
Abstract
Background:
Some studies have explored the effects of amino acid-based formulas (AAF), extensively hydrolyzed formulas (EHF), and soy-based formulas (SF) on growth indices, weight-for-age z-scores, length-for-age z-scores, and weight in children with cow’s milk allergy (CMA).
Aims:
This review aimed to evaluate and differentiate the effectiveness of AAF, EHF, and SF on growth parameters in children with CMA.
Methods:
A systematic review was conducted in three databases—PubMed, Web of Science, and Scopus—up to March 2023 to identify eligible studies. Eight articles were analyzed in this study. Effect sizes were reported as weighted mean difference with 95% confidence intervals (CI). Statistical heterogeneity between studies was assessed using Cochran’s Q-test. The risk of bias was evaluated using the ROBINS-I tool.
Results:
A total of eight studies, encompassing 469 participants, met the inclusion criteria. The meta-analysis demonstrated a significant positive effect of the AAF and EHF on weight and weight-for-age z-scores, while no significant changes were observed for length-for-age z-scores. Furthermore, pooled effect sizes indicated that AAF had a more pronounced impact in weight-for-age z-scores (+0.30) compared with EHF (+0.25). Soy-based formulas had negligible effects on growth parameters.
Conclusion:
The findings suggest that AAF and EHF are more effective in improving growth parameters, particularly weight-for-age z-scores, in children with CMA compared with SF. Among the formulas studied, AAF showed the greatest positive impact on weight-for-age z-scores. These results highlight the importance of formula selection for optimizing growth outcomes in children with CMA.
Introduction
Cow’s milk protein allergy (CMPA) may occur within the first week of cow’s milk introduction and is characterized by an allergic reaction to milk proteins. 1 Reports indicate that the prevalence of allergies has increased in recent years across many countries, particularly among children under 5 years old, where cow’s milk allergy (CMA) is one the most common food allergies in this age-group. 2 Studies estimate that the prevalence of CMPA in infants is approximately 2.69%. 3 Symptoms of CMA include vomiting, hives, angioedema, lethargy, respiratory issues, blood in the stool, crying, diarrhea, and, in the long term, delayed growth. 4
The primary treatment of food allergies is the complete avoidance of allergen food. 5 However, eliminating cow’s milk from a child’s diet poses challenges, as it is a fundamental source of protein and nutrition for this age-group. The American Academy of Pediatrics recommends exclusive breastfeeding for the first 6 months of life and continued breastfeeding alongside complementary foods until at least 1 year of age. 6 Breastfeeding can extend beyond the first year if mutually desired by the mother and the child. 7 In children who cannot consume breast milk, alternative formulas play a critical role in supporting growth and development. 8 The European Society for Paediatric Gastroenterology, Hepatology and Nutrition emphasizes that formulas should only be used if well-tolerated by infants allergic to cow’s milk or other proteins in the formula. Specifically, formulas should demonstrate, with a 95% confidence interval (CI), that at least 90% of infants with CMPA will not react adversely. 9 Many extensively hydrolyzed formulas (EHF), amino acid-based formulas (AAF), and soy-based formulas (SF) meet these criteria. 1
EHF, AAF, and SF are considered suitable options for managing CMPA in the long term. AAF is particularly effective for children who do not respond to EHF, as it is entirely nonallergenic. If symptoms persist despite AAF use, the initial CMPA diagnoses may need to be reconsidered. SFs are also an option for children over 6 months of age, provided they undergo proper nutritional evaluation and potential effects are carefully monitored.1,8,10,11 However, these formulas have notable drawbacks. AAF and EHF are often expensive and have an unpleasant taste,12,13 whereas SF is more affordable and palatable. 13 Despite extensive research on the effects of AAF, EHF, and SF on growth, controversy persists regarding their relative efficacy. For example, while D’auria and collaborators reported no significant differences between the HF and the SF in promoting growth indices, length-for-age and weight-for-age, 14 Agostoni and collaborators found HFs to be more effective. 15 Similar disagreement exists concerning the efficacy of AAF compared with EHF. This systematic review and meta-analysis aimed to compare the efficacy of AAF, EHF, and SF in promoting weight gain, weight-for-age, and length-for-age.
Methods
Search strategy
The search for information was conducted using three electronic databases: MEDLINE, Web of Science, and Scopus until March 2023, with no language restrictions applied.
Study selection
Studies were selected for full-text review using EndNote software if they met the following criteria: (1) Patients: male or female children and adolescents with CMA; (2) Intervention and Comparison: (a) HF and AAF compared with SF and (b) AAF compared with HF; (3) Outcomes: reported sufficient data on at least one outcome of interest, namely weight-for-age, length-for-age, or weight; (4) Study Design: randomized controlled trial (RCT). Observational studies, studies without appropriate control groups, animal studies, review articles, and studies that administered soy milk in combination with other compounds, such as fructooligosaccharides, were excluded.
Data extraction
Eligible studies were included, and the following data were extracted: first author’s name, study location, year of publication, RCT (cross-over or parallel), sample size (intervention and control groups), participant characteristics (gender, age, and health status), intervention duration, quantity of formula consumed, and the means and standard deviations (SDs) of the outcomes of interest at baseline, post-intervention, and/or changes between baseline and post-intervention.
Risk of bias
The risk of bias of the included studies is presented in Table 1 evaluated based on the ROBINS-I tool. Each study is rated as a low, high, or unclear risk of bias based on the following potential sources of bias: Random Sequence Generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other sources of bias.
Quality Assessment of Included Studies
H, high; L, low; U, unclear.
Statistical analysis
Effect sizes were measured using the mean difference between the intervention and control groups at follow-up. When effect sizes were not reported, the mean values at baseline and the study’s conclusion were used. The method was applied by Hozo and collaborators: SD ¼ square root [(SD pretreatment) 2 þ (SD post-treatment) 2 − (2R SD pretreatment SD post-treatment)]. 16 For conducting a single pairwise comparison in studies with more than one control group, the groups were combined by applying a weighted average. For estimating the effect sizes, we used the random effect model (DerSimonian and Laird method) and reported the results with the weighted mean difference and 95% CI. Since some studies provided their results in graphic form, we used Plot digitizer software to extract the data. I2 index was applied for calculating heterogenicity, and I2 greater than 50% was considered an indicator of substantial heterogeneity among the trials. The cutoff values for each quantitative parameter of subgroups were the values less or more than the median. The leave-one-out method was performed for sensitivity analysis, which reported the impact of each study on the results. 17 To direct publication bias, the funnel plot was used, by Beggs’ rank correlation or Eggers’ regression test. The trim-and-fill method was used to estimate the number of potential missing studies in the meta-analysis. For statistical analysis, STATA version 11.0 was used (Stata Corp, College Station, TX), and p-values <0.05 were considered statistically significant.
Results
Study characteristics
The general characteristics of eight studies selected for final analysis are presented in Table 2. After database searches and the elimination of duplicates, a total of 5,404 studies remained and were screened for inclusion. Of these, 5,248 were excluded based on their title/abstract. A total of 156 articles were screened based on their full texts. Following the application of the inclusion criteria, 8 studies were ultimately included in this review. The study selection process is outlined in the flow diagram according to the PRISMA checklist (Fig. 1). Most of the studies were conducted in Europe,14,15,18,21,22 while others were conducted in Asia19,20 and America. 6 All studies included patients with CMA. The sample size of the studies ranged from 16 (14) to 63 participants. 15 The follow-up ranged from 2 weeks 6 to 12 months. 21 All studies enrolled both girls and boys.

The PRISMA flow diagram for literature search and selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Baseline Characteristics of Included Studies
AAF, amino acid-based formula; CH, casein hydrolyzed; CHF, cow’s hydrolyzed formula; CMA, cow’s milk allergy; EHF, extensively hydrolyzed formula; eHWF, extensively hydrolyzed whey formula; nRCT, Nonrandomized Clinical Trials; RCT, randomized controlled trial; RH, rice hydrolyzed; SF, soy formula; SH, soy hydrolyzed; WH, whey hydrolyzed.
Meta-analysis
The meta-analysis revealed a significant effect of both AAF and HF on weight gain (0.10 kg; 95% CI: 0.01, 0.19; p = 0.023; I2 = 99.5%) (Fig. 2A) and weight-for-age z-score (0.25; 95% CI: 0.00 to 0.50; p = 0.047; I2 = 29.7%) (Fig. 2B). However, no significant changes were observed for length-for-age z-score (0.07; 95% CI: −0.29 to 0.44; p = 0.69; I2 = 69.7%) (Fig. 2C). A subgroup analysis to explore potential sources of heterogeneity was not feasible due to study limitations.
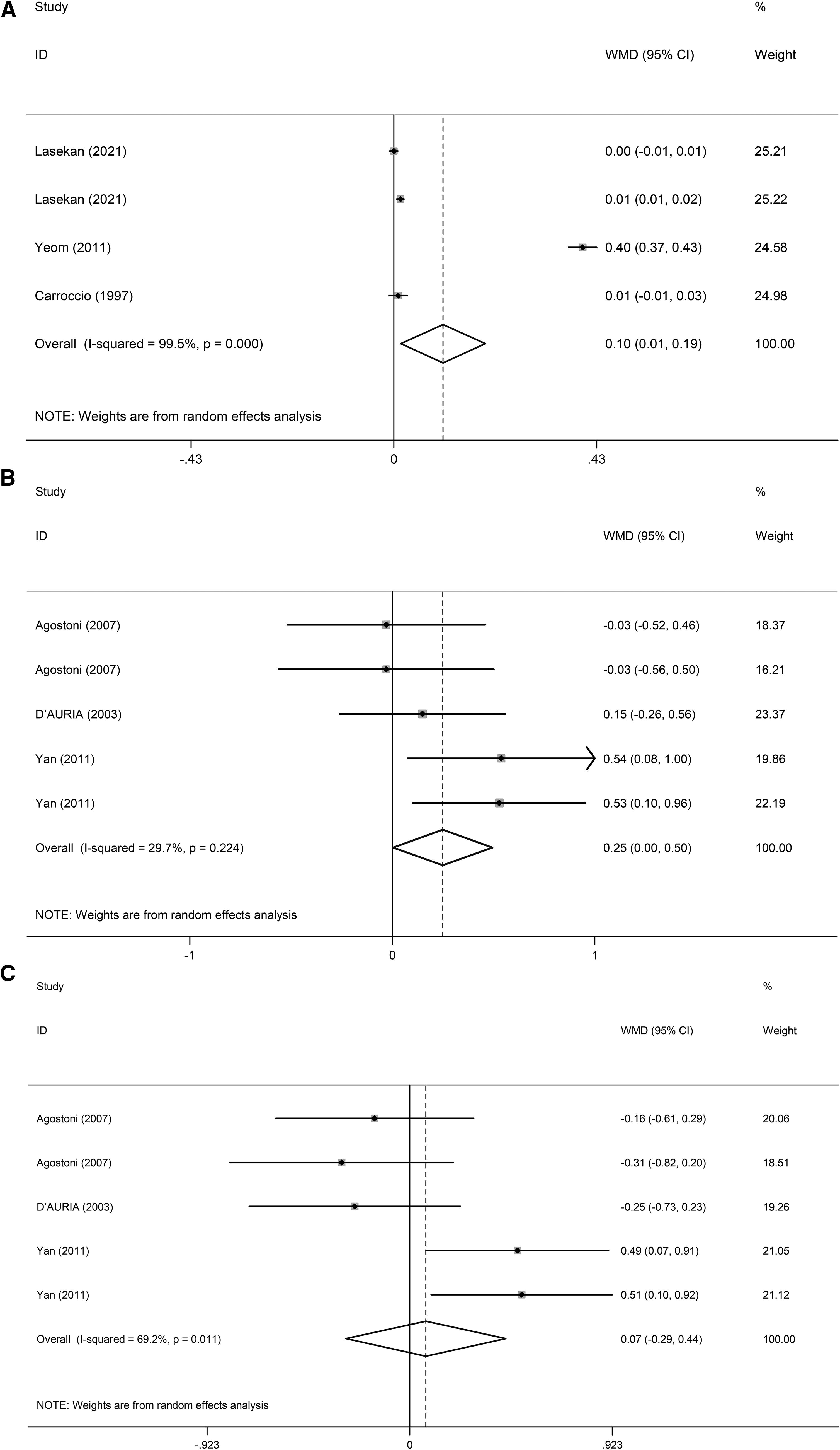
Forest plots from the meta‐analysis of clinical trials investigating the effects of hydrolyzed and amino acid-based formula compared with soy formula on
The pooled effect sizes indicated a significant benefit of the AAF on weight-for-age (0.30; 95% CI: 0.06 to 0.54; p = 0.015; I2 = 0.0%) compared with HF (Fig. 3).
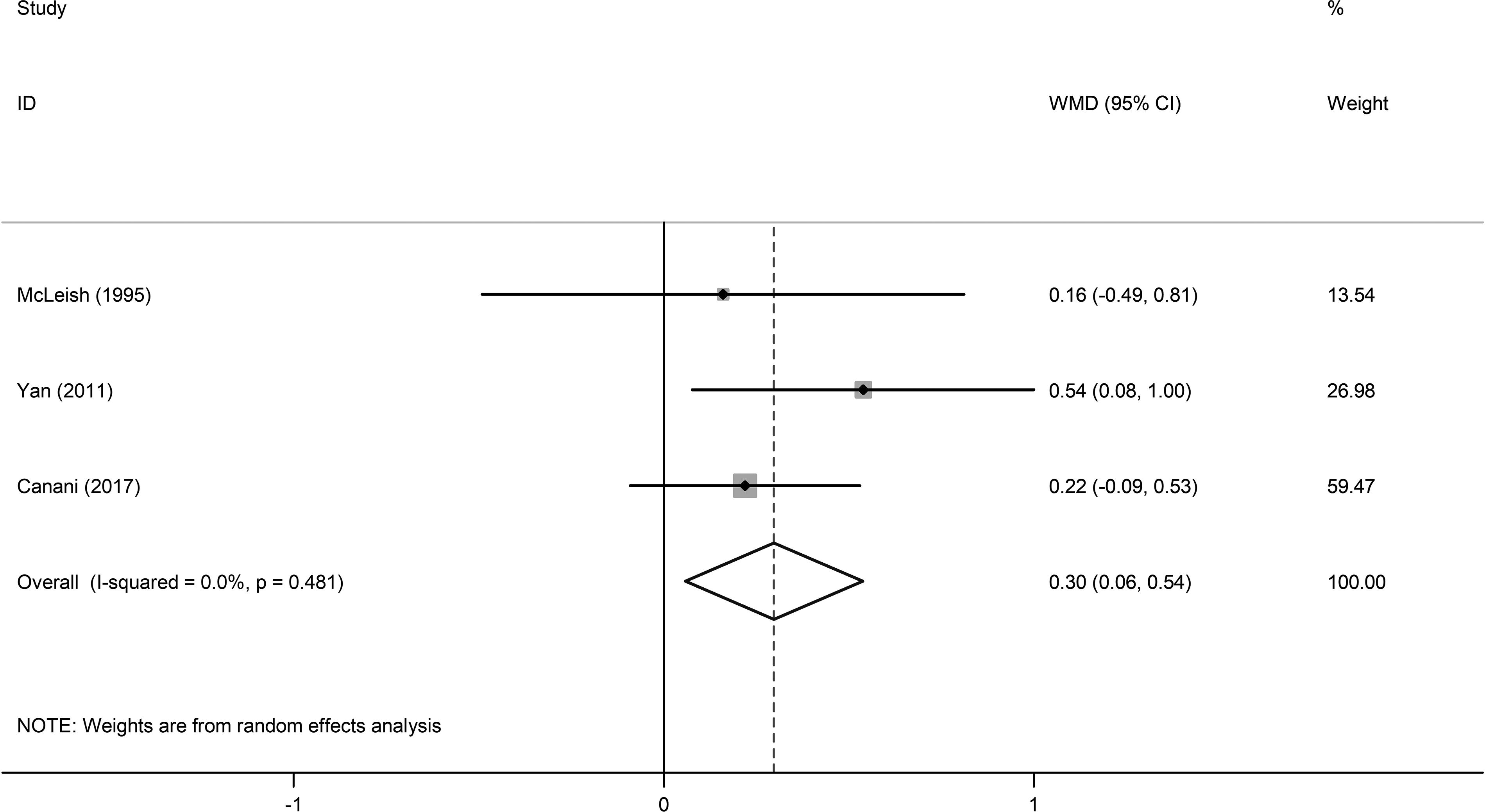
Forest plots from the meta‐analysis of clinical trials investigating the effects of amino acid-based formula compared with hydrolyzed formula on weight-for-age.
Sensitivity analysis
The leave-one-out method was applied to assess the influence of each individual study on the pooled effect size. The results remained robust after the sequential removal of studies (Supplementary Figs. S1 and S2).
Publication bias
Visual inspection of the funnel plot revealed no evidence of publication bias regarding the impacts of HF, AAF, and SF on the outcome measures. Additionally, the results of Egger’s regression test supported the absence of significant publication bias for weight (p = 0.23) and weight-for-age (p = 0.33). Although significant evidence was seen for height-for-age (p = 0.02), the trim-and-fill analysis did not identify any missing studies (Supplementary Figs. S3 and S4).
Discussion
The goal of the present systematic review and meta-analysis was to compare the effect of HFs, AAFs, and SFs on growth parameters, weight-for-age z-scores, length-for-age z-scores, and weight in childhood and adolescence. To the best of our knowledge, this is the first systematic review and meta-analysis to evaluate and compare their effectiveness. Eight studies with a total of 469 participants met the inclusion criteria. Among these, three studies evaluated AAF, eight evaluated HF, and six evaluated SFs.
Based on our results, both AAF and HF showed a statistically significant effect on growth indices compared to SF. Specifically, the weight-for-age z-score increased by +0.30 for AAF and +0.25 for HF, while SF showed no significant improvement. The impact of the AAF formula on weight-for-age z-scores (+0.30) was greater than that of HF (+0.25).
Several studies have analyzed the efficacy of these formulas in promoting growth. Some studies concluded that HF supports normal growth,23,24 while SF has also been reported to be effective.25,26 AAF has also been shown to be effective. 27 The efficacy of the formulas, however, varies across studies. In line with our results, one study found that HFs were more effective than SFs, 15 while another study reported the opposite. 19 Contrary to our findings, one study showed similar effects to AAF and HF on growth. 21
The reasons for impaired growth in children with CMA are varied, but they may include (1) inflammation of the intestinal mucosa due to allergy, which leads to nutrient loss and reduced bioavailability28,29; (2) increased energy requirements30; and (3) elevated energy expenditure due to agitation. 31 For these reasons, introducing a hypoallergenic formula for patients with CMA can be beneficial for their growth. In the study evaluating these formulas, both AAF and EHF resulted in increased growth in patients with CMA, while the growth rate was significantly slower in the SF group. 20
Infant formula is designed as a potent substitute for breast milk, aiming to mimic its nutritional profile. These formulas are categorized into three main groups: (1) cow milk-based formula, (2) SF, and (3) specialized formula, including AAFs or those containing extensively hydrolyzed whey or casein proteins. 32
Hypoallergenic formula refers to formulas specifically intend to prevent allergy and/or treat CMA. 33
In general, extensively or partially hydrolyzed formulas are the first line of treatment in CMA. Even though it is realized as a hypoallergenic formula in up to 10% of patients, it can induce allergic reactions and should be replaced with AAF.1,34 EHFs are produced by hydrolyzing cow’s milk protein in smaller sizes. 32 The difference between partially hydrolyzed formulas (PHFs) and EHFs is in their molecular weight. PHFs have a higher molecular weight. 33 HFs are generally well tolerated by patients with CMA and are nutritionally adequate, but they have some drawbacks, such as high cost, low palatability, and the potential to cause anaphylaxis. 35
Though HFs are proper for most infants with CMA, some infants may react to small peptide fragments. 36 AAF is made of synthetic amino acids, fats, carbohydrates as glucose polymers, and micronutrients. 34 AAFs are expensive, not delicious, and not widely accessible. 35 Their odor and palatability are even worse than EHFs, 35 and their cost-effectiveness is lower than EHFs. 37 Among its advantages is the lack of protein residual allergenicity, better digestion, and absorption. Furthermore, they may contain different percentages of fat which lead to diminished deficiencies in essential fatty acids. 37
While using an SF, we should consider two facts: (1) their isoflavones content and (2) their phytate content, which lessens the absorption of minerals and trace elements. It is worth mentioning that most recent SFs have lower levels of phytates with higher levels of zinc, iron, and calcium compared with previous formulas.38,39 Besides, transgenic soybeans use in these formulas is a concern. 40 “Nutrition for Healthy Term Infants” recommends EHF for CMA; however, SFs are more frequently used for these children. The underlying factors for this selection include (1) their lower cost and (2) their higher palatability. 13
The present study had several limitations. First, the number of studies included for the analysis was small. Second, the source of protein varied across the HF. Third, potential sources of heterogeneity could not be identified, as subgroup analysis was not performed. Fourth, the duration of the studies varied. Fifth, a dose–response meta-analysis could not be conducted due to insufficient data in some studies. Sixth, the study is limited by the lack of longitudinal follow-up to evaluate changes in linear growth and body composition. Although we observed significant weight gain in children with CMA, the lack of a concurrent increase in height suggests that this weight gain may represent fat mass rather than lean body mass. Future research should include comprehensive assessments of body composition and longer follow-up periods to evaluate the proportionality of growth in this population. Seventh, while the current study highlights the effect of AAF and HF on weight gain in children with CMA, the lack of longitudinal data on height limits the ability to evaluate the formulas’ potential impact on linear growth. Further studies with extended follow-up periods are needed to assess whether the observed weight gain translates to improvements in height and overall proportional growth.
The strengths of the present study are as follows: (1) it is the first meta-analysis comparing the effects of these three different formulas on growth indices, (2) we based our analysis on three formulas, (3) we minimized the methodological issues, and (4) we measured the risk of bias of included studies with an established tool.
Conclusions
In conclusion, both AAF and HF have a greater impact compared with SF. Moreover, the effect of the AAF is stronger than that of HF. Given the limitations of this study, the findings should be interpreted with caution.
Footnotes
Acknowledgments
The authors express their gratitude to the participants of this study. This article is taken from disease registry, titled “Registry of Food Allergy in Iranian Pediatric” with code number IR.SBMU.RICH.REC.1400.043 from ethics committee, that was supported by the deputy of research and technology in Shahid Beheshti University of Medical Sciences (![]() ).
).
Authors’ Contributions
S.F. and A.M.H. conceived the study, carried out the literature search, and wrote the article. A.M.H., N.S.G., and S.F. carried out data extraction and independent reviewing. A.M.H. assessed the quality of included studies. F.S. and S.F. performed data analysis and interpretation. F.S. and N.S.G. revised the article. The article has been read and approved by all authors.
Confirmation Statement
Our research is supported by an institution that is primarily involved in education or research.
Author Disclosure Statement
No financial or nonfinancial benefits have been received from any party related directly or indirectly to the subject of this article.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. All authors are primarily involved in education or medical research and are not directly supported by the government.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.