
Abstract
Background:
Social determinants of health account for racial inequities in breastfeeding rates in the United States. There is a gap in the role of neighborhood socioeconomic status (NSES) as it relates to breastfeeding disparities.
Methods:
Using longitudinal data from the Black Women’s Health Study, we assessed associations of NSES with breastfeeding initiation and duration in a cohort of primiparous U.S. Black women. We also explored associations within strata of important economic indicators, including education, occupation, and marital status.
Results:
Breastfeeding initiation (n = 2,705) increased with NSES quartile, from 75.2% in the lowest quartile to 88.3% in the highest quartile (p < 0.0001). Compared with women living in the highest NSES quartile, those in the lowest quartile had a 41% (odds ratio: 0.59 [95% confidence interval: 0.43, 0.81]) decreased odds of initiating breastfeeding. For breastfeeding duration (n = 2,172), women residing in NSES quartiles 1–3 were significantly less likely (p < 0.0001) to breastfeed (44.4%) for 6+ months compared with those living in the highest quartile (62.8%). Adjusted relative risks for those in quartiles 1–3 compared with 4 (highest) were 0.63 (0.45, 0.87), 0.50 (0.37, 0.68), and 0.64 (0.47, 0.86), respectively (p = 0.0001). There was no statistically significant evidence of effect modification by education, occupation, marital status, and region (Pinteraction = >0.05).
Conclusion:
Living in a lower NSES environment was associated with reduced breastfeeding initiation and duration compared with a higher NSES environment. Research is needed to understand the mechanisms by which neighborhood-level factors influence breastfeeding initiation and duration for Black women in the United States.
Introduction
Breastfeeding is a critical foundation of public health promotion and disease prevention. In updated guidelines, the American Academy of Pediatrics recommends breastfeeding initiation within the first hour of birth, exclusive breastfeeding for 6 months continuing for at least the first 2 years of life with the addition of complementary foods, and as long thereafter as is mutually desired. 1 Longer breastfeeding duration relative to shorter is associated with reduced risk of acute and chronic illness in children. 2 For women who breastfeed, a longer duration of lactation is associated with reduced risk of breast and ovarian cancer and other chronic metabolic illnesses such as type 2 diabetes. 2 Breastfeeding can influence future health risks at subsequent stages of life for women and children, 3 with higher population level rates of breastfeeding contributing to economic benefits 4 by reducing health care costs and inequities by race. 5
In the United States, the majority of women choose to initiate breastfeeding, but many stop breastfeeding before the recommended duration. 2 Breastfeeding rates have steadily increased over decades, but inequities in breastfeeding outcomes by race persist. Non-Hispanic White infants have higher rates than non-Hispanic Black infants (hereafter White and Black). 6 In 2021, initiation rates for White infants were 86.2% compared with 75.4% for Black infants. 7 Duration rates reflect a larger percentage difference for 3 months of exclusive breastfeeding for White infants (50.3%) compared with Black infants (39%). Similarly, at 6 months “any breastfeeding” for White infants (63.4%) was relative to Black infants (51.7%). 7 For White infants at 12 months, any breastfeeding was 42.5% compared with 31% for Black infants. 7
Differences in breastfeeding outcomes by race have been attributed to social drivers of health, including exposure to racism 8 resulting from a legacy of slavery in the United States,9–12 whereby women who were enslaved served as wet nurses for enslavers’ children. 13 Present-day mechanisms by which racism influences broad population health outcomes have been extensively investigated. 14 Structural inequities are associated with access to societal resources, 14 but neighborhood-level factors may also contribute to individual behaviors by way of community norms and values. 15
Residential neighborhood segregation is one mechanism that has been reported to contribute to breastfeeding inequities by race. 12 We previously found that Black women who reported growing up in a racially segregated neighborhood had lower odds of breastfeeding initiation and shorter duration compared with women who did not grow up in a racially segregated neighborhood. 12 Reasons for these differences may reflect exclusion from societal resources such as access to the highest standard of hospital lactation support for areas with a greater proportion of Black residents compared with other groups.16,17
Neighborhood-level factors relative to breastfeeding initiation and duration have also been examined by education status among urban women, 18 exposure to neighborhood violence, 19 and experiences of racism with the police and in housing 12 with mixed results. Yourkavitch et al. reported racial and ethnic variation on exclusive breastfeeding (EBF) and any breastfeeding, depending on measures of affluence and deprivation among a large urban population. 20 Specifically, the odds of EBF decreased as neighborhood disadvantage increased for all but White women, but the odds of any breastfeeding were positively associated with increasing affluence for all but Hispanic women. 20
Grubesic and Durbin called for “spatial equity” in supportive services, citing the inequitable distribution of lactation support that has historically favored White, educated, affluent women in urban and suburban areas. 21 In our previous work, women who experienced racism in settings with the police had increased odds of ever breastfeeding and breastfeeding for longer durations. 12 Given the persistence of racial segregation in housing, Black women at all levels of individual socioeconomic status (SES) tend to live in more disadvantaged neighborhoods than their White counterparts, irrespective of individual levels of education.22,23
We aimed to build on emerging “place-based” research in the field of breastfeeding inequities by assessing the association between neighborhood socioeconomic status (NSES) and breastfeeding initiation and duration in a cohort of U.S. Black women. We also sought to explore this association within strata of important economic indicators, including education, occupation, and marital status.
Methods
Study design and human subjects
The methods of the Black Women’s Health Study (BWHS) have been described in detail elsewhere.12,24 Briefly, the BWHS is a prospective cohort of 59,000 U.S. Black women who enrolled in 1995 when they were 21–69 years of age. Biennial follow-up questionnaires from 1997 to 2023 have collected information on numerous health outcomes. Incident births were collected on the 1995 through 2005 questionnaires. The BWHS was approved by the Boston University Institutional Review Board (IRB), and the UMass Chan Medical School IRB determined that the analyses were exempt from review due to de-identified data.
Measurement
We recognize that the term “breastfeeding” may differ by personal preference. In this study, we intentionally use “breastfeeding” to be consistent with the data as it were collected.
Breastfeeding initiation is a measure of whether a parent begins breastfeeding following the birth of the infant. 12 The BWHS assessed breastfeeding outcomes at baseline and biennially from 1999 through 2005, with the question “Did you breastfeed the baby?” Responses were dichotomous “yes” or “no.”
Breastfeeding duration refers to how long after the birth the child received their mother’s milk. In 1999 and 2001, participants who responded “yes” to the question “Did you breastfeed?” were prompted to report how long with the categories <3 months, 3–5 months, 6 months, or more. In the following survey cycles (2003 and 2005), the response was open ended, and participants were prompted to write a numerical response. The continuous data were transformed to match the categories described above. In the 2011 survey cycle, an open-ended question was included to fill in for missing data for both initiation and duration in previous cycles.
Neighborhood socioeconomic status is a measure that was created using residential addresses that were geocoded to year 2000 U.S. census data. 22 A factor analysis was conducted of 29 block group census variables measuring dimensions of education, income, and wealth, from which we selected 6 variables to represent NSES. These were median household income; median housing value; percentage of households receiving interest, dividend, or net rental income; percentage of adults who completed college; percentage of white-collar employed persons; and percentage of families with children that are not headed by a single woman. Factor analysis regression coefficients were used to weigh and combine the six variables into an NSES score that was divided by quartiles, whereby 1 represents the lowest quartile and 4 the highest quartile. 25
Covariate selection was based on the literature and previous analyses. 12 Height (inches) and occupation (professional/managerial, sales/clerical, student, other/unemployed) were reported on the 1995 baseline questionnaire. Years of completed education (≤12, 13–15, 16, ≥17) were assessed on both the 1995 and 2003 questionnaires, and marital status (married, living as married, divorced, widowed, single/never married) was assessed on the 1997, 1999, and 2005 questionnaires. Participant age (years), current weight (pounds), and geographic region (Northeast, South, Midwest, West) were assessed on each questionnaire between 1997 and 2005. Height and weight were used to calculate body mass index (BMI) in kilogram per square meter.
Analytic sample
The current study is a secondary analysis of data used to explore the relationship between perceived racism and lactation 12 and was limited to primiparous women to reduce confounding associated with having breastfed previous children. 26 Therefore, participants who had more than one child (n = 36,130) or remained nulliparous through 2005 (n = 13,972), the last time questions were asked on breastfeeding, were not eligible. In addition, we excluded 5,863 women who did not complete the 1997 questionnaire, which was the source of data on experiences of racism. In an earlier analysis within the BWHS, approximately 30% of women reported the same racism scores between 1997 and 2009. 27 In 2006, 28 we also reported the kappa statistics for the consistent responses to the racism questions among a sample of women who submitted duplicate questionnaires in 1997. There was high agreement between the first and second returned questionnaires.
The eligible cohort therefore comprised 3,036 primiparous women. Further excluded were 41 women with missing data on breastfeeding and 290 with missing covariate information, resulting in a total of 2,705 for the breastfeeding initiation analyses. For analyses of breastfeeding duration, we excluded women who did not initiate breastfeeding (n = 497) and those who had missing or discrepant breastfeeding duration data (n = 36), resulting in 2,172 participants for the duration analyses.
Statistical analyses
We used binomial logistic regression to estimate odds ratios (ORs) and 95% confidence intervals (95% CIs) for the relationship of NSES with breastfeeding initiation and multinomial logistic regression to estimate relative risks (RRs) and 95% CIs for the association of NSES with breastfeeding duration. For each association, we performed age- and multivariable-adjusted regression analyses. The fully adjusted model included age, BMI, education, marital status, geographic region, and occupation. Finally, we tested effect modification of NSES by years of education (<16 years versus 16+ years), occupation (white collar versus not white collar), and marital status (ever versus never married) and by geographic region according to U.S. Census Bureau divisions (Northeast, South, Midwest, West). 29 All analyses were conducted using SAS Version 9.4 (SAS Institute, Cary, NC).
Results
Between 1997 and 2005, there were 2,705 primiparous births from all regions of the United States. Baseline characteristics in 1997 are shown in Table 1. The mean age of the sample was 31.6 years, approximately 68% had 16 years or more of education, over half (52.1%) were married or living as married, and 41.6% reported being single or never married. Over one third (37.7%) reported living in the U.S. South followed by Northeast, Midwest, and West, respectively. Nearly 60% reported being in professional/managerial occupations followed by sales/clerical and students, respectively; 8% reported other or unemployed occupation status.
Characteristics of Primiparous Women (1997–2005), Black Women’s Health Study (n = 2,705)
M, mean; SD, standard deviation.
As shown in Table 2, the percentage of participants initiating breastfeeding rose steadily from 75.2% in the lowest NSES quartile to 88.3% in the highest quartile (p < 0.0001). Compared with women residing in the highest quartile of NSES, those in the lowest quartile were estimated to have 61% decreased odds of initiating breastfeeding (OR: 0.39 [95% CI: 0.29, 0.53]). Upon adjustment for covariates, the association was attenuated to 41% decreased odds of initiation (OR: 0.59 [95% CI: 0.43, 0.81]).
Odds Ratios (95% CI) for the Association Between Quartile of Neighborhood Socioeconomic Status and Breastfeeding Initiation (n = 2,705), Black Women’s Health Study 1997–2005
Adjusted for age, body mass index, education, marital status, geographic region, and occupation.
CI, confidence interval; SES, socioeconomic status; MV, multivariate.
We assessed effect measure modification of the above associations and breastfeeding initiation within strata of education, occupation, marital status, and region (Fig. 1). The associations of NSES quartile with initiation were similar across subgroups with no statistically significant evidence of effect modification (Pinteraction = >0.05).
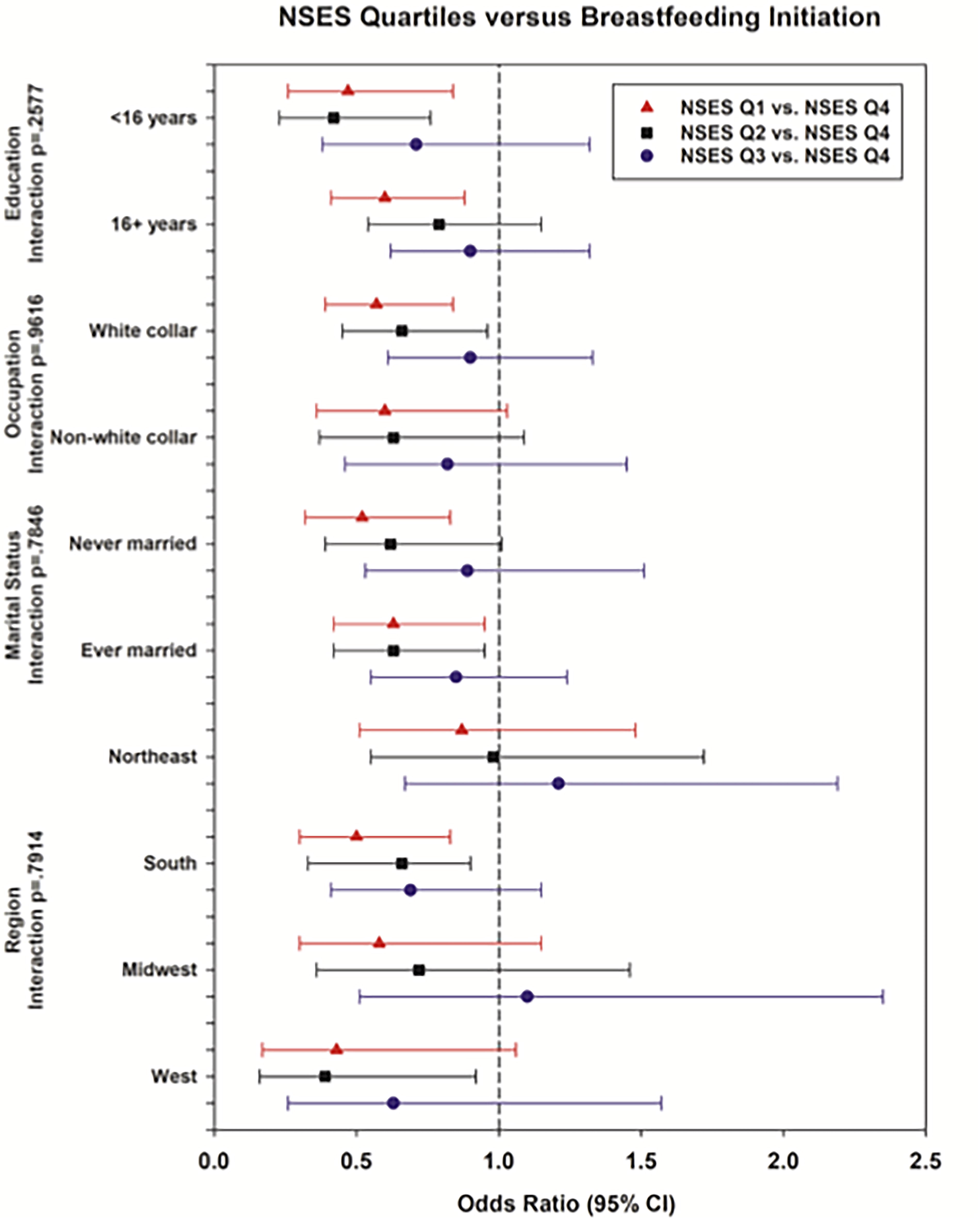
Neighborhood SES and breastfeeding initiation within strata of age, education, occupation, marital status, and geographic region. SES, socioeconomic status.
Among women who initiated breastfeeding, both <3 months and 3–5 months duration were inversely associated with NSES quartile (Table 3). The proportion breastfeeding for <3 months (short duration) decreased from 27% in the lowest quartile of NSES to 17%, while the proportion breastfeeding for 3–5 months decreased from 28.6% in the lowest quartile of NSES to 20% in the highest quartile (p < 0.0001). Conversely, those residing in quartiles 1–3 were significantly less likely to breastfeed for 6+ months as the percentage of long-duration breastfeeding increased from 44.4% in the lowest quartile of NSES to 62.8% in the highest quartile (p < 0.0001). For women who breastfed for 3–5 months (versus <3 months), the adjusted RRs for those in the lower quartiles of NSES (quartiles 1–3) compared with the highest (quartile 4) ranged from 1.05 to 0.70, but none achieved statistical significance. For long-duration breastfeeding (versus short), the adjusted RRs for those in quartiles 1–3, compared with quartile 4, showed statistically significant lower likelihood of breastfeeding for 6+ months as follows: 0.63 (0.45, 0.87), 0.50 (0.37, 0.68), and 0.64 (0.47, 0.86), respectively (p = 0.0001). As shown in Table 3, the association is driven by the longer duration (6+ months versus < 3 months).
Adjusted Odds Ratios and Risk Ratios (95% CI) for Association Between Quartile of Neighborhood Socioeconomic Status and Breastfeeding Duration Among Those who Initiated Breastfeeding (n = 2,172) Black Women’s Health Study, 1997–2005
Breastfeeding duration reference category is <3 months.
Adjusted for age, body mass index, education, marital status, region, occupation.
CI, confidence interval; SES, socioeconomic status.
As we did with breastfeeding initiation, we assessed effect measure modification of the associations between NSES and breastfeeding duration within strata of education, occupation, marital status, and region (Fig. 2). Once again, there was no evidence of effect modification of the relationship between NSES quartile and duration of breastfeeding (3–5 months versus <3 months, 6+ months versus <3 months), as RRs were similar across subgroups (Pinteraction = >0.05).
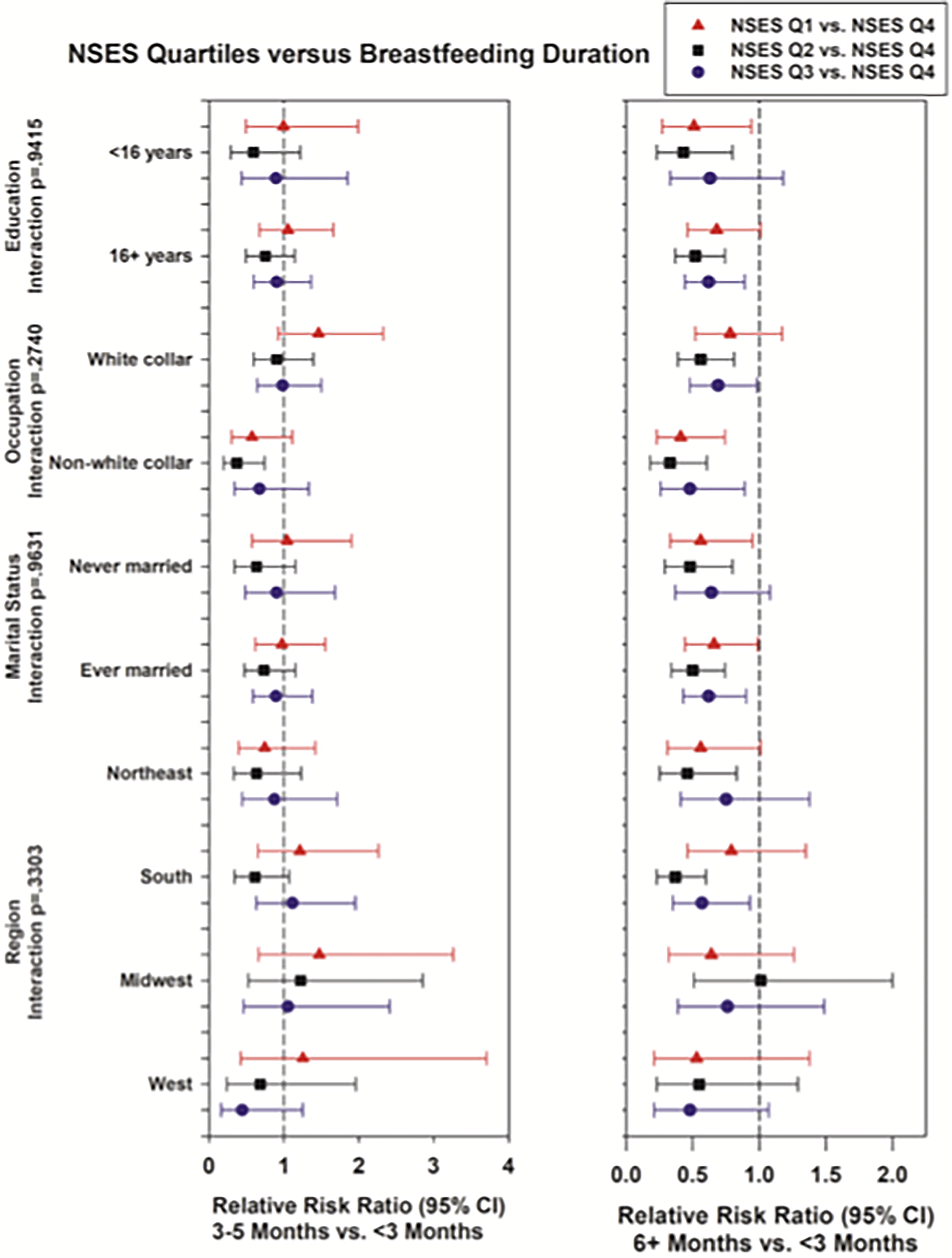
Neighborhood SES and breastfeeding duration within strata of age, education, occupation, marital status, and geographic region. SES, socioeconomic status.
Discussion
In the present analyses among primiparous U.S. Black women, residing in low NSES settings relative to high NSES settings was associated with lower initiation of breastfeeding and shorter duration among those who initiated breastfeeding. We also explored interactions between strata of education, occupation, and marital status. Findings from this large sample of women, who all identified as Black, demonstrated that low NSES was associated with reduced breastfeeding initiation and shorter duration even among women who had a college degree or more. These findings diverge from previous reports that support the role of educational attainment in breastfeeding outcomes. It is generally accepted that education level is positively associated with breastfeeding regardless of race and ethnicity.8,30 One explanation for this finding may be that our sample is entirely inclusive of women who identify as Black. Thus, we likely see a greater expression of heterogeneity than is currently reflected in U.S. breastfeeding surveillance data. Surveillance data have historically been hindered by small sample sizes according to race and ethnicity, 31 making stratification by education and other social intersecting factors challenging.
Furthermore, breastfeeding is solidly situated within the birth continuum. It is possible that education effects seen in pregnancy and birth disparities continue into the breastfeeding experience. For example, a recent study compared adverse infant outcomes among Black women who had a college education and White women attaining a high school degree. The authors reported that although Black women held advanced degrees, they were still disadvantaged by socioeconomic, school, and neighborhood characteristics, 32 representing possible pathways of systemic racism. 33 In keeping, it is reasonable that neighborhoods characterized by lower NSES may account for neighborhood differences in breastfeeding outcomes for highly educated Black women. This proposed scenario may illuminate social exclusion from resources necessary to breastfeed despite educational attainment. It is imperative that future research aim to understand the full expression of how Black women experience breastfeeding according to an intersectional paradigm that accounts for multidimensional identities. 34
NSES and breastfeeding
Neighborhood-level factors, including measures of socioeconomic status, race, and education, are complex intersecting mechanisms that contribute to breastfeeding outcomes in ways that are challenging to disentangle. It is possible that in the presence of neighborhood racial segregation, the aforementioned attitudes and practices can become entrenched through the establishing of social norms, similar to what has been observed in studies of obesity.35,36 There is an absence of consistent neighborhood level measures that allow for comparison across studies. Yet, the findings reported here indicated that lower odds of initiating breastfeeding and shorter breastfeeding duration at 6 months were associated with living in the lowest quartile of NSES relative to the highest quartile. Broadly, “place-based” breastfeeding disparities by race have been examined by neighborhood segregation, racism in housing and with policing, 12 neighborhood affluence and disadvantage, 20 and housing insecurity and conditions. 37
Using a life course perspective, Griswold and colleagues 12 reported lower breastfeeding initiation and shorter duration for women living in a segregated neighborhood relative to women not living in a segregated neighborhood. Access to societal resources is a critical dimension of health equity. In this case, access to optimal lactation clinical care may be restricted in neighborhoods that are predominately Black. One study 38 used geodemographic methods to understand the geographic distribution or “spatial equity” of mother-to-mother breastfeeding support groups. The findings highlight that the availability of such support may favor communities that are predominately White and affluent. Increasing access to support is not only about providing support groups but also considering how breastfeeding parents can physically get there, by way of transportation or by having remote options. 21 Reasonably, limited breastfeeding support in Black neighborhoods occurs across educational levels. Conversely, it is important to note that increasing investment in community-led efforts and increasing clinicians who identify as Black consistently improve breastfeeding for women who identify as Black.39–41 Culturally matched virtual support groups have also demonstrated, through a community-based participatory method, that this type of support is well accepted by African American women. 42
Perception of neighborhood safety has also been investigated with racial and ethnic differences. Using data from the National Survey of Children’s Health (n = 29,829), Kummer and colleagues 43 described community factors that may influence breastfeeding. Contrary to their hypothesis, in racial subgroup analyses, living in a perceived safe neighborhood was inversely associated with exclusive breastfeeding for Black non-Hispanic participants. Prior findings from BWHS analyses 12 demonstrated that experiences of racism with police and in the housing sector were predictive of increased odds of breastfeeding initiation and duration relative to participants not reporting experiences of racism in these domains. Data to identify underlying reasons for this finding were not available, but it is possible that breastfeeding parents chose to be inside in areas with greater police activity, facilitating the breastfeeding relationship. Police interactions and neighborhood safety are reasonably related domains; however, research is scarce in the context of breastfeeding and lactation. Emerging research in the field of pregnancy underscores police violence as a determinant of biological stress 44 leading to pregnancy loss. By extension, even the anticipation of police violence was a source of anxiety for Black mothers. 45 Given that breastfeeding and lactation are the sequelae of birth, it is critical to understand how families experience breastfeeding decision-making in the context of neighborhood safety and police violence.
Another study reported that EBF decreased as neighborhood disadvantage increased for all racial and ethnic groups except for White women, 20 indicating important racial differences in how neighborhood-specific factors influence breastfeeding. Housing insecurity is another concept applied to the study of “place-based” breastfeeding behaviors by Medicaid eligible families living in New York City and Pittsburgh. 37 Reno and colleagues highlighted variation across race and ethnicity. Overall, measures of housing insecurity such as the threat of foreclosure and eviction predicted lower exclusive breastfeeding at 6 months. Household crowding predicted EBF through intention to breastfeed for predominately Hispanic families but not for predominately Black families. The authors reported that breastfeeding is a cultural norm for Hispanic families, and multigenerational families may provide support. 36 From a public health perspective, no one factor is sufficient to predict social drivers. These findings support the critical need to disentangle neighborhood-level factors to understand the social environments that optimally support Black families’ breastfeeding experiences. The expansion of research surrounding neighborhood level factors particularly in the context of health equity for Black families is warranted.
Historical influences on NSES
Wet nursing is a global, age-old practice of breastfeeding and caring for another’s child. 46 During U.S. slavery, African American women were forced to serve as wet nurses, often to the detriment of their own children’s health and parental bonding, 13 thereby altering African American/Black (AA/B) women’s traditional breastfeeding practices. It has been hypothesized that this disruption, and the negative association of breastfeeding with oppression, may have shaped long-term attitudes toward breastfeeding within AA/B communities.11,47 Theoretically, attitudes and perceptions precede behavioral intentions.
Data from focus groups have explicitly highlighted non-normalized perceptions of breastfeeding. 47 Other focus groups 11 provided a direct connection to the slavery era and subsequent generational trauma such as stealing breast milk from slaves, images of slaves feeding White babies, and the lack of choice for enslaved women at the time. Thus, exercising the “choice” or decision to either breastfeed or formula-feed one’s child may be directly related to the lack of choice during the slavery era.
Furthermore, in the aftermath of slavery, AA/B women faced steep structural and cultural barriers to breastfeeding, including exploitative employment, lack of parental leave and other benefits, hyper-sexualization of exposed breasts, and targeted marketing by formula companies. 11 The legacy of these structural barriers is evident in neighborhood socioeconomic factors. In addition to predatory marketing efforts of the commercial formula industry, authors have argued that government-sponsored programs incentivized Black women to formula-feed by providing greater benefits through food packages to women who formula fed versus breastfed. 48 Although efforts to provide participants of the Special Supplemental Program for Women, Infants, and Children (WIC) with breastfeeding support have increased, WIC remains the largest purchaser of commercial formula and almost half of the total WIC budget is spent on formula. 49 In the present day, the effects of formula marketing, lack of federal regulation, and subsequent supply chain shortages continue to disadvantage AA/B communities. 50
Strengths and Limitations
This report is strengthened by its prospective design and large sample size representing all regions of the United States, allowing for stratification of outcomes by education and geographic region. The high follow-up rate of the BWHS cohort minimizes the impact of selective losses. We were able to objectively measure the neighborhood environment of participants by linking their residential addresses to U.S. Census data. There is little consensus as to the optimal manner for measuring NSES or neighborhood concentrated disadvantage, but the composite NSES variable we utilized has been associated with other important outcomes in the BWHS, including obesity, type 2 diabetes, breast cancer, and mortality. We also controlled for several important individual-level confounders, including age, BMI, and occupation. We did not, however, have detailed data on additional neighborhood characteristics such as individual and community support and/or access to health care, including lactation support services.
In terms of limitations, BWHS is not a random sample of U.S. Black women. Nevertheless, participants represent all regions of the United States. Approximately 97% of all BWHS participants have completed high school or a higher level of education. In comparison, 83% of the U.S. Black female population in the same age-group have at minimum a high school education.51,52 Thus, our results should apply to most U.S. Black women. Next, only a proportion of the BWHS cohort (<4%) could be studied for this article, potentially limiting generalizability.
Finally, data used in the present study were collected between 1997 and 2005, and arguably, social forces have changed. Over the past two decades, great strides have been made in the context of breastfeeding promotion, protection, and support through implementation of the Baby-Friendly Hospital Initiative and surveillance methods, for example. 53 Despite this, racial disparities persist suggesting that all U.S. families are not sharing the benefits of expanded breastfeeding promotion efforts. The COVID-19 pandemic demonstrated that any social progress for Black women is easily reversed and/or erased. Black women of all education levels were negatively impacted by the pandemic. 54 Research has demonstrated that without targeting underlying causes of disparities such as racism, mechanisms of social exclusion tend to adjust to maintain the oppressive relationship 14 ; thus, it is not realistic to believe that social forces have changed for the better. Findings from these historical data strengthen our understanding of “place” as a critical condition allowing families to thrive through breastfeeding.
The data reported herein contribute to the identification of the long-standing issue of racism and breastfeeding outcomes. Our findings fill a gap in an explanatory chain beginning with a historical insult that lives on in breastfeeding rates in the present day.
Conclusion
Breastfeeding and lactation have health implications over the life course for both women and children and are therefore critical to achieving health equity. These findings demonstrate that “place” and opportunities for optimal health through breastfeeding are inextricably linked. Further research is needed to understand the limitations and strengths of mechanisms by which neighborhood-level factors influence breastfeeding initiation and duration for Black women in the United States.
Footnotes
Acknowledgments
M.K.G. would like to acknowledge Dr. Donna Perry, PhD, RN, for her contribution to the original study and Natalie Schriefer, MFA, for her assistance with formatting. The authors thank the participants and staff of the BWHS for their contributions.
Authors’ Contributions
M.K.G.: Conceptualization, methodology, formal analysis, and writing—original draft. S.L.C.: Methodology, formal analysis, writing—review and editing, and visualization. S.D.P.: Methodology and writing—review and editing. L.R.: Methodology, data collection, and writing—review and editing. J.R.P.: Methodology, data collection, and writing—review and editing. Y.C.C.: Methodology, data collection, writing—review and editing, and visualization.
Disclaimer
The content presented is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Disclosure Statement
The authors have no conflicts of interest to report.
Funding Statement
This work was supported by the National Institutes of Health (UM1CA164974, U01CA164974, and R01CA058420) (J.R.P., Y.C.C., L.R.).