breast milk. During the interview, a previously trained health professional from the HMB carried out a standardized questionnaire and applied the informed consent form at the first personal contact with the women.
To be included in the study, the mothers had to have prenatal and postnatal tests compatible with HM donation (blood count and negative serologies—VDRL, HIV, HTLV 1 and 2, and hepatitis B and hepatitis C) and agree to participate. Mothers who smoked (more than ten cigarettes a day), those who used substances of abuse (cocaine, heroin, amphetamines, crack, and cannabis), those receiving medication incompatible with breastfeeding, and those with diseases that absolutely or relatively contraindicated breastfeeding were excluded10. The HM samples were collected, stored, and analyzed using the procedures recommended by the HMB technical standards. 10
This project was approved by the Research Ethics Committee of the Centro Universitario FMABC (number 5.219.965, CAAE: 54657221.4.0000.0082). The procedures were explained to the nursing mothers, who signed an informed consent form to participate in the study. This article was organized according to the CONSORT guidelines.
Outcomes
The amount of energy was calculated, and the fat was measured in pasteurized HM samples using an infrared transmission spectrophotometry analytical instrument (Miris, Human Milk Analyser [HMA], Uppsala, Sweden) and the creamatocrit method.
Collection and processing of breast milk
A questionnaire was applied to nursing mothers at home or at the HMB. This survey contains information on maternal age and health, prenatal care, tests carried out, gestational age, lactation period, place of birth, child sex, and type of delivery.
The mother carried out manual or mechanical breast milk extraction at the HMB or at home after guidance from the HMB professional. The donor has dressed appropriately, and after hand hygiene, she began a circular massage of the breasts, discarded the first jets, and proceeded to extract and store the milk in a glass jar with a plastic lid previously sterilized and supplied by the HMB. After collection, the date and time were recorded on the glass jar and immediately placed in a freezer at the HMB or home. The HM remained frozen (−3°C) for 15 days from the first collection. 10 For home collection, the HMB sent a car or motorbike to collect the glass jar from the nursing donors.
The glass jars with HM were visually analyzed to detect the presence of contaminants. They were then analyzed by determining the Dornic acidity, which consists of assessing the HM via two reagents, sodium hydroxide and phenolphthalein. 10 According to the parameters defined, acidity values between 1.0°D and 8.0°D were considered normal. All glass jars that did not meet the selection, classification, and physicochemical analysis requirements were discarded.
The evaluated and approved HM was sent for pasteurization, 10 which involves heating the HM to 62.5°C for 30 minutes. This inactivates 100% of the pathogenic microorganisms likely to be present in the samples and 99.99% of the saprophytic or normal microbiota. After the pasteurization process, an aliquot of 10 mL was separated from each glass jar for analysis of the macronutrient content. 10
Analyzing energy value and fat quantity
Infrared transmission spectrophotometry analytical instrument (Miris)
The MIRIS method was carried out in four stages. 15 The first stage involved sanitizing the equipment’s two cuvettes, into which a specific MIRIS cleaning solution was injected (2 mL twice). In the second stage, the cuvettes were washed with 5 mL of deionized water (the wash was repeated five times). The third stage was calibration, in which 3 mL of Miris test solution was injected into the cuvettes, leaving 0.5 mL in the syringe to prevent air from entering the analysis equipment. In the fourth stage, the energy and fat values of the samples were evaluated.
To do this, 3 mL of HM was aspirated from the tube containing pasteurized HM, which was first homogenized (Miris Ultrasonic Processor) and then injected into the dosing cuvettes. The cleaning and calibration solutions used in the procedures were kept at 38°C to 40°C. The results were released on the device’s digital screen within 60 seconds. The amount of energy was expressed in kilocalories (kcal) and fat in grams (g).
Creamatocrit technique
Determination of the creamatocrit was carried out at the HMB according to the recommendations. 10 The human milk (LH) samples were divided (0.5 mL each) into three 0.75 × 1.5 mm glass capillaries, which were immediately centrifuged at 11,500 rpm for 15 minutes (FANEM® model 2410 centrifuge). After centrifugation, the HM was separated into liquid and fat (cream). The heights of the total column and the cream of each capillary were measured via a millimeter caliper, and the value of the cream was used in a standard formula to estimate the energy density. Two formulas were used to calculate the energy and measure fat values. 10
Cream content: Cream column (mm) × 100 ÷ Total column (mm) = Cream %.
Fat content (% cream-0.59) ÷ 1.46 = % fat
Total energy content (% cream × 66.8 + 290) = kcal/L
Statistical analysis
The data were tabulated, consolidated in an Excel® spreadsheet, and analyzed via the SPSS 29.0 statistical package (IBM). Categorical variables are presented as absolute numbers and percentages, and the chi-square test compares them. Continuous variables were tested for distribution via the Shapiro–Wilk test, kurtosis values, and histograms. Those with a normal distribution were compared via Student’s t-test, and those with a nonparametric distribution were compared via the Mann–Whitney test. Pearson’s correlation was used to assess the associations between the variables studied. A paired t-test was used to compare the differences in the energy and fat contents of the pasteurized HM samples obtained by MIRIS and creamatocrit.
The total sample was randomly divided into two parts. Two-thirds (n = 1240) were used to procedure the linear regression (robust residuals) using as dependent variable energy from Miris adjusted by maternal age, lactation days, and gestational age. The other part of the sample (n = 618) was used to carry out a new correlation between energy calculated from Miris and creamatocrit corrected by the fit values obtained from the linear regression. The significance level adopted was less than 5%.
Results
The average age of the mothers was 29.7 ± 5.1 years, and the median number of days of lactation was 22 days (interquartile range [IQ]: 7.7–59.2). Full-term births were observed in 196 (95.1%) of the nurses (Table 1). The median number of samples per mother was 7.5 (3.0; 19.0). The distributions of the quantity of energy and fat obtained by MIRIS and creamatocrit are shown in Table 2 and Figure 1.
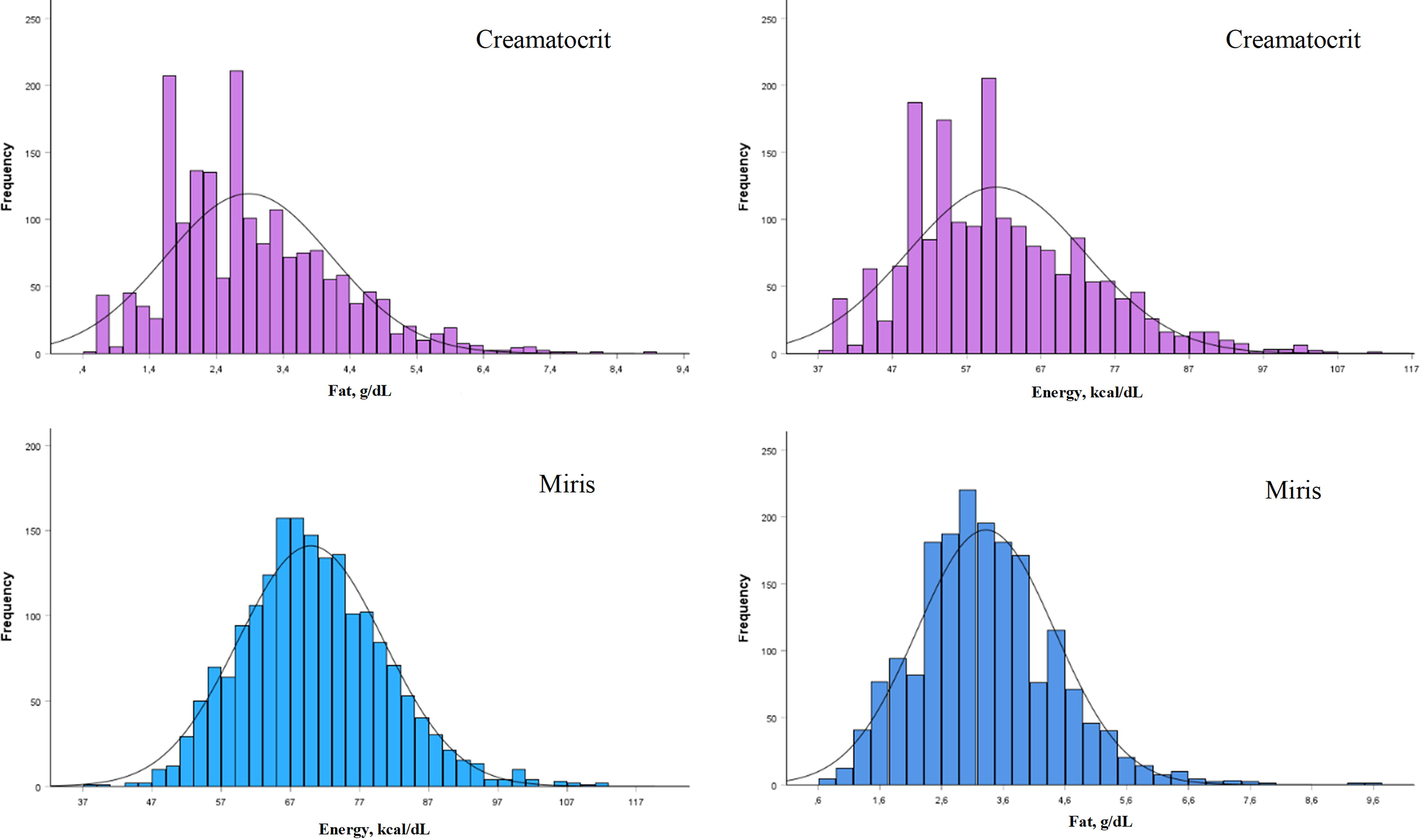
Histogram of the distribution of energy and macronutrient values assessed via the infrared method (Miris) and creamatocrit (n = 1,858).
Characterization of Donor Mothers (n = 317)
Mean ± SD.
Median (interquartile range).
N(%).
Description of Energy and Macronutrient Values per 100 mL of Human Milk Obtained by Creamatocrit and Infrared Methods (n = 1,858)
SD, standard deviation; IQ, interquartile range.
In the HM samples from women who gave birth prematurely, the median lactation time was 25.0 days (IQ: 10.0–47.0). There were no statistically significant differences in these samples’ energy and fat content (data not shown).
The energy quantity obtained by Miris in the HM samples correlated directly with the amount of fat (r = 0.585; p < 0.001) and energy (r = 0.591; p < 0.01) obtained by the creamatocrit method.
The values for energy (difference: +8.96 kcal/dL, 95% CI: 8.52–9.44 kcal/dL; p < 0.001) and fat (difference: +0.40 g/dL, 95% CI: 0.35–0.45 g/dL; p < 0.001) in the HM samples obtained by Miris were higher than those estimated by the creamatocrit (Table 3).
Pairwise Analysis of Energy and Fat Values Obtained by Infrared Method (Miris) and Estimated via the Creamatocrit (n = 1,858)
Result of the difference: MIRIS–Creamatocrit values. Significance level of paired t-tests.
The linear regression-adjusted maternal age, lactation days, and gestational age showed that the energy values estimated by creamatocrit were directly associated with those of MIRIS (β = 0.516; p < 0.001) (Table 4). Linear regression was used to generate the formula (energy kcal/dL = 38.43 + [0.516 × kcal/dL of creamatocrit]), which adjusted the creamatocrit values of energy. After this adjustment, the correlation of energy values using Miris and creamatocrit was more significant (r = 0.607, 95% CI 0.555 to 0.655) (Fig. 2).
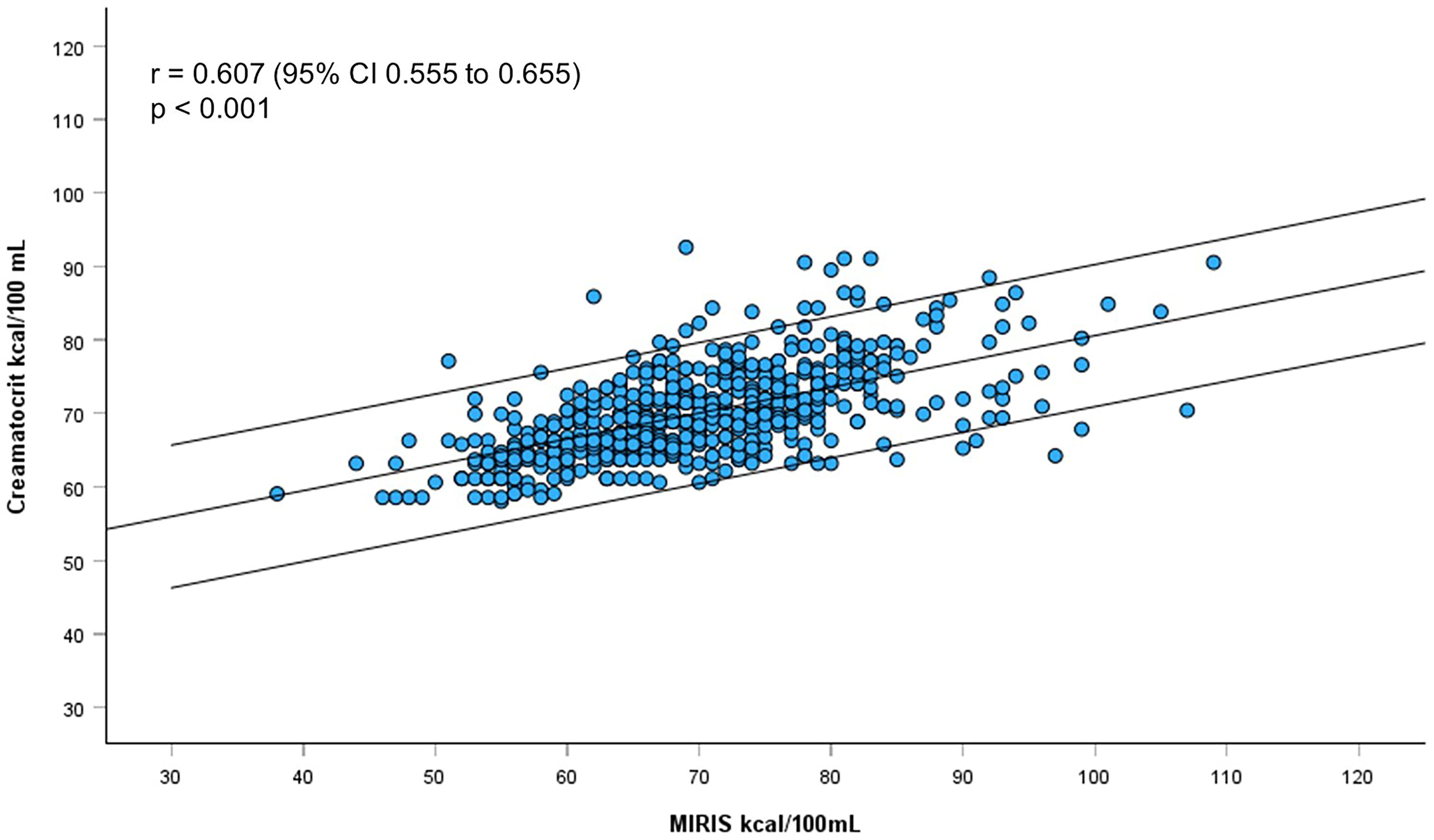
Correlation between energy values calculated by Miris and creamatocrit after adjustment with linear regression (n = 618).
Linear Regression Analysis of Energy Values Obtained by Creamatocrit and Miris (n = 1,240)
Dependent variable: Energy (kcal) obtained by Miris, adjusted for maternal age, lactation time, and gestational age.
Discussion
The results of this study provide essential information on the values of energy and fat in pasteurized HM samples evaluated with different methods. The quantity of energy and fat obtained using the infrared method was consistently higher than that of the creamatocrit.
This finding has significant implications for the accuracy and reliability of routinely used energy and fat measurements in HM. Some hypotheses may explain these findings. First, the infrared method is more accurate and sensitive when calculating the energy quantity in pasteurized HM samples. The second is that creamatocrit may not calculate all energy components in LH. Components such as short-chain fatty acids or other bioactive compounds can contribute significantly to the total energy value and are more efficiently detected by the infrared method.13,16
The use of breast milk is essential in neonatal care. Although mother’s milk is the gold standard for feeding neonates, teams in neonatal intensive care units are sometimes unable to maintain the use of exclusive breast milk throughout the hospitalization period. Factors that can interfere with this process include prolonged hospitalization, the clinical condition of PTNBs, maternal stress and associated illness, a lack of family support and appropriate places for mothers to stay with their newborns, and finally, the widespread use of infant formula. Fewer than 30% of PTNB mothers maintain some form of breastfeeding at hospital discharge. 17
The HMB plays an essential role in maintaining the exclusive use of HM for PTNBs when the mother’s raw milk is unavailable and reduces the risk of unnecessary introduction of infant formula. Pasteurized HM offers several advantages for PTNBs, such as reducing the risk of necrotizing enterocolitis and late-onset sepsis. 18 A better understanding of the composition of pasteurized HM can improve and promote nutritional therapy protocols aimed at its use for PTNBs at different times.14,19
The macronutrient content of pasteurized HM varies considerably. An Australian study, which used the same method as that used in this study, reported that the average protein content of pasteurized HM samples was 1.16 g/100 mL (0.7–1.96 g/100 mL) and fat was 3.85 g/100 mL (1.46–9.39 g/100 mL). The stages of lactation and gestational age are the main protein and fat content predictors, respectively. 20 These findings were similar to those observed in this study, which showed that gestational time and maternal age also influence the macronutrient composition of HM.
Evidence supports that pasteurization reduces fat concentration in HM, ranging from just zero to up to 25%.21,22 A recent meta-analysis suggests that the discrepant impact of pasteurization on HM fat may be related to different methodologies and preanalytical samples used. More research considering the role of preanalytical handling procedures and detailed methodologies is necessary to clarify the impact of pasteurization on fat HM composition, especially because fat has a crucial role in providing energy and supporting optimal growth in preterm infants. 23
Brazil has the largest HMB network in the world, with legislation and capillarization for updates on the safety and administration of HM. 11 Creamatocrit is a method routinely used to estimate the amount of energy and fat in LH samples. This method is based on a study published over 20 years ago. 13 Since then, no significant modifications or adjustments to this estimate have been proposed. On the contrary, in the last decade, HM composition analyzers have emerged for use in hospital units, which are relatively simple to use. However, their acquisition and maintenance costs are high for most centers. 24
A study of unpasteurized HM samples revealed that the amount of fat calculated by the creamatocrit correlated strongly with the esterified fatty acid assay method and infrared analysis. 24 However, the average estimated fat (+2.6 g/dL) and energy (+1.4 kcal/dL) contents of the creamatocrit were significantly greater than those obtained by Miris. In contrast, this study revealed that the energy and fat values of creamatocrit were lower than those of Miris (−8.96 kcal/dL and −0.4 g/dL). 25 The higher number of samples included pasteurized LH, and the different regional characteristics (health, type of diet, and maternal ethnicity) may have interfered with these findings.
Although it is more widely used because of its practicality and lower cost, creamatocrit values may have lower reproducibility and greater variation in pasteurized LH samples with low-fat content 26 and frozen samples. 27 More precise methods can be considered to improve the accuracy of calculating and measuring the quantity of energy and macronutrients in LH in a single analysis, especially pasteurized LH, to improve care protocols and pasteurization techniques.16,28
Although Brazil has a significant number of HMBs, the size of the country and the different realities of each center mean that equipment for measuring nutrients in HM, such as the one used in this study, is rarely available, and creamatocrit is recommended and routine procedure. Based on the data from this research, it was possible to propose a formula that can improve the accuracy of energy calculation by the creamatocrit in pasteurized LH samples. This calculation needs to be validated in other scenarios and populations. However, it opens a prospect for improving the results estimated by creamatocrit in places that do not have the equipment, such as an infrared analyzer.
The number of nursing and HM samples included and the use of the same pasteurization method for all the samples evaluated can be considered strengths of this study. On the contrary, the lack of more detailed maternal clinical data (nutritional status and dietary intake) and the absence of energy and macronutrient analyses before the pasteurization process can be considered weaknesses.
Conclusions
The energy and fat values of pasteurized LH samples obtained by creamatocrit and infrared methods were moderately correlated, and the quantity obtained by the creamatocrit method was significantly lower than that by the infrared method. These results indicate a promising possibility for improving the estimates made at the HMB using a creamatocrit to improve the accuracy of the assessment of energy content in pasteurized HM samples.
Footnotes
Acknowledgments
The authors thank Angela Tavares Paes for supporting the statistical analyses, Multidisciplinary Team of Womeńs Hospital of São Bernardo do Campo. The authors also thank Arthur Albiero Neto, Rotary Club São Bernardo do Campo and Cibele Wolf Lebrão, Head of Neonatology at Women’s Hospital.
Authors’ Contributions
N.P.A.: Conceptualization (lead), data curation (lead), investigation, validation, visualization, and writing. F.I.S.-S.: formal analysis (lead), investigation, methodology, supervision, and writing. R.O.S.S.: investigation, methodology, project administration (lead), supervision, validation, visualization, and writing (lead).
Disclosure Statement
The authors declare that they have no conflicts of interest in this study.
Funding Information
No funding was received for this article.