
Abstract
Objective:
Olfactory stimulation can be used for many purposes, such as providing comfort, improving sleep, and reducing pain in newborns. However, there are only a few studies in the literature examining the effect of olfactory stimulation on newborn growth. The aim of this study was to evaluate the effect of olfactory stimulation on growth parameters of newborns.
Method:
This systematic review used the PRISMA checklist. No date limitation was applied, and all studies were considered for inclusion. Pubmed, Web of Science, Scopus, and Medline databases were used for the search.
Results:
A total of 367 publications were found in the search. Eight studies that met the inclusion criteria were included in the study. The olfactory stimulations applied were maternal odor, maternal milk odor, cinnamon, aniseed, vanilla, and formula milk odors. Olfactory stimulation was found to have a positive effect on the weight gain of newborns in three of the eight studies, and maternal odor and maternal milk odor were used in these studies. In two of the three studies evaluating the effect of maternal odor and maternal milk olfactory stimulation on the height of newborns, the result was found to be significant. The effect of maternal milk olfactory stimulation on head circumference was found to be significant in one of the two studies.
Conclusion and Recommendation:
Maternal odorand maternal milk odor may have a positive effect on newborn growth parameters. Further studies on this subject are needed.
Introductıon
The neonatal period covers the first 28 days following birth. Body weight and weight gain rate, height and growth rate, head circumference, and head circumference growth rate are among the criteria used to evaluate growth in the neonatal period. 1 The use of developmental care practices in the care of newborn infants positively affects the physical development of the infant. 2 Developmental care practices include involving parents in care, positioning, swaddling, non-nutritive sucking, cyclic lighting, and noise prevention. 3 Olfactory stimulation is another application used in developmental care.
Olfactory receptors begin to form in the intrauterine period. 4 The olfactory bulbs can be identified by magnetic resonance from 28 to 30 weeks of gestation. 5 Newborns can perceive odors and discriminate and remember them.6,7 The sense of smell is also essential for feeding and attachment. 8 Many studies and systematic reviews have been conducted on maternal milkodor and aromatherapy in recent years. These studies have found that familiar and pleasant odors in newborns are calming, reduce pain, increase sucking movements, and facilitate the transition to oral feeding.9–11 These odors have also been proven to reduce the length of hospital stay and interventional pain of newborns, significantly reduce apnea, and improve SpO2 levels.9,10,12 However, there are few randomized controlled studies in the literature evaluating the effect of olfactory stimulation on the growth parameters of newborns.There is also a systematic review examining the effect of odor on body weight. This systematic review concluded that odor stimulation was not effective on weight gain and that further studies are needed. 13 However, no systematic review evaluating the effect of odor on all growth parameters was found in the literature. This systematic review aimed to examine the studies evaluating the effect of olfactory stimulation on growth parameters in the newborn.
Methods
It is recommended to use PRISMA to ensure international standards when reporting systematic reviews or meta-analyses. 14 This systematic review was conducted in accordance with the PRISMA method.
Selection of studies (selection process and data extraction)
The searches using keywords reached a total of 367 studies (Table 1). Of the studies, 147 were excluded from the systematic review because they were repetitive, 209 were excluded because they did not evaluate the effect on growth parameters, 2 were excluded because they were systematic reviews, and 1 was excluded because it was written in a language other than English. The systematic review was completed with eight studies (Fig. 1).
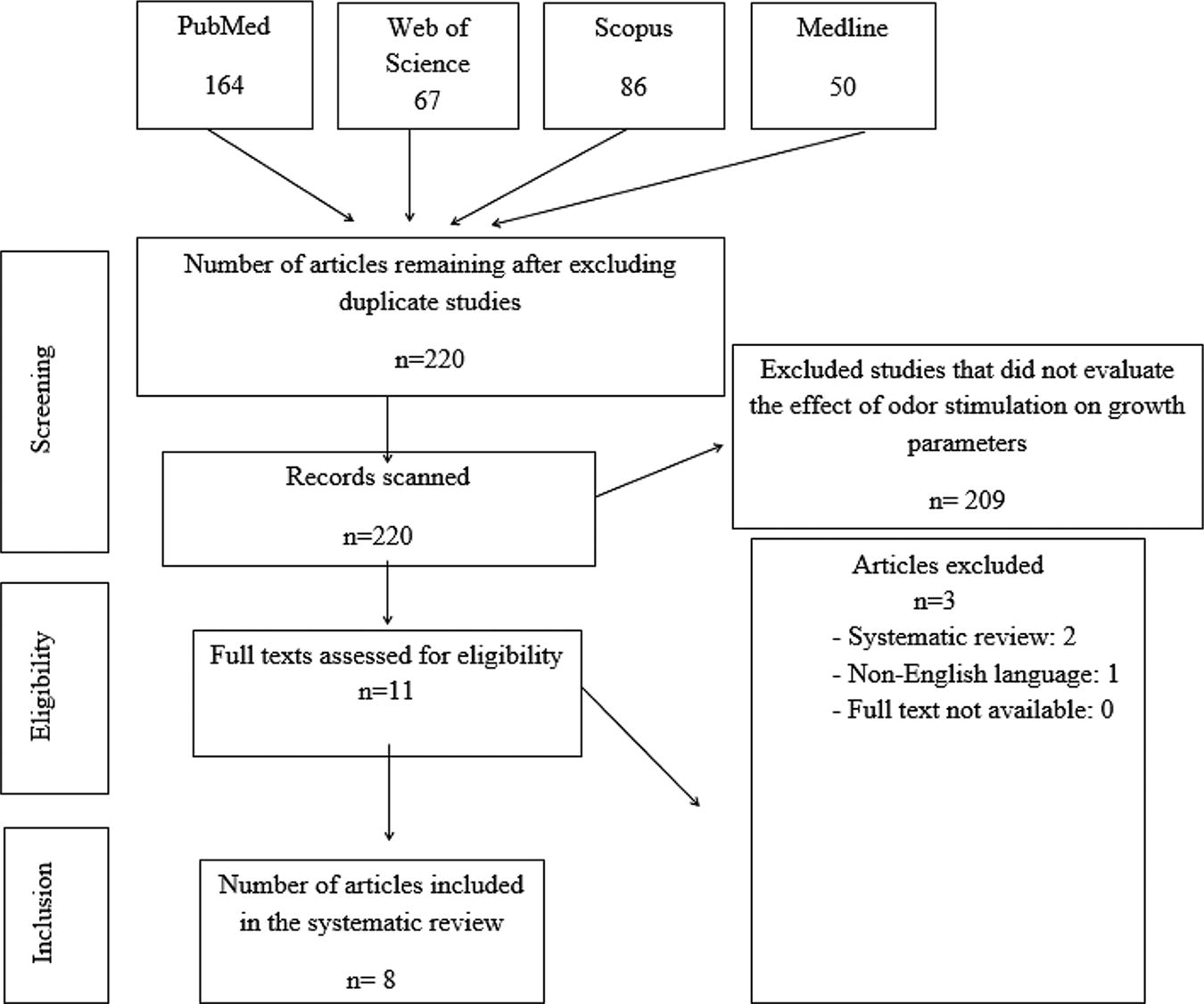
Study flow chart in line with the PRISMA method.
Keywords and Writing Styles Used by Databases
Search Strategy
The search was carried out in Pubmed, Web of Science, Medline, and Scopus databases between February 1, 2024 and March 1, 2024. No time limitation was imposed in the study, and all studies that could be accessed were included in the review. The keywords and writing styles used in the search are given in Table 1.
Inclusion Criteria
The studies included in the systematic review were selected according to the PICOS components: P: population, I: interventions, C: Comparators, O: Outcomes and S: Study design.
P: Population: Preterm and term newborns
I: Interventions: Olfactory stimulation
C: Comparators: Newborns receiving and not receiving olfactory stimulation
O: Outcomes: Growth parameters
S: Study designs: Experimental or quasi-experimental studies
Thus, the following studies were included:
Experimental or semi-experimental studies Studies examining the effect of olfactory stimulation on growth parameters in newborns Published studies in the English language Studies with full texts available
Bias risk
Searches and quality assessments of the eligible studies identified by the searches were carried out independently by three researchers. All three researchers selected the same studies for the systematic review.
Quality assessment
The methodological quality of the studies included in the systematic review was independently assessed by three researchers according to the “Revised JBI Critical Appraisal Tool for Assessing the Risk of Bias in Randomized Controlled Trials” published by the Joanna Briggs Institute. The assessment tool consists of 13 items. Each item is rated as yes, no, unclear, or not applicable. JBI critical appraisal tool score varies between 0 and 13. The higher the total score of the studies, the higher the methodological quality. 15 The scores the three researchers gave were compared, and they were the same.
Results
Eight studies were included in the systematic review.
Details of the studies
All of the studies were randomized controlled trials.16–23 The sample sizes of the studies vary between 32 and 334 people. Seven studies included preterm newborns,17–23 and one study included term newborns. 16 All of the studies (eight studies) evaluated the effect of olfactory stimulation on weight, three evaluated its impact on length,18,21,23 and two evaluated its effect on head circumference.18,23 Maternal milk odor was assessed in four studies,17,18,22,23 maternal odor in two,16,21 cinnamon and aniseed odor in one, 19 and vanilla and milk (maternal milk or formula) odor in one. 20 The characteristics of the studies included in the systematic review are given in Table 2.
Characteristics of the Studies İncluded in the Review
Randomized controlled trial.
Intervention details used in the studies ıncluded in the review
Kardaş Özdemir and Güdücü Tüfekçi 21 included preterm newborns with a gestational age of ≤36weeks, weighing ≥1,000 g, and not being breastfed in their study conducted in a neonatal intensive care unit in Kars city in Turkey. The included preterm newborns were divided into three groups by random assignment method. The first group was the control group, the second was the flexion group, and the third was the maternal odor group. The infants in the control group received routine nursing care and were followed up simultaneously with the infants in the experimental groups until discharge. The infants in the flexion group were positioned using BendyBumper positioning material placed under the hips and feet and on the side of the shoulders in a “U” shape, changing the position of the infant at each feeding time. This was continued until the infant was discharged. The mother of each infant in the maternal odor group was given an Oookie doll with odor-absorbent properties and asked to keep the Oookie doll on her breast overnight (approximately 8 hours), touching her bare skin. The next day, the Oookie doll was placed in the neonatal incubator. Oookie dolls were kept in the incubator for 24 hours and changed every day at 09:00, the first hour of care. This continued until the discharge of preterm newborns.
Beker et al. 17 included preterm newborns born younger than 29 weeks in their study. The infants in the intervention group smelled and tasted breast milk during each tube feeding. The odor was provided by placing a drop of milk on a gauze pad placed as close as possible to the infant’s nose without touching the infant. For taste intervention, a cotton swab dipped in milk was held to the infant’s lips, and if the infant demonstrated interest, a very small amount of milk (cotton swab or syringe) was given into the infant’s mouth. Infants in the control group received routine care. All infants were followed up until discharge.
The study of Cao Van et al. 19 in a neonatal intensive care unit in Brussels included preterm infants fed with a probe. The included infants were divided into two groups by single-blind randomization. In the experimental group, olfactory stimulation was performed by placing pen-shaped odor sticks called “Sniffin’ Sticks” close to the infant’s nose before feeding. Of the 25 infants in the experimental group, 12 were stimulated with cinnamon and 13 with aniseed. In the control group, odorless sticks were used. All infants were followed up until discharge.
Khodagholiet al. 22 studied newborns with a gestational age of 28–32 weeks in two neonatal intensive care units in Tehran, Iran. The infants were randomly assigned to two groups: control and intervention. Infants in the control group received non-nutritive sucking intervention during probe feeding, while infants in the experimental group received both non-nutritive sucking and maternal milk odor intervention during probe feeding. Non-nutritive sucking intervention was performed by wearing latex gloves and tapping the little finger lightly on the palate of the infant. Maternal milk odor intervention was performed by placing cotton pads soaked with breast milk taken from the infant’s mother ∼2–3 cm away from the infant’s nose. In the intervention group, both stimulations were given simultaneously in the first 5 minutes of probe feeding during three consecutive feedings each day for 10 consecutive days. In the control group, non-feeding suction intervention was given at the same timing and frequency.
The sample of the study conducted by Küçük Alemdar and İnal 23 in a neonatal intensive care unit in Giresun, Turkey, consisted of preterm newborns weighing >1,000 g and for > 34 weeks. Preterm newborns were randomly assigned to four groups. In the breast milk odor group, the intervention was performed by pouring the milk taken from the mothers of the infants into a sponge and placing it 5 cm away from the infant. This intervention was applied once a day and continued until the infant switched to oral feeding. The mothers’ voices of the infants in the mother’s voice group were recorded, and this recording was played three times a day for 30 minutes at 45 dB while the newborn was awake. The incubators of the infants in the incubator protection group were covered with a special thick white cloth and followed up in this way until the infant was switched to oral feeding. Preterm infants in the control group received only routine nursing care.
Beker et al. 18 included preterm newborns <29 weeks old in their study conducted in Australia. The infants were randomly assigned to the intervention or control group. Infants in the intervention group smelled and tasted milk during each tube feeding. The odor was provided by placing a drop of milk on a gauze pad placed as close as possible to the infant’s nose without touching the infant. This intervention was stopped when the infants reached 32 weeks. For taste intervention, a cotton swab dipped in milk was held to the infant’s lips, and if the infant demonstrated interest, a very small amount of milk (cotton swab or syringe) was given into the infant’s mouth. To provide odor and taste intervention, the same milk was used as the milk the infant received through the tube (expressed breast milk, donor breast milk, or formula milk). Infants in the control group received routine care. All infants were followed up until discharge.
The sample of the study conducted by Akkoca et al. 16 in Eskişehir, Turkey, in 2022 consisted of newborns >37 weeks of gestation. The infants included in the study were divided into two groups as experimental and control groups. Mothers of the infants in the maternal odor group were given breast pads and asked to keep the pads on their breasts for 3 hours without touching the nipples. Mothers replaced the pads with new pads every 3 hours. The pads taken from the mothers were placed in the incubator 10 cm away from the infant’s nose. The pads were replaced with new pads given by the mothers every 3 hours. The infants in the control group did not receive any odor intervention.
Gellrich et al. 20 included preterm infants >26 + 6 weeks of gestation in their study conducted in 2024. The infants included in the study were randomly divided into three study groups. In the vanilla group, odor intervention was performed before each feeding by means of felt-tip pens filled with an odorant called “Sniffin’ Sticks.” In the control group, odorless sticks were used. For odor presentation, the cap of the “Sniffin’ Sticks” was removed by the nurse, and the tip of the pen was placed ∼2 cm below the nostrils of the infants for ∼10 seconds. For the milk odor group, sterile packaged cotton swabs were soaked in milk and then placed ∼2 cm below the infants’ nostrils for 10 seconds. For the milk odor group, maternal milk, donor breast milk, or formula milk was used if the mother did not have her own breast milk. This was repeated before each feeding. The infants were followed up until discharge.
Results of growth parameters of the studies ıncluded in the research
Olfactory stimulation positively affected newborns’ weight gain in only three of the eight included studies. In the study by Kardaş Özdemir and Güdücü Tüfekçi, 21 maternal odor increased the mean weight at discharge. In the study by Beker et al., 17 maternal milk olfactory stimulation affected the weight z score at discharge. Akkoca et al. 16 found a statistically significant difference between the mean weight measurements of the newborns in the group exposed to maternal odor on the day of admission and the mean weight measurements on the first and second day after the intervention, while there was no significant difference in the control group.
Among the studies included in the systematic review, three evaluated the effect of olfactory stimulation on height in newborns. Kardaş Özdemir and Güdücü Tüfekçi 21 reported that maternal odor increased the height at discharge in their study, while Küçük Alemdar and İnal 23 indicated that maternal milk odor had no effect on the height at discharge in their study. In the study conducted by Beker et al. 18 with milk odor, there was a significant difference in favor of the experimental group at 36 weeks of gestation in terms of height z scores of newborn infants, while no significant difference was found at discharge.
Two of the studies included in the systematic review evaluated the effect of olfactory stimulation on head circumference length in newborn infants. Küçük Alemdar and İnal 23 reported that maternal milk odor had no effect on the head circumference at discharge. Beker et al. 18 found that milk odor increased the head circumference of newborn infants when they reached 36 weeks of gestational age but had no significant effect at discharge.
Dıscussıon
Odor receptors are functional in the fetus, and there is evidence that odors are learned prenatally. 4 The discrimination of odorous molecules occurs in the amniotic fluid after 28–30 weeks of gestation, and olfactory bulbs can be identified by magnetic resonance at these weeks. 5 It is known that newborn infants can perceive, distinguish, and remember different odors.6,7 Preterm newborns are also capable of responding to a wide variety of odor stimuli, distinguishing odors of different qualities and intensities, memorizing the stimuli to which they are regularly exposed, and categorizing different odors despite their immaturity. 24 Studies have shown that newborn infants are oriented toward maternal odor and amniotic fluid odor, which are familiar odors for them.25,26 In another study, newborn infants gave oral responses to colostrum odor. 27 In other studies, oxyhemoglobin values increased in the frontal region as a result of exposure of newborn infants to vanilla, colostrum odor, and maternal milk odor.28,29 In a systematic review conducted by Khakpour et al. 10 to evaluate the relationship between olfactory stimulation and feeding, maternal milk odor accelerated the transition to full enteral feeding and improved feeding behaviors of infants. Thus, this systematic review aimed to examine the effect of olfactory stimulation on growth factors in newborn infants.
According to our systematic review, olfactory stimulation had a positive effect on weight gain in only three out of eight articles. The difference found in a small number of studies may be associated with the use of different odors because the odors the studies used and found effective were maternal odor and maternal milk odor. The systematic review by Tafrishi et al. 13 investigating the relationship between olfactory stimulation and weight gain in preterm infants concluded that olfactory stimulation was not effective on weight gain and that more studies were needed. As a result of the current systematic review, it can be said that odors such as cinnamon, aniseed, vanilla, and formula do not affect weight gain, whereas maternal odor and maternal milk odor may affect weight gain. However, due to the very limited number of studies conducted on this topic, it is not possible to make a definitive statement about the effect of olfactory stimulation on weight gain. Therefore, there is a need for more studies examining the effect of odors on weight gain.
In the literature, no systematic review has been found that examines the effect of olfactory stimulation on other growth parameters, such as height and head circumference. The effect of olfactory stimulation on height was examined in three of the articles we examined in the systematic review, and it was effective in two of them. One article examining the effect of maternal odor on height was found, reporting that maternal odor improved height in newborns. One article was found examining the impact of maternal milkodor on height. In one of these studies, there was a significant difference in favor of the experimental group in terms of height z scores at 36 weeks gestational age of newborns, but no significant difference was found at discharge. In another study that examined the effect of milk odor on height, it was found to be ineffective. The number of studies conducted seems to be low, and there is a need for further research on this subject.
The effect of olfactory stimulation on head circumference was examined in two of the studies included in the review. The odors used in these studies were breast milk and milk odor. In the study in which milk odor was applied, there was a significant difference in favor of the experimental group in terms of head circumference when the newborns reached 36 weeks of gestation, but no significant difference was found at discharge. In the other study, maternal milkodor was not found to be effective on head circumference. The very limited number of studies and the fact that these studies have only used maternal milk odor indicate a need for more studies examining the effects of different odors on infants’ head circumference.
Environmental and social stimuli in the neonatal intensive care unit cause the baby to consume more energy. This may adversely affect their growth and development. Developmental care approaches aim to minimize energy use and store it to be used for growth and development as much as possible.30–31 Odor stimulation is one of the approaches used in developmental care. The results of the review showed that maternal odor and maternal milk odor may positively affect the growth parameters of infants. However, the fact that other odors were not found to be effective on growth parameters does not necessarily mean that these odors are not useful. For example, in one of the studies included in the review, there was no difference in weight between the vanilla odor group and the maternal milk odor group. However, the amount of milk consumed by the infants in the vanilla group was significantly higher than the infants in the breast milk group. 20 With the current limited literature, it is still difficult to make a judgement on the mechanism by which odors affect growth parameters. Further studies on this subject are needed.
Limitations of the study
The review included studies written in the English language. Some studies may have been missed due to the selection or spelling of keywords.
Conclusıon
Different olfactory stimulations were used in the studies included in the review. Among these odors, maternal odor and maternal milk odor were found to have an effect on infant growth parameters. Odors such as vanilla, aniseed, and cinnamon had no effect on growth parameters. However, this study has shown that there are very few studies in the literature that evaluate the effects of olfactory stimulation on growth parameters. Therefore, it is not possible to make a definite conclusion about the effect of these odors. It is recommended that new studies be conducted to investigate the effects of olfactory stimulation on growth parameters, which are crucial indicators of newborn health. Effective odors identified in these studies could be incorporated into nurses’ daily care routines to support infants’ growth.
Footnotes
Authors’ Contributions
O.B.: Conceptualization, methodology, formal analysis, data curation, writing—original draft, writing—review and editing, and visualization. A.A.: Conceptualization, methodology, formal analysis, data curation, writing—review and editing, and supervision. M.C. conceptualization, methodology, formal analysis, data curation, writing—original draft, and writing—review and editing.
Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.